Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
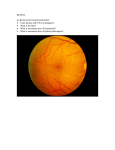
Case Report: Peripapillary Subretinal Neovascular Membranes By David Meyer, OD Primary Care Resident, Salt Lake City VA Hospital Abstract This case report describes the etiology, treatment, management, and importance of peripapillary subretinal neovascular membranes (PSRNVMs). PSRNVMs are uncommon networks of abnormal choroidal blood vessels that occur within one disc diameter of the optic nerve. Case History A 90 year-old Caucasian male presented to the Salt Lake VA hospital for a primary care eye exam. His chief compliant was dry eyes. Significant ocular history included dry ARMD, cataracts, and dry eye. His current medication included amlodipine, hydrochlorothiazide, lisninopril, terazosin and warfarin. The patient was taking warfarin because of previous atrial fibrillation and stated compliance with his medication regimen. The patient also had a history of a hemicolectomy, hypertension, iron-deficiency anemia, BPH, and knee pain. The patient also mentioned that he felt like his vision had decreased somewhat since his exam the year before. Pertinent Findings The patient was refracted and the following visual acuities were obtained: OD: 20/50- OS: 20/30-. Biomicroscopy revealed dry eye, arcus, and 2+ nuclear sclerotic cataracts which likely contributed to his decreased vision. The patient was then dilated as part of the routine exam. Upon examination of the fundus, a large peripapillary hemorrhage was found in the right eye. The hemorrhage extended from the 7:00 to 11:00 portions of the temporal optic nerve head with an inner zone directly adjacent to the nerve that appeared to be lighter than the deep-red surrounding blood. The hemorrhage extended 1DD temporally with well-defined borders. The optic disc did not appear edematous. Confluent macular soft drusen was also noted. No other posterior segment abnormalities were seen in the right eye. The left eye examination revealed a group of exudates superior temporal to the optic nerve head (ONH). The area temporal to the ONH including the exudates appeared to be slightly elevated in comparison to the temporal ONH margin. Near the area of elevation the blood vessels had a very wispy appearance. Like the right eye, the macula had confluent macular drusen. Both ONHs had shallow cupping and c/d ratios of 0.20 round. Fundus photos were taken and images from the Spectralis OCT were obtained. Interestingly, the average-thickness evaluation map on the OCT revealed much more elevation in the non-hemorrhagic left eye. The cross-sectional views confirmed this elevation by showing a large separation between the neurosensory layer and the RPE layer. The macular scans displayed an uneven surface at the RPE which confirmed the appearance of drusen. At this point, the patient was scheduled to be seen in the retinal clinic the following week. He was strongly cautioned against head trauma, excessive lifting or bending, and to not take his medications more than what was prescribed. Differential Diagnosis The primary differential diagnosis in this case was hemorrhagic peripapillary subretinal neovascular membrane (PSRNVM) from exudative ARMD. Other differential diagnoses included polypoidal choroidal vasculopathy, traumatic choroidal rupture, hemorrhage from optic nerve drusen, choroidal tumor, CNVM from ocular histoplasmosis, and idiopathic etiology. Diagnosis During the following week the patient returned to our clinic for fluorescein angiography (FANG). FANG was completed without complication and revealed a hypofluorescent hemorrhage temporal to the ONH in the right eye. The hemorrhage partially obscured a hyperfluorescent network of blood vessels which correlated to the lighter area noted previously. The pattern was consistent with CNVM leakage. The network of blood vessels remained hyperfluoresced throughout the mid and late phases of the procedure. The left eye showed no leakage in the peripapillary region, although patches of indistinct mild hyperfluorescence were observed. The patient was sent to the retinal clinic to be further evaluated. The attending ophthalmologist confirmed the primary diagnosis of PSRNVM secondary to wet ARMD OD. A Lucentis injection in the right eye was performed that day to the patient without complication. Despite the peripapillary elevation in the left eye caused by subretinal fluid on OCT, a PSRNVM was not found. Based on the stability of the vision of the left eye and the lack of a definitive diagnosis, close observation was recommended. The patient was to return in 4 weeks for a follow-up exam which included a second injection of Lucentis OD. To date, 3 total injections will be completed. Discussion Peripapillary subretinal neovascular membranes (PSRNVMs) are relatively uncommon findings which occur within 1 disc diameter of the disc border, with no normal retina separating the membrane from the edge of the disc1. They are associated with a number of conditions, including ARMD, multifocal choroiditis, histoplasmosis, congenital disc anomaly, pattern dystrophy, angioid streaks, optic disk drusen, choroidal osteoma, peripapillary pseudopodal pigment choroidal atrophy, and can be idiopathic2. ARMD is the most common association at around 45%. PSRNVMs can cause decreased vision because of subretinal fluid, exudates, or hemorrhage that extends toward or into the fovea, even when the neovascular membrane is far from the macula 3. Second-eye involvement of PSRNVMs occur in about 20% of patients after the median time of 2 months2. The FANG appearance shows that the majority of them are of the occult-type. Recent research reveals that the vast majority of occult-type PSRNVMs may actually be polypoidal choroidal vasculopathy masquerading as PSRNVM4. This recent evidence emphasizes the importance of indocyanine green angiogram to differentiate the two entities. ARMD-associated PSRNVMs are unique in that most patients do not present with macular drusen2. The clinical characteristics most associated with PSRNVMs were hemorrhage, exudates, fibrosis, and peripapillary atrophy4. These findings are extremely important to the clinician while examining at-risk patients. Treatment and Management PSRNVMs are treated in a variety of ways including laser photocoagulation, photodynamic therapy, transpupillary thermotherapy, and intravitreal anti-VEGF injection3. Photocoagulation has shown very positive results5, but recurrence rate is still an issue with this type of therapy3. Currently the most promising treatment is anti-VEGF injection. Studies show that up to 87.5% of eyes show stabilized or improved vision using this modality6, although specific studies involving PSRNVMs exclusively have not been performed. Typically, treatment is begun in order to prevent foveal involvement. Therefore, treatment is indicated when the PSRNVMs occur temporal to the disc, there is a threat to the macula, and, if using laser photocoagulation, at least 1.5 clock hours adjacent to the temporal ONH can be spared of the laser2. Conclusion PSRNVMs are atypical presentations of subretinal neovascularization that warrant careful observation and/or immediate treatment. They are related to a number of other ocular conditions, and further research is needed to shed more light on the best treatment and management strategies. Due to the relatively high incidence of second-eye involvement, careful observation of the fundus along with OCT analysis are indicated for both eyes. The patient presented in this case report is a very good example of the importance of close observation. FANG is always indicated in suspicious cases, and indocyanine green angiogram is emerging as a near-necessity, especially if the neovascular membrane is the occult type. Overall, visual prognosis is fairly good for those membranes that are treated properly and do not affect the fovea. Bibliography 1. Lopez PF, Green WR. Peripapillary subretinal neovascularization: a review. Retina 1992;12:147-171. 2. Browning DJ, Christina FM. Ocular conditions associated with peripapillary subretinal neovascularization, their relative frequencies, and associated outcomes. Ophthalmology 2005;112:1054-1061. 3. Kokame GT, Yamamoka S. Subretinal surgery for peripapillary subretinal neovascular membranes. Retina 2005;25:564-569. 4. Squirrell DM, Bacon JF, Brand CS. To investigate the prevalence of polypoidal choroidal vasculopathy in presumed age-related peripapillary subretinal neovascular membranes. Clinical and experimental ophthalmology 2009;37:368-372. 5. Turcotte P, Maguire MG, Fine SL. Visual results after laser treatment for peripapillary choroidal neovascular membranes. Retina 1991;11:295-300. 6. Eyetech Study Group. Anti-vascular endothelial groth factor therapy for subfoveal choroidal neovascularization secondary to age-related macular degeneration: phase II study results. Ophthalmology 2003;110:879-881.