Survey
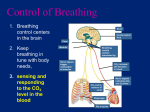
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Respiratory Physiology 1. What are the five functions of the respiratory system? 2. What is the purpose of ventilation? 3. Where does gas exchange take place? 4. What structure uses the oxygen? 5. What is the process of bringing air in and out of the lungs? 6. What are the only organs that do not have smooth muscle? 7. What special type of tissue is found in the lungs? 8. Can the lungs inflate on their own? 9. What do they need to get volume changes? 10. What regulates air flow to the lungs? 11. When the partial pressure of a gas is increased, what does that indicate about the concentration of the gas? 12. How are the lungs protected from pathogens and accumulation of debris? 13. What moves oxygen into the blood? 1) 2) 3) 4) Respiration Acid-base balance Vocalization Defense against pathogens and debris 5) Route for water and heat loss To bring oxygen to the blood Between alveoli and blood plasma Between plasma and hemoglobin in RBC Mitochondria; they use it to make ATP Ventilation The Lungs do not have smooth muscle and instead have elastic tissue. However, the bronchioles have smooth muscle. Elastic tissue NO They need to be tethered to muscles Volume changes regulate air flow The concentration of the gas is increased. Macrophages (millions in the lungs) Pressure gradients (just like concentration gradients) 14. What two gases are involved in external respiration? Oxygen and CO2 15. What is the route that oxygen takes when diffusing down its concentration gradient? Lungs plasma cells 16. What is the route that CO2 takes when diffusing down its concentration gradient? Cells plasma lungs 17. When gases move from lungs to cells and from cells to lungs, what is that process called? External respiration 18. How do the mitochondria use oxygen? They use it as an electron acceptor (they place two H+ on it, which turns it to water). Excess water leaves the cell and enters the tissues. 19. Where does the water go when mitochondria make it? 20. The constant removal of oxygen from the plasma and the addition of water to the tissues creates a driving force known as what? Starling’s principle 21. What is Starling’s Principle? 22. What is internal respiration? What is cellular respiration? 23. Define Carbon Monoxide (CO) Since the new water made by mitochondria released into the tissues does not have particles in it, oxygen (which is a particle) will be sucked into the tissues. Gas exchange that occurs at the tissue capillary beds Actual use of oxygen as a final electron acceptor (process called oxidative phosphorylation) Odorless, colorless gas from incomplete burning of fuel 24. How does CO differ from Oxygen? Binds to hemoglobin 200x stronger than Oxygen, so it drives Oxygen out of hemoglobin and attaches and stays there. 25. What effect does CO have on oxygen transport? CO decreases the amount of Oxygen that can be transported by hemoglobin 26. If a person dies from suffocation and their lips are cherry red, what does that mean? What if their lips were blue? Cherry red – died of carbon monoxide (CO) poisoning Blue – cyanide poisoning 27. What is called when oxygen is on a hemoglobin molecule? oxyhemoglobin 28. Define dissociation of hemoglobin: When the oxygen is released and enters the tissues. 29. When does it increase? 30. What is the waste product of cellular respiration? When the pCO2 levels increase Carbon dioxide 31. How does the body get rid of this waste product? CO2 will attach onto the hemoglobin and be taken to the lungs to be expelled. 32. What happens to the CO2 when it enters a RBC? It reacts with water in the RBC and turns into carbonic acid (H2CO3) 33. What happens after carbonic acid formed and what does it break into to? Carbonic acid breaks apart into a hydrogen ion (an acid) and bicarbonate ion (HCO3- a base). CO2 + H2O H2CO3 H+ + HCO3- 34. What is the reaction for CO2 breakdown? 35. Does the above reaction go to the right or the left in the tissues? 36. Does it go to the right or the left in the lungs? Goes to the right in the tissues Goes to the left in the lungs 37. What ions control the PH of the body? Hydrogen ions lower the body’s pH, while bicarbonate ions raise the pH. 38. In what form is CO2 predominately transported into the blood? Bicarbonate 39. How is the number of H+ in the blood affected by CO2 levels? The more CO2 in the blood, the more H+ in the blood, which makes the blood acidic. bicarbonate ions are absorbed to raise the pH 40. If the blood is too acidic, how do the kidneys compensate? 41. If the blood is too alkaline, how do the kidneys compensate? bicarbonate ions are excreted to lower the pH 42. What happens to a person’s breathing rate if they have excess H+ ions in their blood? They will breathe more rapidly 43. If a person has an airway obstruction, what happens to CO2 levels, and how does this affect blood pH? 44. What is it called when a person has low pH? They cannot exhale excess CO2, so blood levels of CO2 (an acid) build up, and pH decreases. acidosis 45. What happens if enzymes are not in their optimal pH range? They don’t work and chemical reactions stop 46. How does hyperventilation affect CO2 levels in the blood, and how does this affect the pH? 47. What is it called when a person has high blood pH? Hyperventilation means they are exhaling too much CO2, so there is too little CO2 in the blood. That will increase the blood pH (more basic) alkalosis 48. What are changes in lung volume dependent on? Change in thoracic cavity volume 49. What causes alterations in the space inside the thoracic cavity? Contractions of the diaphragm, intercostals muscles 50. How are these muscles innervated? By neurons in the respiratory centers of the brain stem (medulla and pons) 51. What parts of the brain control and regulate the rate of respiration? The Medulla Oblongata and the Pons 52. Which part of the brain contains the pneumotaxic center? The Pons 53. What effect does the Pneumotaxic Center have on breathing rate? It decreases breathing rate. 54. How does the dorsal portion of the Medulla Oblongata affect breathing rate? It increases it. 55. During quiet respiration, is the ventral portion of the Medulla Oblongata active or inactive? Inactive 56. During forced expiration, is the ventral portion of the Medulla Oblongata active or inactive? Active 57. Name the 3 different chemoreceptors? Carbon Dioxide, Hydrogen Ion and Oxygen 58. Of the 3 chemoreceptors which are the central and which are the peripheral receptors? The central chemoreceptors are Carbon Dioxide and Hydrogen Ions and the peripheral chemoreceptors is Oxygen. Located in the medulla their functions are to sense the levels of O2, CO2, and pH in the CSF (cerebral spinal fluid). To sense the Oxygen levels in the blood. 59. What are the functions of the Central Chemoreceptors (these are the ones in the brain)? 60. What are the functions of the Peripheral Chemoreceptors (these are the ones in the aorta and carotid arteries)? 61. What are 2 cranial nerves that carry information on O2 levels from the aorta and carotid chemoreceptors and take the information to the brain? 62. What does the brain do with information received from chemoreceptors? 63. What does the brain do if blood O2 levels are too low? Aortic chemoreceptors - CN X Carotid chemoreceptors – CN IX Maintains proper respiratory rates. If blood O2 levels are too low, will increase breathing rate. 64. What if blood CO2 levels are too low? If blood CO2 levels are too low, will decrease breathing rate. 65. What if blood pH is too low? If blood pH is too low (acidic), will increase breathing rate to get rid of more CO2, which is an acid. Relaxed breathing 66. What type of breathing requires the diaphragm to contract for inspiration, and for the diaphragm to relax for expiration? 67. What muscles are required during Forced breathing? 68. Respiratory centers are most sensitive to what in the blood? CO2 or O2? Forced breathing requires the diaphragm plus muscles that raise and lower the ribs (external intercostals for inspiration, internal intercostals for expiration). They are most sensitive to the level of CO2 in the blood. 10. The most effective stimulus to the respiratory center is An increase in pCO2 69. How is blood flow to tissues controlled? 70. What is the level of O2, CO2, pH, and temperature in cells and tissues that are undergoing increased aerobic activity? By sphincters (smooth muscle) in the capillary beds. This allows the body to adjust the amount of blood flowing to particular tissues. Less oxygen, more CO2, lower pH, and increased temperature. 71. Is ATP used during inhalation? Yes 72. Does normal exhalation require ATP? NO it does not 73. People with respiratory problems use what substance more so than normal? ATP 74. Why do people with respiratory problems need skeletal muscles in the thoracic cage? Skeletal muscles in the thoracic cage are needed to change the thoracic volume, which changes the pressure gradients. No. 75. Are lungs muscular structures? 76. Which direction does air flow in relation to pressure? Air flows from high pressure to low pressure. 77. Boyle’s Law is what formula? P1V1=P2V2 78. What two factors are inversely related in Boyle’s Law? Pressure and volume 79. Every time a molecule strikes the wall of a container what does it cause? Pressure 80. What increases the number of collisions of particles against the side of a wall, thereby increasing pressure? Decreasing volume 81. Decreasing volume does what to pressure? Increases 82. In a large container with few molecules, would there be less or more air pressure in the lungs? 83. What must the lungs have to create a pressure change? Less A volume change 84. What is required to have air move into and out of the lungs? A volume change which creates a pressure change 85. What two muscles contribute to increased volume in the thoracic cavity? Diaphragm and External Intercostals 86. Which muscle contributes the most to increase the volume in the thoracic cavity? Diaphragm 87. When the diaphragm contracts which way does it pull? Downward 88. When the chest wall expands, why do the lungs expand with it? The lungs are stuck to the chest wall because the serous fluid in the pleural cavity makes the lungs stick to the chest wall like two pieces of wet glass stuck together. When lungs expand, their volume expands. Their pressure drops, so air flows from outside (higher pressure) to the inside of the lungs (lower pressure). 89. When the lungs expand, what happens to their volume? What happens to the pressure inside them, compared to the outside air? Where does air then flow? 90. As air flows in, what happens to the volume and pressure in the alveoli? The alveoli expand, so volume expands and pressure decreases 91. When alveolar pressure decreases, where does air flow in from? Air flows in from the bronchi 92. At higher altitudes, does the concentration of oxygen change? No, it is always 21%, whether you are at sea level or high altitude. 93. At higher altitudes, does the pressure of air increase or decrease? Air pressure decreases at higher altitudes 94. Does it require ATP to exhale? No, just relax the muscles. 95. When you exhale, what makes the lung volume decrease? 96. What happens to the pressure? The elastic tissue will recoil. 97. What is the definition of lung compliance? 98. What is compliance the opposite of? 99. What effect does low lung compliance have on the pressure and volume? 100. More energy is needed to breathe in a person with high or low lung compliance? Pressure decreases How much the lung volume changes when the pressure changes It is the opposite of stiffness Would need a greater change in pressure to change the volume. Instead of needing only 10 mmHg pressure difference between the outside air and the lungs, would now need a 20 mm difference. More energy is needed in low compliance 101. How does low lung compliance affect the depth and rate of breathing? Shallow breaths and increased rate. 102. The outside air has a higher level of pressure than the inside of the lungs. That means there is a pressure gradient. 103. How are the pressure gradients switched so the air in the lungs is lower than the outside air? 104. Are the lungs MUSCULAR structures? According to Boyle’s law we will need to create volume changes! The volume in the lungs will have to decrease, so the pressure in the lungs will decrease to something below atmospheric pressure. NO 105. What is the Flow Rule? (Patm – Palv) divided by Resistance 106. What does Patm, Palv, and Resistance mean? Patm is the pressure of the air in the atmosphere. Palv is the pressure of air in the alveoli. Resistance relates to how obstructed or clear the passageway is. Less air flow when resistance is increased 107. How does resistance affect air flow? 108. What are the two types of air pressures? Atmospheric pressure Alveolar (pulmonary) pressure 109. What is required to have a pressure gradient between atmospheric and alveolar pressure? There needs to be a difference in pressure 110. What happens if both types of pressures equal each other? - Air will not flow 111. In what pathological condition will there be no pressure gradient between the outside air and the lungs? 112. Will air flow in this condition? - Pneumothorax 113. In what normal condition is there no pressure gradient? 114. What are two scenarios where air will not flow into the lungs? No air will flow. After maximum inhalation, when the atmospheric pressure and alveolar pressure are equal to each other. 1) After maximum inhalation 2) Pneumothorax 115. What are two scenarios where air will not flow out of the lungs? 1) After maximum exhalation 2) Pneumothorax X-axis is the partial pressure of oxygen (pO2) Y-axis is saturation of Hgb with O2 116. On this graph, what is the X-axis? What is the Y-Axis? 117. Are the partial pressure of respiratory gasses in the arteries similar to the alveolar pressures? Yes 118. How much Hbg is saturated when it leaves the lungs? 98% 119. What is the pO2 in tissues? 70 mm Hg 120. How much Hbg is saturated when it first arrives at the tissues? 98% 121. What is the pO2 in the lungs? 100 mm Hg 122. In the lungs (when the pO2 is 100 mm Hg), what is the saturation of hemoglobin? 100% 123. In the body cells (when the pO2 is 40 mm Hg), what is the saturation level of hemoglobin? 75% 124. What does the 25% difference of O2 saturation mean when the RBC’s are passing by cells that need oxygen? That hemoglobin is only giving up 25% of its oxygen to body cells as it passes by. 125. What are the three factors that would cause an Oxyhemoglobin disassociation curve to shift left? pH increase CO2 decreased Temperature decreased (hypothermia) pH decrease CO2 increase Temperature increase (fever) 126. What three factors would cause the Oxyhemoglobin disassociation curve to shift right? 127. Will a left or right shift increase oxygen’s affinity for hemoglobin? Left shift. 128. In a left shift, will oxygen stay on the hemoglobin or come off and go to the tissues? Oxygen will stay on the hemoglobin 129. What can happen when oxygen’s affinity for hemoglobin increases? Tissue hypoxia (even when there is sufficient oxygen in the blood). 130. What are some left shift conditions? Alkalosis and hypothermia. 131. What are some right shift conditions? Acidosis and fever. 132. What happens when oxygen’s affinity for hemoglobin decreases? Hemoglobin will release oxygen more readily. 133. What thin tissue surrounds each lung? 134. What thin tissue lines the thoracic cavity where the lungs touch it? 135. What do the serousal cells in the parietal and visceral pleura make and what is its function? -More oxygen will be released to the cells but less oxygen will be carried from the lungs. Visceral pleura Parietal pleura 136. What could lack of lubrication lead to? A lubricating fluid that prevents the lungs from rubbing against the thoracic cavity. Heat generation denature of proteins 137. If the vacuum of the lungs is disengaged what will happen to the lungs? They will recoil like a deflated balloon (pneumothorax). 138. How is a pneumothorax treated? How does that fix the problem? With an oxygen mask; it increases the outside pressure so air is driven into the lungs to re-inflate them until they stick to the wall again. Moves inferiorly 139. When the diaphragm contracts during inspiration, does it move up or down? 140. Does that increase or decrease thoracic volume? 141. What other muscle contracts during inspiration? 142. Why are the lungs right up against the chest wall? 143. Can lungs actively move? Increases thoracic volume External intercostals The pleural fluid is watery, and makes the lungs stick to the inside of the chest cavity with a strong vacuum, like two wet pieces of glass stuck together. As long as no air gets into the pleural cavity (between the lungs and the chest wall), the vacuum will hold. No, because they are not muscular organs 144. What is a pneumothorax? air in the pleural cavity 145. What is the condition where blood leaks into the pleural cavity? Hemothorax 146. How does Hemothorax occur? 147. What is atelectasis? Injury (Gun shot, stabbing), Spontaneous (tissue erosion, disease lung),Bleeding wound Alveolar collapse or entire lung collapse 148. Is normal expiration an active or passive process? Passive 149. What is the difference between an active and passive process in the lungs? Active (normal inhalation) means it uses energy because it needs muscle contraction. Passive (normal exhalation) requires no muscles to contract; you just relax the diaphragm. internal intercostals and abdominal muscles 150. What two muscle groups are used for forced expiration? 151. What happens to a person that has to forcefully exhale with each breath, demanding the internal intercostals and abdominal muscles to contract a lot? 152. High or low compliance signifies that the lungs are working normally They get a barrel chest. 153. What does low compliance indicate? Some pathological condition is present that interferes with air movement 154. Do people with emphysema have increased or decreased lung compliance? Low 155. During exhalation, why do COPD patients have to forcefully exhale? The bronchiole walls stick to each other due to inadequate surfactant. 156. How does oxygen in a high concentration help a person with COPD to breathe? Oxygen in high concentration helps get air into their lungs but it reduces their drive for them to breathe on their own. CO2 157. Which is the powerful driving force for ventilation in a normal person: O2 or CO2? 158. What becomes the driving force for a person with COPD? High Oxygen. Why? They have less CO2 because they cannot exhale normally. 159. What happens when a person with COPD is given oxygen? Their drive to breathe becomes diminished. 160. What does CPAP stand for? -They eventually end up on a positive pressure ventilator (CPAP) and if the disease progresses they can die from suffocation. Continuous positive airway pressure (machine). 161. Are the lung and chest wall elastic? Yes. 162. What do both the lung and chest wall have a tendency to do after inhalation? Recoil. 163. What is recoil? The tendency to snap back to resting position. 164. Which way does the chest wall recoil? -(Like when a stretched rubber band recoils when you let go of one end). Outward (springs out) 165. Which way does the lung recoil? Inward (collapses) 166. What happens to the intra-alveolar pressure when: Lung volume is increased? Lung volume is decreased? 167. What is the alveolar pressure when there is no air flowing, such as when you are done inhaling or done exhaling? 168. What is pressure: Of the outside air called? Within the alveoli of the lungs called? In the intra-pleural spaces called? 11. normal intrapleural pressure during quiet respiration, relative to atmospheric pressure is negative or positive? 169. Where does air go when atmospheric pressure is greater than alveolar pressure? Decreases intra-alveolar pressure. Increases intra-alveolar pressure. Zero. Atmospheric Pressure. Intra-alveolar pressure. Intra-pleural pressure. Negative, because of the lack or air in the intra-pleural spaces Air flows into the lungs 170. Where does air go when atmospheric pressure is less than Air flows out of the lungs alveolar pressure? 171. What is the difference between the alveolar and intrapleural pressures called? Transpulmonary pressure 172. When the pressure gradient is caused by changing the Palv, what type of breathing is it? Negative pressure breathing How do you help a patient do negative pressure breathing? 173. Changing the Patm gradient is called what type of breathing? How do you help a patient do that? 174. What was invented for polio patients, whose respiratory nerves were paralyzed? 175. Why is the iron lung more like a negative pressure breathing? Put them in an iron lung Positive pressure breathing CPR air bag, O2 mask, or mouth to mouth Iron lung 176. What are the symptoms of acute mountain sickness (altitude sickness)? It works like a reverse vacuum. There is less air pressure in the tank, so there is less pressure on the chest, so the chest recoils more, to help get air in. The vacuum then reverses, increases pressure on the chest, air flows out. Severe headache, fatigue, dizziness, palpitation and nausea 177. What can this cause? Pulmonary edema 178. Why do you get pulmonary edema? 181. How many ml of air do you usually breathe in? You get it from having pulmonary hypertension (increased pulmonary arterial and capillary pressures) You get it from hypoxia (lack of oxygen) in the pulmonary capillaries. The blood pressure rises, attempting to get more O2 there. Going to a high elevation without a chance to gradually adjust. High elevations have lower pO2 levels. 500 ml 182. How much of that reaches the alveoli? 350 ml 183. Where is the rest of that air? It stays in the conductive zone (trachea and bronchi 184. What is the formula for total ventilation? Tidal volume x breathing rate 500 x 12 = total ventilation 185. What is the formula for alveolar ventilation? 186. What is spirometry used for? (Tidal volume – dead space) x breathing rate. For example: (500 – 150) x 12 = alveolar ventilation To measure lung volume 187. What can be measured directly with a spirometer, be specific? Tidal volume, vital capacity, inspiratory and expiratory reserve volume. 179. How do you get pulmonary hypertension? 180. How can a healthy person get hypoxia 188. How much air is exhaled during the first second of exhalation? 80% 189. What is vital capacity? The volume of air a patient can exhale maximally after a forced inspiration 190. What is expiratory reserve volume? The amount of air you blew out in one second 191. Expiratory reserve volume divided by vital capacity should 80%, less than that indicates an equal to ? What is suggested if it’s less than that amount? obstructive pulmonary disorder 192. What are the characteristics of obstructive lung disease? Inflamed and easily collapsible airways, obstruction to airflow, and frequent hospitalizations. 193. What are 3 examples of obstructive lung disease? Asthma, bronchitis, (COPD) chronic obstructive pulmonary disease 194. What are the characteristics of restrictive lung disease? decreased lung volume It takes more work to breathe (get tired) Inadequate oxygenation Decreased vital capacity. 195. What type of breathing is typical of restrictive lung disease? rapid, shallow breathing 196. List four restrictive lung diseases a. b. c. d. 197. Label the graph, 1-10 1. Maximum inspiration 2. Maximum expiration 3. Inspiratory Reserve Volume (IRV) 4. Tidal Volume (TV) 5. Expiratory Reserve Volume (ERV) 6. Residual Volume (RV) 7. Functional Residual Capactiy (FRC) 8. Inspiratory Capacity (IC) 9. Vital Capacity (VC) 10. Total Lung Capacity (TLC) Cystic Fibrosis Infant Respiratory Distress Syndrome Weak respiratory muscles Pneumothorax 198. What is a single cycle of inhalation and exhalation? Respiratory cycle 199. What is respiratory rate? Number of breaths per minute 200. A normal breath in and out is called what? Tidal Volume 201. The amount of air that can be forcefully inhaled after a normal inhalation in known as? Inspiratory Reserve Volume 202. After taking a normal breath in and out, the amount of air that can be forcefully exhaled after normal exhalation is known as what? Expiratory Reserve Volume 203. The amount of air left in your lungs after you exhale maximally? Residual Volume 204. What is Vital Capacity? The volume of air a patient can exhale maximally after a forced inspiration. 205. What two disorders can be differentiated by vital capacity? obstructive (VC normal) restrictive (VC reduced). 206. What is the equation to determine if your vital capacity is normal? VC/ERV should be 80% 207. How is TLC calculated? the sum of all lung volumes 208. What is the definition of inspiratory capacity? amount of air for a deep breath in after normal exhalation 209. What is the definition of functional residual capacity? amount of air left in your lungs after a normal exhale. You have to calculate this 210. What is the formula to calculate FRC? FRC = ERV + residual volume 211. In COPD, is the FRC increased or decreased? FRC decreases 212. In COPD, are the following increased or decreased: lung recoil, tidal volume, exhalation ability Less recoil Decreased tidal volume Cannot exhale enough Area where air fills the passageways and never contributes to gas exchange. 213. What is the definition of Dead Space? 214. What is the formula for Minute Respiratory Volume (MRV)? MRV = Tidal Volume (TV) x Respiration Rate (RR). 215. What is the formula for Alveolar Ventilation Rate (AVR)? AVR = (TV – DS) x RR. AVR = (Tidal volume – Dead Space) x Respiratory Rate a. Decreased VC. b. Increased TLC, RV, and FRC. c. FEV/VC < 80%. 216. What effect do the following have on people with Obstructive Disease a. VC b. TLC, RV, FRC c. FEV/VC ratio 217. What effect do the following have on people with Restrictive Disease a. VC b. TLC, RV, FRC c. FEV/VC ratio a. Decreased VC. b. Decreased TLC, RV, and FRC. c. FEV/VC = normal. 218. What is the Minute Respiratory Rate volume of air that enters the airways (passes the lips) each min 219. What is the Alveolar ventilation rate volume of air that fills all the lung’s respiratory airways (alveoli) each minute 220. What is the formula to calculate Alveolar ventilation rate? AVR = (tidal volume – dead space volume) x rate of breathing 221. What region of the lungs gets more blood flow? The deeper regions 222. What region of the lung has more air flow? The upper regions. 10. The following reversible reaction occurs with CO2 and H2O CO2+H2O H2CO3 H+HCO3 It goes to the right in the tissues and to the left in the lungs. Does this reaction go mainly to the left or right in the lungs? Does this reaction go mainly to the left or right in the tissues? 223. What is hyperventilation, and how does this affect the amount of air sent to the alveoli? The rate and depth of ventilations increases, so more air gets to alveoli. 224. What is the consequence of voluntary hyperventilation? Apnea (no breathing) eventually occurs b/c the arterial blood will have less carbon dioxide than the body wants to get rid of. Only the conductive zone (the trachea, bronchi, and bronchioles). 225. What region of the lungs is affected by hypoventilation? 226. When panting, what happens to the air? Do the alveoli get more oxygen from panting? The shifting of air in the conducting zone. Not increasing air to the alveoli. 227. Is panting hyper or hypoventilation? Hypoventilation 228. How can you compensate for respiratory alkalosis? Only the kidneys can compensate. They do so by excreting an alkaline urine Can you just hypoventilate to compensate? Cannot hypoventilate since hyperventilation is the problem in the first place! 229. How can you compensate for respiratory acidosis? Only the kidneys can compensate. They do so by excreting an acidic urine Can you just hyperventilate to compensate? Cannot hyperventilate since hypoventilation is the problem in the first place! 230. How can you compensate for metabolic acidosis? Kidneys compensate by excreting an acidic urine Lungs compensate by hyperventilation 231. How can you compensate for metabolic alkalosis? Kidneys compensate by excreting an alkaline urine Lungs compensate by hypoventilation 232. When the kidneys excrete an acid urine, what two pH imbalances are being compensated for? Respiratory and metabolic acidosis 233. When the kidneys excrete an alkaline urine, what two pH imbalances are being compensated for? Respiratory and metabolic alkalosis 234. What are 4 Acid-Base conditions? a) Excessive Diarrhea b) Ingesting excessive stomach antacids c) Aspirin Overdose d) Anxiety or Hysteria 235. What is the chemical formula for bicarbonate ( a base)? HCO3 236. Excessive diarrhea causes the problem of high or low bicarbonate (HCO3)? Excessive Diarrhea causes low HCO3 (bicarbonate is a base) 237. Excessive diarrhea leads to an increase or decrease pH in blood? Decreases pH (Acidosis) 238. After the loss of bicarbonate from diarrhea, and before the body compensates, blood CO2 levels are too high or low? CO2 becomes too high 239. How do the lungs compensate for problems associated with excessive diarrhea? The lungs want to decrease CO2 in the blood. Since loss of bicarbonate (a base) makes the blood pH low (acidic), the body compensates by Hyperventilating, to exhale CO2, which is an acid. 240. Ingesting excessive stomach antacids causes the problem of high or low HCO3? Ingesting excessive stomach antacids causes high HCO3 241. Ingesting excessive stomach antacids leads to an increase or decrease in pH in blood? Increase pH (Alkalosis) 242. After the increase of bicarbonate from ingesting excessive stomach antacids, and before the body compensates, blood CO2 levels are too high or low? CO2 becomes too low. 243. How do the lungs compensate after the effects of ingesting excessive stomach antacids? Since CO2 levels in the blood are too low, the person will Hypoventilate to keep from losing more acid (CO2) 244. Aspirin Overdose causes the problem of high or low HCO3? Aspirin overdose causes a low HCO3. 245. Aspirin Overdose leads to an increase or decrease in pH in Aspirin overdose decreases pH in blood blood? acidosis 246. Is this respiratory or metabolic acidosis? Metabolic acidosis 247. Aspirin Overdose causes an increase or decrease in CO2? Increased CO2 in plasma (acidosis) 248. How do the lungs compensate for the problems caused by aspirin overdose? Hyperventilation, which decreases the CO2 content in the blood, thereby removing acid from the blood. 249. Why is panting considered to be hypoventilating instead of hyperventilating? Air does not go all the way to the alveoli in panting. It just circulates in the conductive zone (trachea and bronchi). Therefore, less air than normal is getting in, so it is hypoventilation 250. hypoventilaation causes the problem of high or low CO2? high CO2 251. hypoventilation leads to an increase or decrease in pH in blood? decreases pH in blood (acidosis) 252. hypoventilation causes an increase or decrease in HCO3? Bicarbonate levels will be low 253. Hyperventilation from fear or pain causes what problem? Increase in blood pH (alkalosis) from too much CO2 being exhaled. 254. How can the body compensate for acidosis caused by hypoventilation? The lungs cannot compensate since they are the problem, but the kidneys can compensate by increasing bicarbonate secretion.