Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
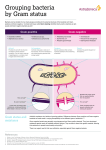
Medical microbiology 1.Give definitions (24) Plasmid: A plasmid is extrachromosomal, circular DNA with an origin of replication (allows replication) and often contains genes for antibiotic resistance, metabolism of unusual molecules (e.g., Pseudomonas), or virulence. Virion: The complete virus particle. In some instances(papovaviruses, picornaviruses), the virion is identical with the nucleocapsid. In more complex virions (herpesviruses, orthomyxoviruses), this includes the nucleocapsid plus a surrouding envelope. This structure, the virion, serves to transfer the viral nucleic acid from one cell to another. Defective virus: A virus particle that is functionally deficient in some aspect of replication. Horizontal spread: Transmission of a pathogen from infected individuals to conspecific individuals within a generation or overlapping generations in a season. Transformation: Acquisition of DNA from the extracellular space, which becomes part of the chromatin. Genetic reassortment: A process in which DNA packaged as a chromosome is broken and fragments are exchanged with another independent chromosome. Occurs during prophase 1 of meiosis. Adherence: the process by which bacteria stick to the surfaces of host cells. Once bacteria have entered the body, adherence is a major initial step in the infection process. The terms adherence, adhesion, and attachment are often used interchangeably. Virulence: The quantitative ability of an agent to cause disease. Virulent agents cause disease when introduced into the host in small numbers. Virulence involves invasion and toxigenicity. 2.Answer the questions 2.1 Describe the microscopic morphology (e.g., Gram-stain characteristic, shape of organism) of the following bacteria: Staphylococcus, Escherichia, Neisseria, Clostridium, Enterococcus, and Pseudomonas. (8) Answers: Staphylococci are gram-positive cocci arranged in clusters. Escherichia are gram-negative rods that typically stain more intensely at the ends (bipolar staining). Neisseria are gram-negative cocci arranged in pairs with the adjoining sides flattened together (shaped like a coffee bean or biscuit). Clostridia are gram-positive spore-forming rods. The spores may or may not be obvious depending upon the species and growth conditions. Typically, spores are not observed in active infections. Enterococci are gram-positive cocci arranged in pairs or short chains. Pseudomonads are small gram-negative rods frequently present in end-to-end pairs. 2.2 How do the differences between gram-positive and gram-negative cell walls influence the cells' clinical behavior, detection, and treatment? (8) Answer: The thickness of the gram-positive membrane facilitates its identification by the Gram stain by trapping the stain, whereas the gram-negative peptidoglycan is only a single layer thick, and the stain washes away during the procedure, requiring use of a counterstain. The LPS present in the outer membrane is the most potent activator of innate and immune functions of any cell wall component and can induce fever and sepsis. Gram-negative bacteria are more likely to induce fever and sepsis. The presence of the outer membrane of gram-negative bacteria provides a unique barrier to complement, to the permeability of large and hydrophobic molecules, and prevents access to peptidoglycan and other internal bacterial structures, including antibacterial drugs. 2.3 Why are spores more resistant to environmental stresses? (8) Answers: Spores are more resistant because they are not growing; they are desiccated, and they are covered with multilayers of a peptidoglycan-like material and a keratin-like protein coat. 2.4 Define the following terms and give one example of each: sterilization, disinfection, and antisepsis. (8) There is not a uniform definition of sterilization and disinfection. In general sterilization represents the total destruction of all microbes including the more resilient forms such as bacterial spores, mycobacteria, nonenveloped viruses, and fungi. Examples of agents used for sterilization are ethylene oxide, formaldehyde gas, hydrogen peroxide, peracetic acid, and glutaraldehyde. Disinfection results in the destruction of most organisms, although the more resilient microbes can survive some disinfection procedures. Examples of disinfectants include moist heat, hydrogen peroxide, and phenolic compounds. Antisepsis is used to reduce the number of microbes on the skin surfaces. Examples of antiseptic agents include alcohols, iodophors, chlorhexidine, parachlorometaxylenol, and triclosan 2.5 what kinds of methods you will use to find out the possible organism of a fever patient? (8) Answers: Direct Detection of Microorganisms in Patient Specimens Microscopic Observation ' Detection by Culture Antigen Detection by Agglutination or Enzyme Immunoassays Molecular Assays: DNA-probe and PCR and RTPCR 3.study the cases then select one right answer each. (12) Case 1. Your patient is a 10-year old girl who is receiving chemotherapy through an indwelling venous catheter. She now has a fever of 390 C but is otherwise asymptomatic. You do a blood culture, and the laboratory reports growth of Staphylococcus epidermidis. Which of the following is least likely to be found by the clinical laboratory? D A. Gram-positive cocci in clusters were seen on Gram stain of the blood culture. B. Subculture of the blood culture onto blood agar revealed nonhemolytic colonies. C. A coagulase test on the colonies was negative. D. A catalase test on the colonies was negative. Case 2. Your patient is a six-year old boy with papular and pustular skin lesions on his face. A serous, honey-colored fluid exudes from the lesions. You suspect impetigo. A Gram stain of the pus reveals many neutrophils and Gram-positive cocci in chains. If you cultured the pus on blood agar, which one of the following would you be most likely to see? A A. Small beta-hemolytic colonies containing bacteria that are bacitracin sensitive. B. Small alpha-hemolytic colonies containing bacteria that are resistant to optochin. C. Large nonhemolytic colonies containing bacteria that are oxidase positive. D. Small nonhemolytic colonies containing bacteria that grow in 6.5% NaCl. Case 3. Your patient is a 20-year-old woman with a sudden onset of fever to 1040 F and a severe headache. Physical examination reveals nuchal rigidity. You suspect meningitis and do a spinal tap. Gram stain of the spinal fluid reveals many neutrophils and many Gram-negative diplococci. Of the following bacteria, which is the most likely to be the cause? B A.Streptococcus agalactiae B.Neisseria meningitides C.Streptococcus pneumoniae D.E. coli Additional history reveals that she has had several serious infections with this organism previously. On the basis of this, which one of the following is the most likely predisposing factor? C A. She is HIV antibody positive B. She is deficient in CD8-positive T cells C. She is deficient in one of the late-acting complement components D. She is deficient in antigen presentation by her macrophages Case 4. Your patient is a 45-year-old woman who was part of a tour visiting the Grand Canyon. The day before coming home, several members of the group developed fever, abdominal cramps, and bloody diarrhea. Of the following, which is the least likely organism to cause this infection? C A.Shigella dysenteriae B.Salmonella enteritidis C.Staphylococcus aureus D.Yersinia enterocolitica A stool culture reveals lactose-negative colonies on EMB agar and mannitol fermenting colonies on CIN plates. Which of the following is the most likely organism to cause this disease? A A.Shigella dysenteriae B.Salmonella enteritidis C.Staphylococcus aureus D.Yersinia enterocolitica 4. Study the case then answer the question (24) A 61-year-old woman with left-sided face pain came to the emergency department of a local hospital. She was unable to open her mouth because of facial muscle spasms and had been unable to eat for 4 days because of severe pain in her jaw. Her attending physician had noted trismus and risus sardonicus.The patient reported that 1 week before presentation, she had incurred a puncture wound to her toe while walking in her garden. She had cleaned the wound and removed small pieces of wood from it, but she had not sought medical attention. Although she had received tetanus immunizations as a child, she had not had a booster vaccination since she was 15 years old. The presumptive diagnosis of tetanus was made. 4.1 How should this diagnosis be confirmed?(6) 4.2 What is the recommended procedure for treating this patient? (5) 4.3 Should management wait until the laboratory results are available?(2) 4.4 What is the long-term prognosis for this patient? (5) 4.5 Compare the mode of action of the toxins produced by C. tetani and C. botulinum. (6) Answers: 4.1 The diagnosis of tetanus is based on the clinical presentation and history (e.g., history of a penetrating injury in a nonimmune individual). Laboratory tests that can be used to confirm the diagnosis include microscopy (useful if positive but generally organisms are not observed in the wound) and culture (relatively insensitive because the organisms are extremely oxygen sensitive). Serology is not useful (antibodies to the toxin do not develop). 4.2 If tetanus is suspected, treatment should begin immediately. This requires debridement of the primary wound, use of metronidazole, passive immunization with human tetanus immunoglobulin, and vaccination with tetanus toxoid. Wound debridement and antibiotic therapy eliminate the vegetative cells producing toxin, passive immunization inactivates free toxin (bound toxin cannot be eliminated), and vaccination protects the patient from future exposure to toxin. The prognosis is determined by the site of the initial injury, the rate of onset of disease, and the rapidity of appropriate management. Mortality in the US is relatively low because the diagnosis is typically made quickly and effective support measures are generally available. In less developed countries, the mortality associated with tetanus is high. 4.3 Tetanospasmin and botulinum toxin are both A-B toxins. The B subunit of tetanospasmin binds to specific sialic acid receptors and adjacent glycoproteins on the surface of motor neurons. The combined toxin is then internalized in endosomal vesicles and transported in the neuron axon to motor neuron somal located in the spinal cord. At this site, the endosome becomes acidified, resulting in a conformation change in the B chain, which facilitates transport of the A chain into the cell cytosol. 4.4 The A chain is an endopeptidase that degrades proteins that regulate the inhibitory neurotransmitters glycine and gamma-aminobutyric acid. This leads to unregulated excitatory synaptic activity in motor neurons. 4.5 Botulinum toxin also binds to specific sialic acid receptors and glycoproteins on the surface of motor neurons (different targets than tetanospasmin) and is internalized. Botulinum toxin remains in the endosome at the neuromuscular junction (vs. travel to spinal cord), where following acidification the endopeptidase A chain inactivates the proteins that regulate release of acetylcholine. Because acetylcholine is not released, neurotransmission is blocked, resulting in flaccid paralysis.