Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
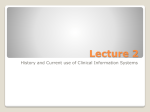
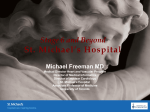
Section 2.2 Utilize – Effective Use Optimization Strategies for CPOE and e-Prescribing Use this tool is to distinguish between computerized provider order entry (CPOE) and e-prescribing. It describes various strategies for implementing these two similar applications. Instructions for Use 1. Determine whether you are focused on CPOE for the hospital or physician office/clinic environment. While you may need interoperability between the settings, their CPOE systems are different, especially where the office/clinic is completely separate from the hospital. As a unique aspect of CPOE, e-prescribing needs to be addressed separately. 2. If you have not done so already, engage all stakeholders in the process of implementation. While the predominant users of CPOE are providers, all managers in departments that receive orders need to be involved. Nurses also need to understanding their new roles with respect to CPOE and in managing refills via e-prescribing. Determining the extent to which ancillary department systems are available and ready to receive orders is essential. You must consider many aspects for rolling out CPOE. 3. Conduct workflow and process improvement mapping to determine how the application being implemented may change current workflows and processes. Ideally, you have already mapped, in detail, current workflows and processes and can now identify processes you want to include in the new application and how improvements can be made. These should relate to your overall goals for CPOE. Standardization will be needed. Providers may find some processes intended to support patient safety and care management seem foreign when they are performed on a computer. 4. Provide the opportunity for all physicians, nurses, and others to be fully trained. As with electronic medication administration records (EMAR), pharmacist involvement is especially critical. Engage laboratory staff to assure timeliness of laboratory test performance. Depending on the nature of the departmental systems currently in place, staff will be alerted in new ways to incoming orders or you may need to create workarounds for older departmental systems. 5. Monitor usage after go live. CPOE and e-prescribing have many associated issues, including the length of time it takes to enter an order, alert fatigue, keeping the drug knowledge base and formulary for e-prescribing up to date, training new or infrequent users, and monitoring the achievement of goals. CPOE and e-Prescribing CPOE enables providers to enter orders for medications, diagnostic studies, imaging studies, therapeutic services, nutrition and food services, nursing services, and other orderables; and be supplied clinical decision support that has many patient safety and other benefits. The extent to which orders are placed for services depends on the nature of the health care delivery services. A CPOE system in the hospital environment is typically either a module or component of an integrated hospital information system or electronic health record (EHR) or a standalone system that is interfaced or integrated through a clinical data repository (1.1 Visioning and Strategic Planning). Physician offices or clinics do not have modules called CPOE, but have a similar functionality embedded in their EHR. Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 1 With respect to medication management, the differences between CPOE and e-prescribing are important to appreciate. In a hospital, the CPOE connects with the pharmacy and nursing services to place orders and receive reminders and alerts, as well as provide access to clinical practice guidance. In an outpatient department, clinic, or other area where a prescription needs to be written (e.g., when sending a patient home from the emergency department or on discharge from a hospital), e-prescribing supports the provider with reminders and alerts and access to guidance, as well as enables checking against a health plan formulary and transmission of the prescription directly to the retail or mail order pharmacy of the patient’s choice. A key difference between CPOE and e-prescribing (other than that e-prescribing is limited to the ordering of drugs via a prescription) is that CPOE is used within a hospital (or long term care or other facility with an internal, clinical pharmacy where most drug costs are generally covered by the patient’s health plan) and e-prescribing is used to communicate with retail pharmacies (and where the patient’s health plan may have strict benefits rules and formularies). The illustration below depicts the process of communicating between a physician’s e-prescribing (e-Rx) system to a retail pharmacy, using an e-prescribing gateway. Such gateways are companies that provide secure routing. The largest is Surescripts. E-prescribing Communication Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 2 E-prescribing is a relatively new process. All pharmacies serving Medicare Part D patients were required to accept e-prescribing transactions by 2009. At the end of 2007, bills were introduced into Congress to require all prescriptions to be written electronically. Also by the end of 2007, over 95 percent of retail pharmacy chains were certified to receive prescription transactions through an eprescribing gateway (even though some of the local stores within those chains may not have fully been trained on using that functionality in their systems). However, by the end of 2007, adoption by physicians was estimated to be only at about five percent, although rapidly rising. During 2007, many Blues plans and some other insurance companies were giving physicians e-prescribing systems with the hope of reducing brand name drug usage to reduce cost. Some issues still need to be addressed in e-prescribing. One that particularly impacts small and rural communities is that pharmacies that are not members of large chains generally have not certified with Surescripts or another gateway. Although the e-prescribing gateway companies convert such prescriptions to a fax, part of the overall benefit of reducing transcription errors at the pharmacy is lost. It also impacts the pharmacies workflow because they now have faxes coming in where patients may not come the same day (or ever) to pick up their medications. The Drug Enforcement Administration (DEA) does not permit electronic prescriptions for controlled substances. Although physicians can still use their e-prescribing system for reminders and alerts and to generate a printed prescription to reduce legibility errors, they must provide the patient a paper prescription with a wet signature to take to the pharmacy. State boards of pharmacies may have more stringent requirements, including information that must be printed on the form, such as a check box for generic substitution, form stock to be used, printer security, and reporting of prescriptions for Schedule II drugs. For the 15 percent of all prescriptions written in the US for controlled substances, you need a workaround until the DEA and the Department of Health and Human Services can come to agreement on what form of electronic signature can be permitted Although not a part of the e-prescribing gateway per se, the ability for physicians’ e-prescribing systems to connect to drug knowledge databases and patients’ health plan formulary information (through a PBM consolidator, such as RxHub) are critical elements for the increasing popularity of eprescribing. In addition to these observable differences, the standard communication protocols used to communicate between the ordering application and the pharmacy destination are different. CPOE systems are written to conform to HL7 standards that are used to communicate with the clinical pharmacy information system, laboratory information system, etc. E-prescribing systems are written to conform to the National Council for Prescription Drug Programs (NCPDP) standards that have been used for many years by retail pharmacies for formulary checking and claims processing. The NCPDP SCRIPT standard has been recognized by the Federal government as the official standard for use in e-prescribing, since HL7 does not have an equivalent standard. Today, a provider in a hospital is unable to use the CPOE system to write and transmit a prescription to be filled by a retail pharmacy (shown by a dotted line in the diagram below). The provider in the clinic (or upon discharge, in the emergency department, or in an outpatient department) using an e-prescribing system is unable to write a medication order for the hospital’s clinical pharmacy (shown by the dotted lines). HL7 and NCPDP are working on harmonizing their standards and this may change in the future. Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 3 The NCPDP SCRIPT standard enables a number of functions to be performed. In addition to being able to transmit a prescription through an e-prescribing gateway directly into the retail pharmacy’s information system, the SCRIPT standard enables electronic communication with the retail pharmacy. For example, if the prescriber has not checked the health plan formulary, the dispenser will do so and can notify the prescriber that a drug prescribed is off formulary via a change notification. The prescriber can respond back electronically with approval for a change—eliminating telephone tag. If a prescription requires prior authorization, the dispenser can notify the prescriber of this. In the near future, the prescriber will be able to obtain the prior authorization in an electronic communication with the health plan or pharmacy benefits manager (PBM). The prescriber can also issue a cancel notification. Although not widely used at this time, the dispenser can supply the prescriber with a fill status notification—alerting the prescriber when the prescription was filled, partially filled, or not filled after a certain period of time. Some prescribers appreciate getting this information and perform follow up with their patients; others prefer not to receive this information. A tremendous amount of time can be saved by the automated refill process enabled by e-prescribing. Some clinics report that as much as 40 percent of a nurse’s time is devoted to this process, almost all of which can be saved by automated notification; rule adherence; routing within the office or clinic; access to documentation in the EHR, including recent lab and other information; and renewal functionality. The following illustrates the nature of the e-prescribing functions. Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 4 e-Prescribing Systems Several different types of e-prescribing systems are available. The three main types are: Drug knowledge reference systems. These are not technically e-prescribing systems because they do not generate a prescription at all, but provide access to a drug knowledge database. As many as 60 percent or more of physicians use such tools. The most popular is Epocrates, which offers a basic free version downloadable from the Internet to a PDA. The drug knowledge database must be updated regularly, requiring an Internet connection, and PDA devices require regular battery recharging. Standalone e-prescribing systems. These systems incorporate a drug knowledge database and generate a prescription. Levels of functionality vary. For example, some only generate a legible prescription form while others connect to an e-prescribing gateway, via a secure Internet connection. Even the most sophisticated standalone system does not have a central database from which to draw patient demographics, past medication history, or share prescription information with other providers in the group. Although the more sophisticated standalone systems retain patient demographic and prescription information, all initial entries must be made from scratch. E-prescribing systems that are part of an EHR not only have their own functionality, but also can draw from the her. They can automatically incorporate patient demographics, prescription information can be shared with whoever has access to the EHR, and more decision support is available (e.g., lab values can be evaluated against drug rules to alert a provider ordering a medication that would be impacted by the patient’s poor renal functional). Such e-prescribing systems make it easier for managing refills, prescription changes, and other tasks. Even though this is the most sophisticated level of e-prescribing, not all EHR/e-prescribing systems include all possible functionality. For drug-lab checking, the EHR must be interfaced with a laboratory information system that generates discrete lab values. Some physicians also do not want to spend the money to subscribe to a formulary information service or believe it is not their role to discuss the cost of the drug with their patients, although health plans are encouraging this discussion in order to achieve greater compliance with patients for their treatment regimens. Hospital Implementation of CPOE Critical success factors for implementing CPOE in a hospital include the following: □ Engaging physicians. Nearly every paper or news article written about CPOE stresses the importance of physician engagement in selecting and implementing CPOE, but many hospitals wait to do so until training is necessary. Physician orders is one of the most fundamental and important parts of a physician’s practice. If a system is seen as not supporting this function, it will not be accepted. Many physicians view CPOE, at least initially, as a means for the hospital to relieve their staff from clerical work, not as a means to support clinical decision making or improve patient safety, let alone to improve physician productivity (which it will not do at the beginning, and in the end may only bring them to parity with respect to time). Physicians must come to understand and trust the CPOE system, believe they are a part of developing the clinical decision support rules, and see their role in selecting a system that is the most user-friendly. Getting physicians to the table to begin with is very difficult. Gain physician involvement by: Indicating that the hospital has specific plans to move to a CPOE system by date certain and want the physician engaged from day one. This puts the physicians on notice that the hospital is serious and gives them ample time to participate. If you fear that physicians will leave, know that the physicians are not likely to find many other places that not moving toward more automation. Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 5 Providing non-monetary incentives for physicians to participate. For example, offer remote access to the system as a means to reduce the burden of verbal order signing. State benefits in a manner that is give and take, recognizing the value to both parties. Ask physicians to participate in measurable goal setting so they can influence the measures, scenario development so they are responsible for assessing the products, standing order development to build their own order templates, and review of the clinical effectiveness and efficiency with using the decision support rules. To make this work for them, start adopting the standing orders as soon as they are developed. If physicians are paid by the hospital, base future forms of compensation on achieving the goals. Asking them to assist the hospital in evaluating complementary e-prescribing or EHR products. If your hospital is not in the position of supporting physicians financially, offer to assist them with process mapping and workflow improvement, vendor selection tips, contract coaching, technical assessments, etc. Benchmarking physician use of CPOE, e-prescribing, and EHR. Professional medical societies favor adopting automation and can provide data on adoption, as well as strategies that appeal to specific specialties. States medical societies, e-health initiatives, malpractice carriers, insurers, and other programs may have IT mandates, incentives, or resources. Institute a regular communication process with all members of your medical staff illustrating your commitment. □ Engaging nursing staff. In some cases, nurses are less interested and knowledgeable about clinical information systems than physicians. CPOE creates significant workflow changes for nurses, who must come to trust the process just as physicians must learn to trust the support embedded in the system. Trust is largely achieved through education and involvement in every step of the selection and implementation process. Engage nurses by: Providing time dedicated to education for HIT in general and CPOE and EMAR specifically, computer skills building, and exploring the impact of automation on nursing practice in general. This will pay off in many ways: gaining adoption of EMAR most directly (which you may do before or after CPOE), getting invaluable input into the entire medication management workflow and point-of-care documentation support, and encouraging and supporting nurses in their professional work. Having nurses work one-on-one with physicians in their various preparatory steps and during implementation. Their functions are complementary, so their involvement in HIT also should be complementary. This can also enhance physician-nurse team building where physicians may not have direct ties to the community or where you want to encourage retention of both nurses and physicians. Providing time dedicated to workflow and process improvement activities. This will provide immediate benefit where nonstandard practices currently exist, and ultimately in the HIT systems. Having nurses complete process mapping, early in the consideration phases of all aspects of HIT, gets them to see the areas where change is needed and will better assure adoption of new processes. □ Pharmacy’s role in CPOE. While many small and rural communities have limited pharmacist support, active participation from pharmacy is needed to help pharmacists with the HIT adoption process as well as to engage them in helping system build for the HIT. For example, names of medications in an EMAR system are not the same as in a pharmacy system (2.2 Optimization Strategies for Electronic/Bar-Code Medication Administration Record). This is also true for CPOE. The hospital’s present pharmacy information system may need a thorough review and possible upgrade. Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 6 Engage your pharmacy consultant in all aspects of selection and implementation. This may mean building in the cost of additional pharmacist time into the overall project. Engage your local retail pharmacist. In small and rural communities, this individual is probably closely aligned with the hospital and clinics. The pharmacist can assist in reviewing the pharmacy and therapeutics aspect of the system during selection and the clinical decision support rules during implementation. The pharmacist may be a resource to others who can provide answers to questions or suggest better processes. Engage the nurses in the hospital who perform pharmacy duties in the absence of the pharmacist to ensure that they fully understand and have input into all processes. Depending on who procures drug and biological supplies, you may need to engage that individual as well as some your suppliers. □ Determine what source and destination systems are needed for CPOE to work for all orderables. Review a sample of orders to ensure you have identified all potential systems that may need to receive orders. If a high percentage of orders is placed to a service that does not have a system, the result will be dual (paper and electronic) processes which is undesirable. If orders are occasionally placed for a service that does not have a system, they likely will have to be processes by exception. In evaluating CPOE products, determine if the exception can be such that the orders are directed to a nursing system that can retrieve them and process them manually, or if they need to be handwritten by the physicians. Each of the following systems may need to be evaluated in terms of whether they are prepared to receive orders, notify staff in the department of the presence of an order, and have the ability to acknowledge receipt of the order. The presence and capabilities of information systems that need to be reviewed include those in: Pharmacy Laboratory Nursing Nutrition and Food Service Radiology Surgery Specialty areas, such as ED, ICU, nursing home, home health, etc. Billing Others. Workflow and Process Improvement The high level workflow map below illustrates the fundamental processes and workflows, and key questions to ask in preparation for CPOE selection and implementation. An important part of workflow and process mapping for CPOE is to understand the thought process of the provider doing the ordering. This will not be easy, even when you get the provider engaged, because much of the processing is second nature. If patient safety and quality improvement are important factors for the organization, you need to be able to tease out what are the most important elements that exist today and what is missing that you want in a CPOE system. Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 7 As current workflows and processes are mapped, providers and other stakeholders should be able to establish measurable goals. Record these in a manner that illustrates how they can be accomplished with HIT and when you will know you have achieved the goals (1.2 Goal Setting). The following are high level objectives hospitals ought to be able to achieve with CPOE. Modify or add to these, and make them specific and measureable for your organization: Reduce errors of omission and commission in ordering to improve patient safety Decrease variation in standards of care to improve quality Achieve more-effective dosing for improved response time to therapy Increase turnaround time for ordered services to facilitate patient response and reduce length of stay Respond more rapidly to changes as monitoring indicates Improve downstream productivity by reducing time to address follow up issues Reduce cost of care CPOE System Selection All of the above should position your organization to select the system that best meets your needs, or at least to recognize if a system you are evaluating does not address them. Many small and rural facilities may have limited choices in for products that serve their markets. Recognizing what these systems may lack can help you encourage your vendor to support those functions in subsequent product releases and help you address these deficiencies in your new workflows and processes. No perfect product is available—for any environment—so you may need to compromise. The following are important requirements to consider in evaluating CPOE systems: □ System characteristics User-friendly interface Sub-second response time Reliability Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 8 Workstations available everywhere needed Ability to modify decision support rules Ability to create favorite lists for frequent orders Ability to create standing orders □ Functionality Duplicate therapy checking Drug-drug checking Drug-allergy checking Drug-hospital formulary checking Drug-health plan formulary checking (e-Rx) Drug-lab checking (general) Dose-renal function checking Dose-age and weight, or BSA Dose-height and weight, or BMI Drug-disease indications Corollary orders for adjunct drugs and tests Corresponding monitoring orders/secondary orders Expiring order alerts Alerts with options to facilitate response Exception documentation for alert overrides Links to reference material Links to patient education material CPOE Implementation During process mapping, be sure to collect all standing orders, samples of commonly placed order sets, and other forms and reports that are used to support all aspects of the ordering process and audit quality of care. All of these should factor into your ability to perform system build effectively (2.1 System Build). In addition to engaging all stakeholders in system build, the following are often important go-live planning issues to address: □ Rollout strategy options Big bang mandate. This rollout strategy has often been avoided because of the belief that physicians and staff cannot manage too much change at one time. Many organizations are finding that a long, drawn-out process of implementation can actually be a detriment. For a very small organization, the question of big bang may be moot, but mandate is still an issue. Allowing providers to adopt at their own pace has backfired for many. If providers are engaged early and in all aspects of the selection and implementation of systems they are expected to use, a mandate likely will not be needed or will be effective. Medication ordering first, then other orderables. While this is not ideal, many organizations chose this primarily to ease providers into CPOE. This creates dual processes and more work. For hospitals that have limited resources and want to achieve the benefits of CPOE for patient safety, adopting this rollout strategy may be necessary. Most common standing orders first, then others. This strategy attempts to follow the 80/20 rule of phasing in a system. This may be an effective strategy for the first few days that CPOE is used or in a large facility where bugs need to be worked out. In general, for any sized facility, it should not be used over an extended period of time because it will have the same effect as any other phased approach, where dual processes actually create more work for providers and more confusion for other staff, potentially posing an unintended risk. Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 9 □ Training strategies. As with all other aspects of implementation, the more engagement of stakeholders in the process of selection and implementation the more likely you are to have wellpositioned users ready to accept training and even able to navigate reasonably intuitive systems on their own. Address the following special training issues: Physicians prefer minimum training and maximum personal coaching. While time consuming for trainers or other staff, one-on-one support to learn to use the system pays huge dividends. Even if some classroom or online training is provided, one-on-one support in the early days of go live is essential. Training on actual screens and workflows is essential. If temporary workflows have to be introduced because of waiting for a system upgrade or an interface or other issue, the temporary workflow is likely to becomes permanent. This is a matter of how much change can be learned within a short period of time. You are better off delaying implementation than to train and have to retrain shortly thereafter. Use clinicians as coaches and trainers. Not only does this demonstrate that actual clinicians can do this, but it reduces potential embarrassment for those who feel they lack skills or abilities. Some peer pressure is built in to this approach, encouraging greater adoption. New and infrequent users need special attention. - Many small and rural hospitals will have a fairly significant amount of turnover, at least in their physician community. As a result, you need a formalized plan to afford new users as much training as original users received in order to optimize their adoption. Many new users also may be new providers. They may have been exposed to CPOE and other clinical automation where they trained. If physicians rotated through a Veterans Administration (VA) hospital, they will surely have used its EHR. These new, experienced individuals may believe that having used one system they will know how to use another. They may find that your systems are very different than what they have previously used, with more or less functionality. To reduce their potential frustration, have a competency requirement for all new users—no matter who they are—and set appropriate expectations. - Infrequent users may be the biggest challenge. Using the system so infrequently, they cannot be expected to remember all of the functions. If they rotate among a variety of facilities, each with different systems, they may have an especially difficult time remembering how each works. For all users, having basic cheat sheets that walk them through the typical process they are expected to perform can be helpful. You may need to designate a staff member to always be ready to assist them. Not using the system is unacceptable, any exception increases the risk of unintended consequences. □ Ongoing maintenance and support. As the practice of medicine changes (new drugs, drug resistant strains of viruses, new evidence to support changes in practice standards, etc.), clinical information systems must be kept up to date. Some suggestions to aid the ongoing maintenance include: Solicit user feedback early, often, and ongoing. User feedback is critical, and the organization should be open to hearing and addressing everything. Every suggestion should be considered, even if you decide not to act on every one. Organizations should accept feedback without being defensive or assigning blame. Continuing your Issues Log to capture suggestions and monitor who is making them can be useful (2.1 Issues Management). Extensive suggestions from one person can signify a problem. Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 10 For clinical changes, ensure you have a process to vet the proposal and obtain approval for the change from the appropriate channels. A single change in a data element or rule can have a ripple effect. When system changes affects users, explain the proposed change in advance so the change does not disrupt actual practice. Something as simple as moving a data element from one place on the screen to another in order to add another element can cause frustration and potential distrust. Find a mechanism that works for communicating such changes, even if it means hanging sticky note on every computer. Keeping current with all system patches, updates, and upgrades is essential. Not only will skipping such an update result in a potential clinical problem, but it can also result in additional cost to the organization if a later change that is critical requires all previous changes to have been made. Copyright © 2009, Margret\A Consulting, LLC. Used with permission of author. For support using the toolkit Stratis Health Health Information Technology Services 952-854-3306 [email protected] www.stratishealth.org Section 2.2 Utilize – Effective Use – Optimization Strategies for CPOE and e-Prescribing - 11