Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
SIDE EFFECTS OF AMIODARONE/Harris et al.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
40. Narula OS, Samet P, Javier RP: Significance of the sinus-node
recovery time. Circulation 45: 140, 1972
41. Strauss HC, Bigger JT, Saroff AL, Giardina EGV: Electrophysiologic evaluation of sinus node function in patients with sinus node
dysfunction. Circulation 53: 763, 1976
42. Hellestrand KJ, Bexton RS, Nathan AW, Spurrell RAJ, Camm AJ:
The acute electrophysiological effects of flecainide acetate on cardiac conduction and refractoriness in man. Br Heart J 48: 140,
1982
43. Seipel L, Breithardt G: Sinus recovery time after disopyramide
phosphate. Am J Cardiol 37: 1118, 1976
44. Dean RR, Ferguson DM: Effects of disopyramide on the A-V
conduction system. Arch Int Pharmacodyn 190: 183, 1971
45. Ranney RE, Dean RR, Karim A, Radzialowski FM: Disopyramide
phosphate: pharmacokinetic and pharmacologic relationships of a
new antiarrhythmic agent. Arch Int Pharmacodyn 191: 162, 1971
46. Mathur PP: Cardiovascular effects of a newer antiarrhythmic agent,
disopyramide phosphate. Am Heart J 84: 764, 1972
47. Kent KM, Epstein SE, Cooper T, Jacobowitz DM: Cholinergic
innervation of the canine and human ventricular conducting system. Anatomic and electrophysiologic correlations. Circulation 50:
948, 1974
48. Tonkin AM, Tomos P, Heddle WF, Rapp H: Autonomic effects on
the human cardiac conduction system. Evaluation by intracardiac
49.
50.
51.
52.
53.
54.
55.
56.
45
electrocardiography and programmed stimulation techniques. Br
Heart J 44: 168, 1980
Bissett JK, De Soyza NDB, Kane JJ, Murphy ML: Electrophysiology of atropine. Cardiovasc Res 9: 73, 1975
Akhtar M, Damato AN, Caracta AR, Batsford WP, Josephson ME,
Lau SH: Electrophysiologic effects of atropine on atrioventricular
conduction studied by His bundle electrogram. Am J Cardiol 33:
333, 1974
Stemple DR, Hall RJC, Mason JW, Harrison DC: Electrophysiological effects of edrophonium in the innervated and the transplanted denervated human heart. Br Heart J 40: 644, 1978
Hulting J, Jansson B: Antiarrhythmic and electrocardiographic
effects of single oral doses of disopyramide. Eur J Clin Pharmacol
11: 91, 1977
Niarchos AP: Disopyramide: serum level and arrhythmia conversion. Am Heart J 92: 57, 1976
Dhingra RC, Amat-y-Leon F, Wyndham C, Denes P, Wu D,
Pouget JM, Rosen KM: Electrophysiologic effects of atropine on
human sinus node and atrium. Am J Cardiol 38: 429, 1976
Simpson MB, Spear J, Moore EN: The relationship between atrioventricular nodal refractoriness and the functional refractory period
in the dog. Circ Res 44: 121, 1979
Dreifus LS: The electrophysiology of Norpace (part I). Angiology
26: 111, 1975
Side Effects of Long-term Amiodarone Therapy
LouISE HARRIS, M.B., WILLIAM J. MCKENNA, M. D., EDWARD ROWLAND, M.B.,
DAVID W. HOLT, PH.D., GERARD C.A. STOREY, B.SC., AND DENNIS M. KRIKLER, M.D.
SUMMARY Although amiodarone is an effective antiarrhythmic agent, long-term therapy may be associated with unwanted effects. We report our experience in 140 patients treated over 5 years. Important effects
were seen particularly in the thyroid gland, liver, lung and skin. Some of these effects are dose-dependent
and others may be related to the chemical structure and metabolism of amiodarone. Corneal microdeposits
were always found when sought, but did not cause impairment of visual acuity.
AMIODARONE has been available in Europe for approximately 20 years for the management of angina
pectoris,' but only in the past decade have its unique
antiarrhythmic properties been recognized.2 It is effective in the management of refractory ventricular arrhythmias, including those associated with ischemic
heart disease and the cardiomyopathies.3 4 It is particularly useful in the management of chronic atrial arrhythmias refractory to conventional drugs, with an
impressive conversion rate of chronic atrial fibrillation
to sinus rhythm.4 Amiodarone is especially effective in
suppressing or modifying paroxysmal atrial arrhythmias, including those associated with the Wolff-Parkinson-White syndrome,5 in which sudden death from
rapidly conducted atrial fibrillation is a risk.6
With the more widespread use of amiodarone, several side effects have been identified. In the majority of
From the Division of Cardiovascular Disease, Department of Medicine, Royal Postgraduate Medical School, and the Poisons Units, Guy's
Hospital, London, England.
Dr. McKenna is a Research Fellow of the Medical Research Council
of Canada.
Address for correspondence: Dennis M. Krikler, M.D., Cardiovascular Division, Hammersmith Hospital, Du Cane Road, London W12
OHS, England.
Received April 30, 1982; revision accepted July 7, 1982.
Circulation 67, No. 1, 1983.
patients, these are well tolerated and are often modified by a reduction in dosage so that discontinuation of
therapy is rarely necessary. A few patients, however,
have more serious complications, including pulmonary fibrosis7 I and clinical thyroid disease.9 The incidence, mechanisms and management of these complications is uncertain. Our experience in individual cases
dates back over 9 years. We are now able to report 140
patients in whom we have systematically monitored
the unwanted effects over the past 5 years.
Patients and Dosage
We reviewed 140 patients (95 males and 45 females,
mean age 52 years) who had been taking amiodarone
for an average of 2 years; the longest follow-up was 5
years. Although 69 of our patients were taking amiodarone for primary arrhythmias, including the WolffParkinson-White syndrome, we also treated 15 patients with ischemic heart disease and 48 who had
arrhythmias associated with cardiomyopathy, 28 hypertrophic and 20 congestive. Five patients had valvular disease, two hypertensive heart disease and one
patient an atrial septal defect. Details of the arrhythmias treated are listed in table 1.
The dose varied from 100 to 1200 mg/day, but only
11 patients took 600 mg/day or more long-term; the
CIRCULATION
46
VOL 67 , No 1, JANUARY 1983
The unwanted effects are categorized as thyroid,
hepatic, pulmonary and cutaneous. Ocular and neurologic changes are also considered, as are alterations in
cardiac conduction and repolarization.
TABLE 1. Arrhythmias Treated with Amiodarone
No. of
Mean dose
pts
Arrhythmia
(mg/day)
46
Ventricular tachycardia
440
(200-1200)
10
400
Ventricular extrasystoles
(200-600)
15
310
Chronic atrial fibrillation!
flutter
(200-400)
38
280
Paroxysmal atrial arrhythmia
(100-400)
31
350
Supraventricular arrhythmias,
including Wolff-Parkinson-White
(100-600)
syndrome
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Thyroid
Changes in thyroid function were recognized ear1Y;9 12 the most common was a rise in thyroxine (T4)
and reverse triiodothyronine (rT3) levels, and a fall in
triiodothyronine (T3).'3 There is also an associated
incidence of clinical thyroid disease.
We measured T4 in 10 patients and rT3 in nine of the
same 10 patients systematically over an 18-month period. All had normal thyroid function at the start of
treatment (fig. 1). T4 decreased in the first 2 weeks of
treatment in four of the patients, but thereafter levels
increased in all; rT3 increased in all subjects (increase
of 79% over 18 months). In addition to these detailed
serial observations, we measured T4 in 85 additional
patients. The mean T4 level for the group was elevated
by 20% above the mean for the laboratory (fig. 2). In
five, the T4 level decreased and thyroid-stimulating
hormone (TSH) increased (table 2); two of these patients were clinically myxedematous. In contrast, four
patients had increased T4 levels of 25% or more above
the upper limit of normal (table 2); two were clinically
thyrotoxic. To identify predisposing factors in these
patients with marked alterations in thyroid function,
mean dosage was 360 mg/day. We gave an initial
loading dose of 600-1200 mg/day for 1 week, followed by 400-600 mg/day for a month; thereafter, the
maintenance dose was determined by balancing control of arrhythmia against side effects. Amiodarone
and its desethyl metabolite were measured in plasma
and, where possible, in various tissues, using highperformance liquid chromatography.'10' Plasma concentrations were assessed relative to side effects and
alterations of metabolic function. Drug levels of amiodarone (range 0. 1-5.2 mg/l) and desethyl amiodarone
(range 0.1-5.0 mg/l) correlated with dosage (r = 0.59
p < 0.001 and r = 0.66 p < 0.001, respectively).
190-
SB
170DW
150-
vCH
-6
E
.c
.x
0
;
130-
,
NS
TH
RC.ww
110-
BN
90-
tDS
-{,_
24
70weeks
months
Duration of therapy
1.21. 0_ DW
* NS
BN
-TH
GR
RC
0.8-
Ez
0.4-
0.2O.
O-i
I
I
I
I
0 12
weeks
nI .
I
1
months
3
6
Duration of therapy
12
24
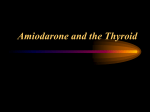
FIGURE 1. (top) Thyroxine levels (nmol/l) in
10 patients before and during amiodarone
therapy for as long as 18 months (nglml =
nmol/l x 1.287). (bottom) Reverse triiodothyronine (T3) in nine patients before and during
treatment with amiodarone for as long as 18
months (ng/ml = nmol/l x 0.651).
SIDE EFFECTS OF AMIODARONE/Harris
Thyroxine (nmol 11)
300n
200-
=
95
es
I
0
100-
m
.
0
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
O0
FIGURE 2. Thyroxine levels in 95 patients during treatment
with amiodarone. The mean level was 124 nmol/l (mean for
normal persons 102 nmol/l).
we examined various clinical features. All had normal
thyroid function before treatment, and none developed
goiter. There was no family history of thyroid disease,
and thyroid antibody titers were negative in all. The
mean duration of treatment before changes were observed was 30 months, and all but two patients were
receiving moderate doses, with appropriate plasma
drug concentrations. '4 Of the five hypothyroid patients, four were more than 70 years old. Generally,
TSH does not increase in relation to age in men. s
However, four of the five patients were male, suggesting that there may be an increased risk of thyroid
et
al.
dysfunction in older patients taking amiodarone, irrespective of their sex. Treatment was discontinued in
one patient (table 2), but T4 was added after 6 weeks
because clinical hypothyroidism persisted. In another
patient (table 2), treatment could not be discontinued
because of the intractability of the arrhythmia; therefore, amiodarone was continued and T4 replacement
initiated. Both patients are now clinically and biochemically euthyroid on replacement T4.
More difficult to assess, and more insidious in presentation, is increased thyroid activity on amiodarone.
As the majority of patients have some elevation of T4
on chronic therapy and some may have tremor and
sleep disturbance, the diagnosis of thyrotoxicosis may
be difficult. In our two clinically thyrotoxic patients,
the diagnosis rested on raised T3 levels (4 nmol/l and
5.3 nmol/l respectively), increasing weight loss, anxiety and weakness. Response to thyrotropin-releasing
hormone (TRH) was not measured, but a flattened
response would have assisted in the diagnosis. There
was no recurrence of the underlying arrhythmia in either patient. Thyrotoxicosis resolved spontaneously,
as judged biochemically and clinically, in both patients
1-2 months after treatment was stopped.
Several mechanisms have been proposed to explain
this spectrum of altered thyroid activity. Amiodarone
does not interfere in the T4 assay and does not modify
the T4-binding globulin concentration. 12 13 Each 200mg tablet of amiodarone contains approximately 75
mg of organic iodine and, in the steady state, metabolism of 300 mg of amiodarone yields 9 mg/day of
iodine,16 which represents a 100-fold increase over the
normal iodine intake. The effects of a chronic iodine
load on thyroid function have been well documented
and both iodine-induced hypothyroidism'7 and hyperthyroidism'8 can occur in apparently normal glands.
An additional acute antithyroid action of an iodine
TABLE 2. Patients with Gross Alterations in Thyroid Function Tests on Amiodarone
T4
Free T4
Dose Duration (nmol/l) (pmol/l)
ArrhythAge
on amiodarone
TSH
mia
Pt
(mg/day) (months)
(years) Sex
function
Decreased
8
>25
M
200
39
70
AFI
JE*
200
10
33
>60
77
F
SND
FD*
44
>20
M
AFI
200
29
76
LH
24
36
19
M
VT
200
77
RM
32
25
>25
M
VT
600
MD
59
Increased function
<1
34
226
39.5
M
VT
400
48
MFt
<1
207
42.0
32
M
62
VT
400
GFt
37
26
193
M
600
40
AF
CAF/FI
231
67.2
36
SVT/WPW 400
F
SB
18
Normal range: thyroxine 45-160 nmol/l; free thyroxine 0.8-24 pmol/l.
*Clinically myxedematous.
tClinically thyrotoxic.
47
AmiDesethyl
odarone amiodarone
(mg/i)
(mg/i)
0.7
1.5
0.5
1.1
0.8
1.5
0.9
1.5
2.0
1.3
4.6
0.5
2.0
1.4
3.8
0.8
Abbreviations: AFR = atrial flutter; SND = sinus node disease; VT = ventricular tachycardia; CAF/Fl = chronic
atrial fibrillation/flutter; SVT = paroxysmal supraventricular tachycardia; WPW = Wolff-Parkinson-White syndrome;
T4 = thyroxine; TSH = thyroid stimulating hormones.
48
CIRCULATION
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
load, the Wolff-Chaikoff effect,'9 may explain the initial fall in T4 in some of our patients (fig. 2). In normal
persons, as in our patients, this effect is transient even
with continued iodine administration, because of autoregulatory inhibition of intrathyroid iodide transport.
Amiodarone itself may have a direct action on the
thyroid gland, but in vitro studies have shown no alteration of active iodide transport, iodine organification
or iodotyrosine deiodination.20 However, a direct intrathyroid action in vivo cannot be ruled out if amiodarone is substantially concentrated in the gland. In a
single postmortem observation of a patient not included in this series, concentrations of amiodarone and
desethyl amiodarone of 15 mg/kg and 92 mg/kg, respectively, were found in the thyroid gland. Amiodarone is also reported to inhibit the peripheral conversion
of T4 to T3 with increased conversion along the alternative pathway to rT3, resulting in a rise in T4 and rT3,
with a low or normal T3;'2 our findings are consistent
with this suggestion.
VOL 67, No 1, JANUARY 1983
6.0f
r = 0.59
a)
(a
I
'A
4!
5.0k
p <0. 001
n =88
c
17
cu
:
1000
*:
Q)
co
V.
0
*.a
6S
Vm
.
0
00
0.
*
3.01-
4m
q
0
Z. u
0
*
0
=
0.0
1.0
2.0
3.0
Amiodarone (mg/I)
4.0
5.0
6. 0
r = 0.62
p <0.001
a)
n = 88
5.0 F
.
.
.E
_
ow'
0
0
4.0 -
0
0
S
@00
.0
nsm
Hepatic
Hepatic dysfunction from drugs is well recognized.
The liver enzymes rise in patients on large doses of
amiodarone, but clinically evident hepatic dysfunction
has not been detected. In 15 of 100 patients taking
amiodarone, we found a 1.5-4-fold increase in serum
aspartate aminotransferase levels. These changes are
seen in patients on high doses and correlate with plasma concentrations of amiodarone (r - 0.59, p <
0.001) and its desethyl metabolite (r = 0.62, p <
0.001) (fig. 3). There was a similar increase in alanine
aminotransferase and a minimal increase in gamma
glutamyl transpeptidase, with no change in serum bilirubin or alkaline phosphatase. Other investigators
have reported similar alterations in hepatic function.
Heger et al. 8 reported a twofold increase in aspartate
aminotransferase and lactic dehydrogenase in about
50% of their patients and Plomteaux et al.21 reported
increased levels of aspartate aminotransferase and malic dehydrogenase in 10-20% of 36 patients. These
changes are not persistent and may fluctuate within the
individual patient over time; they usually return to
normal despite continued treatment. None of our patients or those in these two series8' 21 has developed
clinical hepatic dysfunction. We performed liver biopsies in two patients who had increased enzyme levels,
but no changes attributable to amiodarone could be
demonstrated in either biopsy. In the one biopsy suitable for measurement, there were high concentrations
of amiodarone (1020 mg/kg), and particularly, desethyl amiodarone (5050 mg/kg). Similar concentrations in hepatic tissue were found postmortem in a
patient not reported in this series with ischemic heart
disease who died suddenly. Although amiodarone is
also metabolized in the liver, these high concentrations
probably reflect large hepatic stores of the parent compound, and especially its metabolite.
Hepatic injury due to drugs is common, having both
a wide variety of mechanisms and a wide spectrum of
presentation. Furan derivatives can cause centrilobular
0
*
0
0
a
.Em 4.01-
3.0 F
*1
00 * * 0
go
*.0000.0
.0. *00
**
0
:
*
0
ft
0::..:.
S:w.
0
*
0
*
I
2.0
0.0
1.0
2.0
3.0
Desethyl amiodarone (mg I I)
Il
5.0
4.0
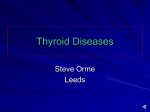
FIGURE 3. (top) Log aspartate aminotransferase vs plasma
amiodarone (mgll) in 88 patients during treatment. (bottom)
Log aspartate aminotransferase vs plasma desethyl amiodarone
(mg/l) in 88 patients during treatment.
hepatic necrosis in rats,22 and amiodarone or its metabolites may produce similar injury. The high incidence
of dose-dependent hepatic changes with amiodarone
suggests a toxic effect rather than host idiosyncrasy as
the underlying mechanism. In our experience, the
changes are transient and do not progress. We therefore monitor hepatic function regularly in patients with
raised hepatic enzyme levels, but do not discontinue
amiodarone.
Pulmonary
Amiodarone has recently been suggested as a possible, albeit rare, cause of pulmonary fibrosis. Only one
of our patients developed pulmonary interstitial
changes with an associated restrictive pattern on pulmonary function testing. Review of his radiographs,
however, revealed that such changes may have been
present before treatment. In addition, a Kveim test had
been positive 4 years previously, but other evidence of
sarcoidosis was lacking. To identify common predisposing factors, we reviewed the five additional cases
that were previously reported.7 8 23 Three of the total of
six patients had been in severe cardiac failure and four
were on high doses (800 mg/day). The interval before
the onset of changes varied widely (2-28 months).
There were no other distinguishing clinical features. In
our patient, immunoglobulin concentrations were elevated and antinuclear antibodies, previously negative,
were positive at a titer of 1:200. These abnormalities
were not detected in the one other patient2' in whom
SIDE EFFECTS OF AMIODARONE Harris et al.
49
they were sought. Lung biopsies were performed in
four of the patients, but only nonspecific featuresalveolar wall fibrosis and atypical pneumocytes
were demonstrated. In our patient and in three previously described, the pulmonary changes resolved
after the amiodarone had been discontinued and corticosteroids commenced. None has been rechallenged
with amiodarone. The two remaining patients died of
severe coexistent heart failure.
The mechanism of pulmonary injury is unknown.
Our patient had positive antinuclear antibodies and
elevated immunoglobulin levels; one possibility is a
drug-induced autoimmune disorder. No conclusions
can be drawn, however, as these tests were normal in
the one other patient in whom they were measured.
Alternatively, a direct toxic effect may occur. The
roles of high dosage and of cardiac failure must be
explored.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Amiodarone Dermatopathy
Two types of skin reaction have been described.
Photosensitivity is common, but there is also a rare
slate-gray pigmentation of the exposed areas. Photosensitivity is the commonest side effect reported by our
patients (57%). There is a wide spectrum of skin reaction, ranging from an increased propensity to suntan
during the summer months to intense burning, erythema and swelling of the exposed areas. We reviewed
dosage and measured plasma concentrations of amiodarone and its metabolite in patients with and without
photosensitivity, but fbund no significant difference
between the two groups. lHowever, the intensity of the
reaction can be alleviated by a reduction in dosage and
most patients can be protected by prophylactic barrier
creams. None of our patients had to stop treatment. We
observed a different skin reaction in the first 2 weeks
after starting amiodarone in six patients: a pruritic,
erythematous, fine maculopapular rash with a predominantly truncal distribution. It resolved spontaneously within days and did not require treatment or
cessation of therapy.
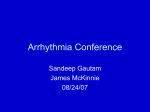
Two patients have developed a slate gray/purple
pigmentation of the face (fig. 4). They had been taking
600 mg/day for 5 and 2 years, respectively, for control
of ventricular arrhythmias. Although not excessive for
the dosage they were receiving, both patients had high
plasma concentrations of amiodarone (3.1 mg/I in
both) and desethyl amiodarone (3.7 mg/l and 3.2 mg/I,
respectively). In one of these patients, biopsies were
taken from affcted skin (fbrehead) and unaffected skin
(forearm). Lipofuscin deposits were noted in both, but
were more conspicuous in the affected skin. Intense
elastic degeneration, inappropriate for the age and solar exposure of the patient, was seen in affected skin
only. Surprisingly, melanin was reduced in the affected skin. Other investigators have also demonstrated
increased lipofuscin deposits, both histologically and
histochemically, in the cells of the dermis of similar
patients and most attribute the pigmentation to this.6
Similar facial pigmentation (visage mauve) has been
described with prolonged use of high doses of pheno-
FIG,URE 4. Slategara facial pigmentation in a patient taking
amiodarone, 600 mg1dav fir 2 vears.
thiazine derivatives, such as chlorpromazine, which
also causes photosensitivity.' Similar histologic deposits have been thought to represent complexes of
chlorpromazine or one of its metabolites. Methacycline- another agent causing photosensitivity'8
also causes intense elastic degeneration in the dermis.
Forty percent of the 34 pigmented patients reported
with amiodarone2t26 29-32 had been taking 600 mg/day
for an average of 2 years before pigmentation developed; this is consistent with the pigmentation being
dose-duration dependent. Furthermore, both of our patients, as well as almost all of those reported, had
experienced photosensitivity before the development
of pigmentation. Perhaps photosensitivity predisposes
to elastic degeneration, with subsequent increased deposition of lipofuscin and skin discoloration in patients
on high doses. If the pigmentation is cosmetically unsightly, amiodarone should be discontinued. In our
one patient who discontinued it and in others, pigmentation improved over a period of 6-12 months. Our
data suggest that this pigmentation can be avoided if
doses are kept as low as possible.
Ocular
Deposits occur in the cornea with amiodarone.33
These deposits, detected on slit-lamp examination,
have been widely described, but no other ocular
changes have been reported.34 We observed comeal
deposits as early as 10 days after starting amiodarone,
and they are present in all of our patients undergoing
ophthalmologic exam:ination after I month. These deposits occur peripherally in the comea, and do not
50
CIRCULATION
produce symptoms. However, two of our patients
using 600 mg/day complained of blue/green haloes on
looking at bright lights and were found to have comeal
deposits encroaching on the pupil. Both responded to a
reduction in dosage. We have observed no other ophthalmologic complications, and no patient has required
discontinuation of therapy for ocular side effects.
Therefore, we no longer advise serial ophthalmologic
examinations in asymptomatic patients on long-term
amiodarone.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Neurologic
Peripheral neuropathy has been seen in rare instances with long-term amiodarone therapy, and intracellular inclusion bodies, similar to those seen in skin,
have been demonstrated in peripheral nerve fibers.36
Proximal weakness, with predominant involvement of
the thigh muscles, was observed in eight of our patients in the first weeks of therapy. It occurred in patients taking high doses (800 mg/day or more) and
resolved spontaneously or with a reduction in dose. A
delay in nerve conduction but normal electromyograms were demonstrated in two other patients taking
1800 and 2000 mg/day, respectively; both responded
to a reduction in dosage.8
Clinically distinct from this is the problem of peripheral neuropathy. There are several reports of a sensorimotor neuropathy, with a glove and stocking distribution, in patients using moderate (400 mg/day) to large
doses (1800 mg/day) for 1 year or longer.36-9 Nerve
conduction velocity is reduced. Histologically, segmental demyelination of the nerve fibers has been
demonstrated as well as lipid-containing lysosomal
inclusion bodies in the Schwann cells. Although the
neuropathy resolves when treatment is discontinued,
this is often slow and incomplete. Some of the patients
described were using other drugs, including perhexiline, but in other cases there were no apparent predisposing factors. None of our patients developed this
complication, and there does not appear to be a means
of identifying which patients are at risk.
Cardiac Conduction and Repolarization
The electrophysiologic effects of amiodarone include depression of sinus"' and atrioventricular nodal
function and prolongation of myocardial refractoriness,41 reflected in the surface ECG as a decrease in
heart rate and repolarization changes.
Although amiodarone has been used safely in patients with the sick sinus syndrome,42 it does prolong
sinus cycle length8 and sinus node recovery time.40 The
concurrent administration of other antiarrhythmic
drugs, such as /8 blockers, may result in sinus arrest.43
Amiodarone increases plasma digoxin concentrations," but the effect of this interaction on arrhythmias
is uncertain. Prolongation of the QTc interval occurs in
the majority of patients and is the electrocardiographic
expression of the drug effect on the action potential
duration. It does not appear to have the same implications as a similar degree of QTc prolongation seen with
quinidine-like antiarrhythmic agents. McComb et al.45
VOL 67, No 1, JANUARY 1983
suggested an association between amiodarone and
atypical ventricular tachycardia. We do not agree that
their patient had torsade de pointes,46 which has not
occurred in any of our patients; nor had it been found
when amiodarone was given as the sole agent in an
extensive review of use of amiodarone in France.47
The mechanisms of the unwanted effects seen in
patients receiving amiodarone fall into two broad
groups. Some of the effects are dose-related. This is
particularly clear in the elevation of the serum aminotransferases, where almost all patients who take 600
mg/day or more have raised levels. Other effects are
both dose- and duration-dependent; the extent of the
corneal microdeposits and the abnormal facial pigmentation are the best examples. These effects of long-term
high doses make careful balance of dose against arrhythmia control imperative. In contrast, the effects on
the thyroid gland and the peripheral nerves appear to
be independent of these factors and suggest specific
reactions in individual patients; thus, older patients on
amiodarone appear to run an increased risk of myxedema. Until we have a better understanding of the
mechanism of the pulmonary reaction, this effect cannot be defined.
Regardless of the mechanisms of these unwanted
effects, almost all, with the possible exception of myxedema, resolve when treatment is discontinued. Amiodarone has proved sufficiently valuable for serious arrhythmias that its judicious administration is often
required; its benefit will clearly be greatest when
knowledge of its side effects is complete.
References
1. Vastesaeger M, Gillot P, Rasson G: Etude clinique d'une nouvelle
medication anti-angoreuse. Acta Cardiol (Brux) 22: 483, 1967
2. Coumel Ph, Bouvrain Y: Etude clinique des effects pharmacodynamiques et antiarythmiques de l'amiodarone. J Agreges 6: 69,
1973
3. Rosenbaum MB, Chiale PA, Halpern MS, Nau GT, Przybylski J,
Levi RJ, Lazzari JO, Elizari MV: Clinical efficacy of amiodarone
as an anti-arrhythmic agent. Am J Cardiol 38: 934, 1976
4. McKenna WJ, Harris L, Perez G, Krikler DM, Oakley C, Goodwin JF: Arrhythmia in hypertrophic cardiomyopathy. Il. Comparison of amiodarone and verapamil in treatment. Br Heart J 46: 173,
1981
5. Rowland E, Krikler DM: Electrophysiological assessment of amiodarone in treatment of resistant supraventricular arrhythmias. Br
Heart J 44: 82, 1980
6. Dreifus LS, Haiat R, Watanabe Y, Arriaga J, Reitman NC: Ventricular fibrillation: a possible mechanism of sudden death in patients with Wolff-Parkinson-White syndrome. Circulation 43: 520,
1971
7. Rotmensch HH, Liron M, Tupilski M, Laniado S: Possible association of pneumonitis with amiodarone therapy. Am Heart J 100:
412, 1980
8. Heger JJ, Prystowsky EN, Jackman WM, Naccarelli GV, Warfel
KA, Rinkenberger RL, Zipes DP: Amiodarone: clinical efficacy
and electrophysiology during long term therapy for recurrent ventricular tachycardia or ventricular fibrillation. N Engl J Med 305:
539, 1981
9. Jonckheer MH, Blockx P, Kaivers R, Wyffels G: Hyperthyroidism
as a possible complication of the treatment of ischaemic heart
disease with amiodarone. Acta Cardiol (Brux) 28: 192, 1973
10. Flanagan RJ, Storey GCA, Holt DW: Rapid high performance
liquid chromatographic method for the measurement of amiodarone in blood plasma or serum at the concentrations attained during
therapy. J Chromatogr 187: 391, 1980
SIDE EFFECTS OF AMIODARONE/Harris et al.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
11. Flanagan RJ, Harris L, Holt DW, McKenna WJ, Rowland E,
Storey GCA: High-performance liquid chromatographic measurement of amiodarone and its desethyl metabolite in plasma. In
Proceedings of the British Pharmacological Society meeting. Oxford, 1981, p 139
12. Burger A, Dinichert D, Nicod P, Jenny M, Lemarchand-Beraud T,
Vallotton MD: Effect of amiodarone on serum tri-iodothyronine,
reverse triodothyronine, thyroxine and thyrotropin: a drug influencing peripheral metabolism of thyroid hormones. J Clin Invest
58: 255, 1976
13. Jonckheer MH, Blockx P, Broeckaert I, Comette C, Beckers C:
Low T3 syndrome in patients chronically treated with an iodinecontaining drug, amiodarone. Clin Endocrinol 9: 27, 1978
14. Holt DW, Storey GCA: Measurement of amiodarone. In Amiodarone and Arrhythmias, edited by Krikler DM, McKenna WJ,
Chamberlain DA. Oxford, Pergamon Press, 1983. In press
15. Tunbridge WMG, Evered DC, Hall R, Appleton D, Brewis M,
Clark F, Grimley Evans J, Young E, Bird T, Smith P: The prevalence of thyroid disorders in an English community. In Thyroid
Research, edited by Robbins J, Braverman LE. Amsterdam, Excerpta Medica, 1976, pp 520-522
16. Broekhuysen J, Laruel R, Sion R: Recherches dans la serie des
benzofuranes. Etude comparee du transit et du metabolisme de
I'amiodarone chez diverses especes animales et chez l'homme.
Arch Int Pharmacodyn 177: 340, 1969
17. Wolff J: Iodide goitre and the pharmacologic effects of excess
iodide. Am J Med 47: 101, 1969
18. Savoie JC, Massin P, Thomopoulos P, Leger F: Iodine-induced
thyrotoxicosis in apparently normal thyroid glands. J Clin Endocrinol Metab 41: 685, 1975
19. Wolff J, Chaikoff IC: The inhibitory action of iodide upon organic
binding of iodine by the normal thyroid gland. J Biol Chem 172:
855, 1948
20. Gluzman BE, Coleoni AH, Targovnik HM, Niepomniscze H: Effects of thyroid iodine metabolism in vitro. Acta Endocrinol 85:
781, 1977
21. Plomteaux G, Heusghem C, Ernould H, Vandeghen N: Longterm
hepatic tolerance of amiodarone in the clinic. Eur J Pharmacol 8:
369, 1969
22. Boyd MR, Burka LT: In vivo studies on the relationship between
target organ alkylation and the pulmonary toxicity of a chemically
reactive metabolite of 4-ipomeanol. J Pharmacol Exp Ther 207:
687, 1978
23. Riley SA, Williams SE, Cooke NH: Alveolitis after treatment with
amiodarone. Br Med J 284: 161, 1982
24. Morand Ph, Benatre J, Viau G, Carli-Basser C, Laine JL, Neel JL,
Brochier M, Raynaud R: Etude clinique et histologique (ultrastructure) de la pigmentation par le chlorhydrate d'amiodarone.
Sem H6p Paris 48: 553, 1972
25. Labouche F, Balouet G, Daoulas R, Masse R, Le Moigne P,
Coignard A, Baret MF: Les accidents cutanes de l'amiodarone.
Arch Med Ouest 5: 37, 1973
26. Texier L, Meunier J, Gauthier Y, Dubiau JM, Gaillard G: Pigmentations cutanees accidentelles au cours de traitements par l'amio-
51
darone. Concours Medical 93: 4859, 1971
27. Satanove H: Pigmentation due to phenothiazine in high and prolonged dosage. JAMA 191: 263, 1965
28. Dysner-Aas K, Jansson H, Miorner G: Pigment deposits in eyes
and light exposed skin during long term methacycline therapy.
Acta Derm Venereol (Stockh) 54: 209, 1974
29. Wanet J, Achten G, Barchewitz G, Mestdagh G, Vastesaeger M:
Amiodarone et depots cutanes. Etude clinique et histologique. Ann
Dermatol Syph 98: 131, 1971
30. Heme N, Marion J, Brisou B, Antiglio V, Rousselot M: Pigmentations cutanees induites par le chlorhydrate d'amiodarone. Lyon
Med 226: 205, 1971
31. Vulliemin JF: Les effets secondaires cutanes de la Cordarone.
Schweiz Rundschau Med (Praxis) 62: 1426, 1973
32. Lambert D, Noble JP, Justrabo E, Hewitt J: Pigmentation cutan6e
secondaire a l'administration d'amiodarone: problemes histogenetiques. Ann Dermatol Syph 102: 277, 1975
33. Wrin P, Gendre P, Barchewitz G, Laurent-Bronchat G, Yacoubi
M, Morax S: Thesaurismose corneenne par amiodarone: donn6es
recentes. Arch Ophtalmol 31: 581, 1971
34. Ingram DV: Ocular changes during oral amiodarone therapy. In
Amiodarone and Arrhythmias, edited by Krikler DM, McKenna
WJ, Chamberlain DA. Oxford, Pergamon Press, 1983. In press
35. Babel J: Amiodarone et tissus oculaires. Schweiz Rundschau Med
(Praxis) 61: 1571, 1972
36. Dudognon P, Hauw JJ, de Baecque C, Derrida JP, Escourolle R,
Nick J: Neuropathie au chlorhydrate d'amiodarone: etude clinique
et histopathologique d'une nouvelle lipidose m6dicamenteuse. Rev
Neurol (Paris) 135: 527, 1979
37. Lustman F, Monseu G: Amiodarone and neurological side effects.
Lancet 1: 568, 1974
38. Kaeser HE: Amiodaron-neuropathie. Schweiz Med Wschr 104:
606, 1974
39. Meier C, Kauer B, Muller U, Ludin HP: Neuromyopathy during
chronic amiodarone therapy. J Neurol 220: 231, 1979
40. Touboul P, Atallah G, Gessard A, Kirkorian G: Effects of amiodarone on sinus node in man. Br Heart J 42: 573, 1979
41. Wellens HJJ, Lie KI, Bir FW, Wesdorp JC, Dohmen HJ, Durer
DR, Durrer D: Effect of amiodarone in the Wolff-Parkinson-White
syndrome. Am J Cardiol 38: 189, 1976
42. Brown AK, Primhak RA, Newton P: Use of amiodarone in bradycardia-tachycardia syndrome. Br Heart J 40: 1149, 1978
43. McGovern B, Garan H, Ruskin JN: Sinus arrest during treatment
with amiodarone. Br Med J 284: 160, 1982
44. Moysey JO, Jaggarao NSV, Grundy EW, Chamberlain DA: Amiodarone increases plasma digoxin concentrations. Br Med J 282:
272, 1981
45. McComb JM, Logan KR, Khan MM, Geddes JS, Adgey AAJ:
Amiodarone-induced ventricular fibrillation. Eur J Cardiol 11:
381, 1980
46. Krikler DM, Curry PVL: Torsade de pointes, an atypical ventricular tachycardia. Br Heart J 38: 117, 1976
47. Brochier M, Fauchier JP: Torsades de pointe et rentrees provoquees par les anti-arythmiques. Arch Mal Coeur 71: 477, 1978
Side effects of long-term amiodarone therapy.
L Harris, W J McKenna, E Rowland, D W Holt, G C Storey and D M Krikler
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Circulation. 1983;67:45-51
doi: 10.1161/01.CIR.67.1.45
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1983 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/67/1/45.citation
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/