Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
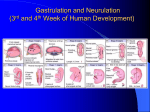
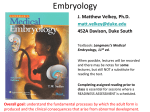
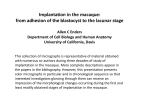
Foundation Embryology Development of bilaminar and trilaminar germ discs (ID#7070) (Second and third week of development) Dr. Narayana Kilarkaje Department of Anatomy Figures or photographs used in this presentation are originally reproduced from Langman’s Medical Embryology by T. W. Sadler, 10th Edition, Lippincott Williams & Wilkins, for teaching purpose only. Objectives • • • • • Describe the processes involved in formation of inner cell mass and trophoblast Describe the beginning of formation of germ layers from the inner cell mass Describe the formation of ectoderm, endoderm and mesoderm Describe the formation of notochord and body axis establishment Describe the growth of the embryonic disc Background- What happens in the first week? Uterus Ovary Ampulla of uterine tube Implantation Second week (day 8-14) Day 8 • The blastocyst is partially embedded in the endometrium. • The trophoblast forms 2 layers-inner layer-cytotrophoblast; and an outer layer of cells without cell boundariessyncytiotrophoblast. • Two cavities appear- blastocyst cavity (forms the primitive yolk sac) and amniotic cavity. • The inner cell mass forms 2 layers-lower hypoblast in relation with the yolk sac. The upper layer-in relation with the amniotic cavity-epiblast. • The endometrial stroma is edematous and highly vascular and filled with glycogen and lipids. • This process is called decidual reaction and the endometrium is called decidua. Days 9 and 10 Days 9 and 10 • The blastocyst is more deeply embedded in the endometrium-interstitial implantation • The penetration point on the endometrium is closed by fibrin coagulum • The vacuoles appear in the syncytiotrophoblast, and large spaces appear called lacunae • This stage of development of trophoblast is known as lacunar stage • A layer of cells probably derived from the hypoblast form a lining on the yolk sac called exocoelomic membrane (Heuser’s) Days 11 and 12 Days 11 and 12 • • • • • • • • • • The blastocyst now protrudes into the uterine lumen The trophoblast is characterized by lacunar spaces The trophoblast erodes the maternal capillaries (sinusoids) The maternal blood enters the lacunae, thus establishing utero-placental circulation A new cell layer is formed between the yolk sac and cytotrophoblast layer known as extra-embryonic mesoderm Spaces appear in the extra-embryonic mesoderm called extra-embryonic celom The extra-embryonic celom divides the extra-embryonic mesoderm into 2 layers The layer surrounding the yolk sac is called splanchnic mesoderm The layer with the trophoblast is called somatic mesoderm The bilaminar disc remains very small Day 13 Day 13 • By 13th day, the site of implantation is healed, but bleeding takes place-implantation bleeding (coinciding with 27th/28th day of an otherwise menstrual cycle) • This bleeding could be mistaken for last menstrual period, thus making it difficult to predict the expected delivery date • The trophoblast has villous like structures • The cytotrophoblast penetrates into the syncytiotrophoblast (primary villi) • The primary yolk sac transforms into secondary yolk sac, which is smaller • The extra-embryonic coelom expands and forms the chorionic cavity • The connecting stalk (later becomes the umbilical cord) suspends the embryo 0 4 No fertilization; therefore, menstruation Ovulation 14 days before next menstrual 14 28 period Menstrual period No pregnancy MP Secretory Phase Proliferative Phase Ovulation Implantation 20/ 21 day Menstrual period with pregnancy 0 4 MP MP- Menstrual period 14 MP Implantation bleeding 13 day 28 Secretory No MP Proliferative Phase Phase Fertilization Missed MP Abnormal implantation • • • • Implantation at a site other than at the normal site-most common site is the uterine tube (90%) The sites of abnormal implantation are1) In the recto-uterine cavity, 2) ampulla of the uterine tube, 3) tubal, 4) interstitial, and 5) at internal os of uterus Implantation at internal os results in placenta previa-leading to bleeding during late stage of pregnancy Ectopic pregnancy- Outside the uterus Syncytiotrophoblast produces human chorionic gonadotropin (hCG); by the end of second week, it can be detected by radioimmunoassay (pregnancy test) Third week of development - Gastrulation (Trilaminar germ disc) • Important event occurring during 3rd week is gastrulation • The gastrulation is a process by which 3 germ layers-ectoderm, mesoderm, and endoderm-are formed from epiblast • It begins with the formation of primitive streak; the latter establishes the body axis (Right-left; cranial-caudal) • It is clearly formed by 15-16 days as a narrow groove • The cephalic end of the streak is called primitive node in which a small pit is present-primitive pit • The epiblast cells migrate through the primitive pit by invagination • The cell migration is controlled by fibroblast growth factor 8 (FGF8) • The migrating cells move between the epiblast and hypoblast • The prechordal plate is formed in the hypoblast at cephalic end; no mesoderm is present at this point • This prechordal plate forms the buccopharyngeal (oropharyngeal) membrane Third week of development - Gastrulation Cranial (Prechordal plate) Left Right Caudal Primitive pit Formation of the notochord • Amniotic cavity • LS Yolk sac • • • TS • • TS • The cells from the primitive pit migrate cranially in the midline up to the prechordal plate (buccopharyngeal membrane). These cells become intercalated with hypoblast for a short time, then they get separated to form a solid cord of cells called definitive notochord. The notochord lies under (ventral) the neural tube. It forms the basis of axial skeleton. Because the migrating cells intermingle with hypoblast cells, there is a continuity for a while between the amniotic cavity and yolk sac through the neurenteric canal. The cloacal membrane is formed at the caudal end of the embryo. At both prechordal plate and cloacal membrane, the mesoderm is absent. The notochord disappears, but remains of it form the nucleus pulposus of the intervertebral disc. Growth of the embryonic disc Cephalic end • • • • • • Caudal end Initially flat and almost round, gradually becomes elongated. The cephalic end is broader and caudal end is narrower. Expansion takes place at cephalic region. Growth and elongation of the embryonic disc are caused by continuous migration of cells from the primitive streak to the cephalic region. The cell migration takes place up to 4th week, then it stops because of disappearance of primitive streak. Differentiation of germ layers begins at the middle of 3rd week in cephalic region, but at 4th week in caudal region. Teratogenesis associated with gastrulation • • • • Caudal dysgenesis (Sirenomelia) When the gastrulaton is initiated during 3rd week, the embryo is highly sensitive for teratogenic insult (critical period). Alcohol consumption at this stage causes holoprosencephaly (fusion of lateral ventricles). Anterior part of germ disc affected. Because the gastrulation takes place 2 weeks after the fertilization or 4 weeks after the last menses, pregnant woman may not know that she is pregnant- prone to risk Caudal dysgenesis (Sirenomelia): -Due to insufficient formation of the mesoderm at the caudal region. -Abnormalities are many-fusion of lower limbs, renal defects, and vertebral abnormalities. -Maternal diabetes also causes this condition in humans. Tumors associated with gastrulation • Sometimes, remnants of primitive streak or primordial germ cells (Pluripotent) persist in the sacrococcygeal region • Those cells form tumors known as sacrococcygeal teratomas • This is the most common tumor in newborns (1/37,000) • These teratomas contain tissues derived from all three germ layers Sacrococcygeal teratoma Further Reading • T. W. Sadler. Langman’s Medical Embryology 12th Edition, Lippincott Williams & Wilkins. Pages 43-62.