Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
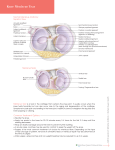
INTRODUCTION The knee joint has a structure made of cartilage, which is called the meniscus or meniscal cartilage. The menisci are the shock-absorbers of the knee - wedged horizontally in between the femur and the tibia. They fill in the in congruency between the rounded ends of the femur bone and the flattened ends of the tibia bone upon which the femur sits. Menisci are squeezed between the rounded ends of the femur (the femoral condyles or rounded ends of the thigh bone) and the flat upper surface of the tibia (the tibial plateau or upper surface of the shinbone) so they are difficult to see, and hard to explore. A torn meniscus is a disruption of the fibrocartilage pads located between the femoral condyles and the tibial plateaus. The medial and lateral meniscus provides shock absorption and plays a role in joint lubrication. Meniscal injuries are the most common surgically treated knee injury. Reported rates of meniscal injury are approximately 70 per one lakh (according to US Statistical Data). Men are affected more than women. Meniscal injuries can occur in all age groups. In older patients tears are predominantly degenerated and are commonly caused by activities of daily living, squatting or activities involving deep flexion. In younger patients up to 1/3rd of meniscal tears are sports related and are primarily caused by twisting or cutting movements, hyperflexion or trauma. In all sports with the exception of wrestling, tears of the medial meniscus occur more often than tears of the lateral meniscus. Meniscal injuries often occur in knee pathology, although with different etiologies. Such injuries may occur (i) as part of a rotational trauma, (ii) due to bending, as a result of progression of a degenerative process, or (iii) as a spontaneous injury caused by fatigue. 1 The different etiologies converge into the same symptomatology, with similar clinical manifestations and treatments, although different therapeutic results are expected. When associated with the instability of the knee or with arthrosis at an advanced stage, meniscal injury is analyzed as a function of the major pathology. The physiotherapy management of meniscal injuries involves shifting the focus of case towards increasing activity tolerance, prevention of recurrence apart from treating the pain alone. 2 DEFINITION Injuries to the crescent-shaped cartilage pads between the two joints formed by the femur (the thigh bone) and the tibia (the shin bone). The meniscus acts as a smooth surface for the joint to move on. The two menisci are easily injured by the force of rotating the knee while bearing weight. A partial or total tear of a meniscus may occur when a person quickly twists or rotates the upper leg while the foot stays still (for example, when dribbling a basketball around an opponent or turning to hit a tennis ball). If the tear is tiny, the meniscus stays connected to the front and back of the knee; if the tear is large, the meniscus may be left hanging by a thread of cartilage. The seriousness of a tear depends on its location and extent. Types The pattern of meniscus tear is important because it will determine the type of treatment receive (some tears will heal on their own, some can be treated surgically and some can't be fixed). Tears come in many shapes and sizes however there are 3 basic shapes for all meniscal tears: longitudinal, horizontal and radial. If these tears are not treated, they may become more damaged and develop a displaced tear (moving flap of meniscus). Complex tears are a combination of these basic shapes and include more than one pattern. A Longitudinal meniscus tear (circumferential tear) extends along the length of meniscus and does not go all the way through. This tear divides meniscus into an inner and outer section; however the tear generally never touches the rim of the meniscus. It tends to be more medial than lateral, and results from repeated movements. It generally starts as a partial tear in the posterior horn, which can sometimes heal on its own. However if it doesn't heal properly it can lead to a displaced longitudinal tear, known as a displaced 3 Bucket Handle tear. This is a complete tear that goes all the way through and is located near the inner rim of medial meniscus; it is often associated with a radial tear. This tear accounts for 10% of all meniscus tears, and causes the knee to lock in flexion. It is seen most often in young athletes, and happens in conjunction with 50% of ACL injuries. A Horizontal meniscus tear (cleavage tear) starts as a horizontal split deep in the meniscus. This tear divides the meniscus into a top and bottom section (like a sliced bun). It is often not visible, and moves from the posterior horn or mid section to the inside of the meniscus. This tear is rare and often starts after a minor injury from rotation in the knee or 4 degeneration. It occurs frequently in the lateral meniscus; however it is noted in both menisci. A displaced. Horizontal Flap tear can develop if the tear is overlooked or left alone. This type of tear is horizontal on the surface of the meniscus and creates a flap that flicks when the knee moves. It is a result of a strong force that tears the meniscus from the inner rim; it can easily become a complex tear. If this tear extends from the apex of the meniscus to the outer rim, one may develop a meniscal cyst (a mass that develops from a collection of synovial fluid along the outside rim of the meniscus). A Radial split meniscus tear (free-edge transverse tear) starts as a sharp split along the inner edge of the meniscus and eventually runs part way or all the way through the meniscus, dividing it into a front and back section (across the middle body instead of down the length). This tear generally occurs between the posterior horn and middle section and is seen frequently in the lateral meniscus. A small tear is difficult to notice, but when it grows and becomes a complete tear it will open up 5 and look like a part is missing. This is called a Parrot's Beak tear (displaced radial tear with a curved inner portion). It generally occurs in the thicker portion of the lateral meniscus. As it gets larger, it will catch or lock more frequently, and prevent the meniscus from protecting the cartilage during weight bearing. This tear is a result of a traumatic event or forceful and repetitive stress activities; it is often associated with other injuries. Young athletes tend to suffer from combination tears called radial/parrot beak tears (the meniscus splits in 2 directions). 6 ANATOMY Although the knee joint may look like a simple joint, it is one of the most complex. Moreover, the knee is more likely to be injured than is any other joint in the body. We tend to ignore our knees until something happens to them that causes pain. As the saying goes, however, "an ounce of prevention is worth a pound of cure." The knee is essentially made up of four bones. The femur, which is the large bone in thigh, attaches by ligaments and a capsule to tibia. Just below and next to the tibia is the fibula, which runs parallel to the tibia. The patella, or what we call the knee cap, rides on the knee joint as the knee bends. When the knee moves, it does not just bend and straighten, or, as it is medically termed, flex and extend. There is also a slight rotational component in this motion. This component was recognized only within the last 50 years, which may be part of the reason people have so many unknown injuries. The knee muscles which go across the knee joint are the quadriceps and the hamstrings. The quadriceps muscles are on the front of the knee, and the hamstrings are on the back of the knee. The ligaments are equally important in the knee joint because they hold the joint together. 7 The knee joint also has a structure made of cartilage, which is called the meniscus or meniscal cartilage. The meniscus is a C-shaped piece of tissue which fits into the joint between the tibia and the femur. It helps to protect the joint and allows the bones to slide freely on each other. There is also a bursa around the knee joint. A bursa is a little fluid sac that helps the muscles and tendons slide freely as the knee moves. To function well, a person needs to have strong and flexible muscles. In addition, the meniscal cartilage, articular cartilage and ligaments must be smooth and strong. Problems occur when any of these parts of the knee joint are damaged or irritated. The medial meniscus is semicircular and attached to the medial collateral ligament (medial collateral ligament) of the knee joint. It only moves 2-5 mm within the joint and is hence more prone to tears than the lateral meniscus which is more circular in shape and moves 9-11mm. 8 The lateral meniscus is often injured at the same time as the Anterior Cruciate Ligament (ACL), whereas the medial meniscus is itself more prone to tears in the chronically 'ACL deficient' knee Bucket Handle Meniscus Tear. Blood supply The blood supply to the menisci is limited to their peripheries. The medial and lateral geniculate arteries anastomose into a parameniscal capillary plexus supplying the synovial and capsular tissues of the knee joint. The vascular penetration through this capsular attachment is limited to 10-25% of the peripheral widths of the medial and lateral meniscal rims. In 1990, Renstrom and Johnson reported a 20% decrease in the vascular supply by age 40 years, which may be attributed to weight bearing over time. The presence of a vascular supply to the menisci is an essential component in the potential for repair. The blood supply must be able to support the inflammatory response normally seen in wound healing. Arnoczky, in 1982, proposed a classification system that categorizes lesions in relation to the meniscal vascular supply. 9 An injury resulting in lesions within the blood-rich periphery is called a red-red tear. Both sides of the tear are in tissue with a functional blood supply, a situation that promotes healing. A tear encompassing the peripheral rim and central portion is called a red-white tear. In this situation, one end of the lesion is in tissue with good blood supply, while the opposite end is in the avascular section. A white-white tear is a lesion located exclusively in the avascular central portion; the prognosis for healing in such a tear is unfavorable. 10 BIOMECHANICS The menisci provide several integral elements to knee function. These include load transmission, shock absorption, joint lubrication, and joint nutrition, distribution of load, amount of contact force and stability. The menisci act as a structural transition zone between the femoral condyles and tibial plateau. As such, they increase the congruence between the condyles and the plateau. The menisci appear to transmit approximately 50% of the compressive load through a range of motion of 0 to 90 degrees. The contact area is increased, protecting articular cartilage from high concentrations of stress. The circumferential collagen fiber orientation within the meniscus is uniquely suited to this capacity. As load is applied, the menisci will tend to extrude from between the articular surfaces of the femur and tibia. In order to resist this tendency, circumferential tension is developed along the collagen fibers of the meniscus as hoop stresses. The circumferential continuity of the peripheral rim of the meniscus is integral to meniscal function. The menisci follow the motion of the femoral condyle during knee flexion and extension. During extension, the femoral condyles exert a compressive force displacing the menisci antero posteriorly. As the knee moves into flexion, the condlyes roll back ward onto the tibial plateau. The menisci deform medial laterally, maintaining joint congruity and maximal contact area. As the knee flexes, the femur externally rotates on the tibia, and the medial meniscus is pulled forward. 11 12 AETIOLOGY All the knee injuries are more common in women than men, men experience more meniscus injuries and tears (ratio 2.5:1 (Male : Female)) this is belief to be due to men’s participation in more aggressive sports and manual activities. The peak incidence of meniscal injuries for males is between 31 – 40 years whereas for females peak incidence is in between 11 - 20 years. The two most common causes of meniscus injuries are acute trauma to the knee and degeneration of the knee joint. Occupations such as mining or carpet laying (squat position), or participation in contact sports or repetitive stress activities (such as running and skiing) or prone to meniscus injuries. Acute or traumatic meniscus damage: It can result from forceful rotating of a straight or bent knee while foot is firmly planted and bearing weight, or from hyperflexion or hyper extension of knee. These injuries are experienced most frequently in activities such as Rugby, football, baseball, soccer, basketball when one 13 twist or pivot on the knee, or slow down too quickly. The result will generally be a partial complete medical meniscus tear. This type of tear generally affects athletes or those under 40 years of age. A medial meniscus tear will frequently occur along with other injuries such as MCL or ACL tear. The combined injuries are seen most often in contact sports, when an athlete gets hit on the outside of a bend knee. A lateral meniscus tear will result more often from a knee i.e.., bent excessively and experiences full weight bearing, while the thigh bone is turning outward: seen in sports such as skiing. It can also be injured in collisions that involve deep knee bends. Degeneration of the knee joint It involves weakening of tissues with age, which results from small repetitive movements such as squatting or pivoting positions,. Or a minor meniscus injury that never healed properly. In the younger people meniscus is very flexible and pliable (like a new rubber tire) as they get 14 older it becomes less flexible and more brittle, it also develops cracks in it (like those seen in an aged car tire). Articular cartilage and meniscus detoriate as age advances, which can eventually lead to a degenerative tear without any major trauma. There will be a 20 percent decrease in blood supply to menisci by age 40 due to weight bearing over time; this inhibits body’s ability to heal itself. This wear and tear over the years may lead to an osteoarthritis condition. Approximately 60 percent of people over 65 years of age experience some form of degenerative meniscus tear. A Discoid meniscus occurs when are born with a more flat, disc shaped meniscus rather than a crescent shaped, wedge meniscus. It is generally found in the lateral meniscus and in kids less than 11 years of age. The symptoms associated with a discoid meniscus can range from very mild to continuous clicking, snapping, buckling and locking of the knee joint, decreased range of motion, joint pain and tenderness, and atrophied quadriceps (muscles wasting away). The meniscus will often change to a C-shape with maturity and Kids/teens will grow out of their symptoms; however failure of normal development can be experienced. 15 PATHOPHYSIOLOGY There are two different mechanisms for tearing a meniscus. Meniscal tears are common and can be traumatic or degenerative. Traumatic tears occur classically during twisting forces on the knee in young active people, are often vertical longitudinal tears and can be associated with ligamentous injuries. Degenerative tears occur as part of progressive wear in the whole joint, most frequently in the over 40's. These tears are usually horizontal cleavage tears or flaps and have minimal healing capacity. Tears can be described as being complete or incomplete, stable or unstable and of various patterns. Traumatic tears result from a sudden load being applied to the meniscal tissue which is severe enough to cause the meniscal cartilage to fail and let go. These usually occur from a twisting injury or a blow to the side of the knee that causes the meniscus to be levered against and compressed. A football clipping injury or a fall backwards onto the heel with rotation of the lower leg are common examples of this injury pattern. In a person under 30 years of age this typically requires a fairly violent injury although any age group can sustain a traumatic tear. Degenerative meniscal tears are best thought of as a failure of the meniscus over time. There is a natural drying-out of the inner center of the meniscus that can begin in the late 20's and progresses with age. The meniscus becomes less elastic and compliant and as a result may fail with only minimal trauma (such as just getting down into a squat). Sometimes there are no memorable injuries or violent events which can be blamed as the cause of the tear. The association of these tears with aging makes degenerative tears in a teenager almost unheard of. 16 CLINICAL FEATURES The list of signs and symptoms mentioned in various sources for Meniscus injury includes the 6 symptoms listed below: Knee pain Pain straightening knee Knee swelling Knee locking Knee clicking Knee weakness Generally, when people injure a meniscus, they feel some pain, particularly when the knee is straightened. If the pain is mild, the person may continue moving. Severe pain may occur if a fragment of the meniscus catches between the femur and the tibia. Swelling may occur soon after injury if blood vessels are disrupted, or swelling may occur several hours later if the joint fills with fluid produced by the joint lining (synovium) as a result of inflammation. If the synovium is injured, it may become inflamed and produce fluid to protect itself. This makes the knee swell. Sometimes, an injury that occurred in the past but was not treated becomes painful months or years later, particularly if the knee is injured a second time. After any injury, the knee may click, lock, or feel weak. Although symptoms of meniscal injury may disappear on their own, they frequently persist or return and require treatment. 17 INVESTIGATIONS Radiological Examination Most Common Meniscus Injury Diagnostic Tests A medical professional will sometimes recommend diagnostic testing to obtain more detailed information, and assess the amount and/or type of damage done to the knee and meniscus. There are a variety of different tests available to help them analyze the situation; however these will be dependent on injury. X – rays X-rays will provide an image of the overall structure of the knee. It is helpful in identifying abnormal bone shapes, fractures, arthritis, and degeneration (wear and tear) on the joint. It can identify a discoid meniscus, or loose bones and bone abnormalities that may mimic a torn meniscus. MRI MRI is the most powerful, accurate, and noninvasive method for diagnosing meniscal tears. It is more accurate than physical examination and has influenced clinical practice and patient care by eliminating 18 unnecessary diagnostic arthroscopies or by identifying alternative diagnosis that may mimic meniscal tears. When combined with clinical data, such as the patient's age, athletic requirements, and physical findings (e.g, possible associated ligamentous injuries), a treatment plan may be developed by assessing the need for and timing of surgery and by determining the type of surgery (meniscal debridement, rasping, repair, partial or total resection, or meniscal transplantation). MRI may be used to identify other injuries, such as ligament tears, especially ACL tears, the presence of which may also influence the decision whether to perform surgery. With MRI, physicians may obtain images in several planes, providing multiple perspectives on meniscal and ligamentous injuries. Other advantages include the following: with MRI, the patient is not exposed to ionizing radiation; MRI does not normally involve the intravenous administration of contrast material, the use of which is associated with a small but definite number of adverse effects; MRI does not require joint manipulation; MRI is painless and can be performed in less than 35 minutes; and MRI does not require the intra-articular injection of iodinated radiographic contrast material, which is needed for arthrography. MRI results lead to alterations in therapy in about one third of cases 19 Plain radiography Plain radiography is extremely limited in the assessment of meniscal tears. Radiographs may be obtained to rule out unsuspected lesions, such as osteochondritis desiccans and loose bodies. In the presence of a DM, radiographs may show widening of the medial or lateral joint compartments; hypoplasia of the lateral femoral condyle related to the increased size of the LM; a high fibular head; cupping of the lateral tibial plateau; or a squared-off lateral femoral condyle. 20 CT Scan CT or CAT scans (computerized tomography) will be used to provide a more thorough, 3-dimensional assessment of the bones and soft tissues in and around the knee joint. Further diagnostic tests such as an ultrasound, electromyogram, or arthroscopic surgery can be used to determine the degree and location of the injury if required. Physical Examination A complete examination, including that of the lower spine, ipsilateral hip and thigh, patellofemoral joint, and tibiofemoral joint, is essential when evaluating knee pain. Associated findings such as a perimeniscal cyst or ligamentous laxity suggest a higher likelihood of a meniscus injury. Important findings when examining a patient with a possible meniscus injury include the following: Joint line tenderness Joint line tenderness is an accurate clinical sign.10 This finding indicates injury in 77-86% of patients with meniscus tears. Despite the high predictive value, operative findings occasionally differ from the preoperative assessment. 21 Assess joint lines for palpable pain the location of the tenderness is not a sure sign for the type of lesion. Effusion Effusion occurs in approximately 50% of the patients presenting with a meniscus tear. The presence of an effusion is suggestive of a peripheral tear in the vascular or red zone (especially when acute), an associated intra-articular injury, or synovitis. To assess effusion perform the fluid shift test and evaluate for the presence of the fluctuation sign. The amount of effusion doesn’t indicate the presence or absence of a meniscal lesion. Range of motion The patient may have difficulty extending the knee fully if a meniscal tear blocks the motion. Full flexion, as in squatting, may be painful or impossible because of a tear. Assess the gait pattern looking for deviations or compensatory movements. Restricted motion caused by pain or swelling is also common. Girth measurement Girth measurement allow for a general assessment of effusion and atrophy. Swelling within the knee joint is measured grossly by a girth measurement taken at the joint line. Measurements taken at five Centimetre and 20 centimetre proximal to the base of the patella and 15 centimetre distal to the apex of the patella can provide and indirect indication of atrophy in the VMO segment, Quadriceps femoris muscle and calf muscles respectively. 22 SPECIAL TESTS Tests: Perform stability tests for anterior, posterior, and varus-valgus motion to rule out additional involvement of soft tissue. Several special tests may be used to assess meniscal involvement. A positive result of any test does not by itself establish the presence of a meniscal lesion, but, along with the other objective findings, such a test result can help differentiate a meniscal tear from other possible knee injuries. McMurray test This test indicates tears of the middle or posterior horn of the meniscus. With the patient supine and the hip and knee fully flexed, apply a valgus force and externally rotate the tibia while extending the knee. An audible or palpable pop or snap indicates a medial meniscal tear. Lesions of the lateral meniscus are tested by applying a varus force and internally rotating the tibia during knee extension. The snap is produced as the torn fragment rides over the femoral condyle during extension. A snap in extreme flexion is indicative of a posterior horn tear; a click at 90° of flexion indicates a lesion in the middle section of the meniscus. 23 Apley test This test is used to distinguish between meniscal and ligamentous involvement. With the patient in a prone position, the knee flexed at 90°, and the leg stabilized by the examiner's knee, distract the knee while rotating the tibia internally and externally. Pain during this maneuver indicates ligamentous involvement. Then, compress the knee while internally and externally rotating the tibia again. Pain during this maneuver indicates a meniscal tear. Bragard sign This test may be used if anterior joint-line point tenderness is present. To test for a medial lesion, the examiner extends and externally rotates the tibia, which displaces a meniscal lesion forward, if one exists. Palpable tenderness along 24 the anterior medial joint line is reduced with flexion and internal rotation. Bounce home test The patient is supine with his or her heel cupped in the examiner's hand. The examiner fully flexes the knee and then passively extends the knee. If the knee does not reach complete extension or has a rubbery or springy end feel, the knee movement may be blocked by a torn meniscus. Childress test Instruct the patient to squat with the knee fully flexed and attempt to "duck walk." If the motion is blocked, a meniscal lesion is indicated; however, pain in this position may indicate a meniscal tear or patellofemoral joint involvement. Merkel sign Instruct the patient to stand with his or her knees extended and to rotate the trunk. This movement causes compression of the menisci. Medial compartment pain during internal rotation of the tibia indicates a medial meniscal lesion. Lateral compartment pain occurring during external rotation of the tibia indicates a lateral meniscal lesion. 25 Modified Helfer test While the patient is sitting on the edge of a table with the knee flexed 90°, instruct him or her to extend the knee. If knee mechanics are within normal limits, the tibial tuberosity can be seen in line with the midline of the patella in full flexion; during extension, the tibia rotates and the tibial tubercle moves into line with the lateral border of the patella. Failure of the tibia to rotate during extension indicates a meniscal lesion or cruciate ligament involvement. O'Donoghue test With the patient prone, the examiner flexes the knee 90°. The examiner rotates the tibia internally and externally twice, then fully extends the knee and repeats the rotations. Increased pain during rotation in either or both knee positions indicates a meniscal tear or joint capsule irritation. With a valgus force to a flexed and laterally rotated knee, the medial meniscus, medial collateral ligament (MCL), and the ACL all may be injured, representing the O'Donoghue triad. Payr sign With the patient sitting cross-legged, the examiner exerts downward pressure along the medial aspect of the knee. Medial knee pain indicates a posterior horn lesion of the medial meniscus. First Steinmann sign With the patient supine and the knee and hip flexed at 90°, the examiner forcefully and quickly rotates the tibia internally and externally. 26 Pain in the lateral compartment with forced internal rotation indicates a lateral meniscus lesion. Medial compartment pain during forced external rotation indicates a lesion of the medial meniscus. Second Steinmann sign This test is indicated when point tenderness is located along the anterior joint line. When the examiner moves the knee from extension into flexion, the meniscus is displaced posteriorly, along with its lesions. The point of tenderness also shifts posteriorly toward the collateral ligament. 27 DIFFERENTIAL DIAGNOSIS Anterior Cruciate Ligament Injury: An ACL tear is a common injury that occurs in all types of sports. This injury usually occurs during a sudden cut or deceleration, as it typically is a non contact injury. Posterior Cruciate Ligament Injury: Posterior cruciate ligament (PCL) injuries are usually the result of a direct blow to the anterior part of the tibia, with a hyperextension moment at the knee. Knee osteochondritis dissecans Lumbosacral radiculopathy Osteoarthritis: Osteoarthritis (OA, also known as degenerative arthritis, degenerative joint disease), is a group of diseases and mechanical abnormalities involving degradation of joints,[1] including articular cartilage and the subchondral bone next to it. The patient increasingly experiences pain upon weight bearing, including walking and standing. As a result of decreased movement because of the pain, regional muscles may atrophy, and ligaments may become more lax. Patellofemoral joint dysfunction Rheumatoid arthritis Tendon inflammation (tendinitis) Tibial tubercle avulsion fracture 28 GENERAL PHYSIOTHERAPY ASSESSMENT OF MENISCAL INJURIES The aims of Assessment To elicitate what is preventing the patient from moving in the normal way, in order to plan the treatment. Making frequent reviews possible, so that the treatment can be altered if necessary. Recording the patient’s condition accurately for future therapeutic of statistical purposes. Subjective Assessment: Name : Age : Sex : Occupation : Address : Date of Assessment : Chief Complaints of patients: Difficulty in Straightening the knee. Difficulty in running and long walking. Pain during walking. Weakness of knee Swelling of knee Difficulty in twisting the knee joint. Difficulty in Squatting History of present illness Onset - Gradual Duration Progression Treatment taken 29 Associated Problems Diabetes Hypertension Any injury to the joint Any infection to the joint Past Medical History History of joint injury Diabetes mellitus Hypertension Present Medical History Personal History Smoker Exercise habits Alcoholic Diet Sedentary or active life style Socio economic status Type of job and nature of job Steps / Ramp / Lift Social History Pain Assessment Site of pain Side of pain Type of pain Frequency of pain Aggravating factor Relieving factor 30 Objective Assessment Vital Sign B.P. Temperature Respiratory rate Pulse rate All normal or may be some variation Observative findings Built of the patient Posture of patient Attitude of limb – Slight flexion of knee Quadriceps Atrophy Gait On Examination On palpation Swelling Warmth Bony Contour Pain Muscle wasting Effusion Crepitus Motor Examination In Acute - Normal In Chronic – Tone – Quadriceps – Flaccid. Sensory Assessment May be normal Range of motion is decreased It is of less significant as no neural involvement 31 Postural Examination Normal or Varied Gait Examination Investigations X – Ray MRI Suggested Diagnosis Meniscal injury . Range of motion Decreased Acute – Decreased Chronic – Quadriceps weakness Muscle Power Medical Research counseling 0- No Contraction 1- Flicker of contraction 2- Full range of motion in elimination of gravity 3- Full range of motion against gravity 4- Full range of motion against gravity with mild resistance 5- Full range of motion against gravity with maximum resistance Reflex Examination Normal or reduced (Knee jerk ) due to Quadriceps weakness Reflex is of less significance as there is no nerve involvement 32 Problem List Pain Swelling Tenderness Difficulty to Squat Decreased range of motion Weakness of muscle Difficult to climb stair Treatment Goals Short term goals To Reduce pain To reduce tenderness To reduce swelling Long term goals To increase the joint range of motion To increase the strength of muscle Make the patient to walk independently Moderate or Good Prognosis Follow up care 33 MANAGEMENT OF MENISCAL INJURY Non Surgical Management of Meniscal injury An acute meniscus tear can be treated with ice application, rest, anti-inflammatory medications, and physical therapy. These simple measures will help decrease swelling and pain in the joint. RICE The RICE protocol is effective for most sports-related injuries. RICE stands for Rest, Ice, Compression, and Elevation. Rest. Take a break from the activity that caused the injury. The doctor may recommend that one use crutches to avoid putting weight on the leg. Ice. Use cold packs for 20 minutes at a time, several times a day. Do not apply ice directly to the skin. Compression. To prevent additional swelling and blood loss, wear an elastic compression bandage. Elevation. To reduce swelling, recline when rest, and put the leg up higher than heart. Ultrasound therapy is a great therapeutic option to decrease pain, inflammation and soft tissue (muscle, ligament, tendon, connective and nerve tissue) damage experienced with a meniscus or knee injury. This can be received using a portable, home ultrasound device (selfadministered) or by seeing a physiotherapist. The treatment is safe, easy, painless, and generally requires between 5 10 minutes. It is based on a form of deep tissue therapy, which is generated through high frequency sound waves (that we can not hear). These waves send vibrations deep into body and raise the temperature of soft tissue. The waves are delivered through a hand held transducer and medicinal conductive gel that are used together in a slow, circular motion on skin over the injured area. Patient may experience a slight tingling or warm 34 sensation during the process as a result of the gel; this enhances the therapeutic effects of ultrasound (Phonophoresis). Ultrasound therapy increases collagen and tissue elasticity, which in turn promotes circulation (blood flow) and brings oxygen and nutrients to injured knee area. This cleans tissue by getting rid of cell waste products and allows meniscus injury to heal correctly. If not treated properly injured tissue can heal with a weakened state, which can lead to scar tissue or calcification. If used on an ongoing basis, ultrasound will help to improve range of motion by breaking down any scar tissue that may form in the knee area. Ultrasound waves penetrate deep into tissues, relax muscles, decrease chronic inflammation and accelerate recovery rate, so one can return to daily activities as soon as possible. The goals of pharmacotherapy are to reduce morbidity and prevent complications. Analgesics Pain control is essential to quality patient care. Analgesics ensure patient comfort and have sedating properties, which are beneficial for patients who have sustained injuries. Acetaminophen (Tylenol, Feverall, Tempra, Aspirin-Free Anacin) DOC for pain in patients with documented hypersensitivity to aspirin or NSAIDs, with upper GI disease, or who are taking oral anticoagulants. Nonsteroidal anti-inflammatory drugs Have analgesic, anti-inflammatory, and antipyretic activities. Their mechanism of action is not known, but they may inhibit cyclooxygenase (COX) activity and prostaglandin synthesis. Other mechanisms may exist 35 as well, such as inhibition of leukotriene synthesis, lysosomal enzyme release, lipoxygenase activity, neutrophil aggregation, and various cell membrane functions. Ibuprofen (Motrin, Ibuprin) DOC for patients with mild to moderate pain. Inhibits inflammatory reactions and pain by decreasing prostaglandin synthesis. Naproxen (Naprelan, Anaprox, Naprosyn) For relief of mild to moderate pain; inhibits inflammatory reactions and pain by decreasing activity of COX, which results in a decrease of prostaglandin synthesis. Diclofenac (Voltaren, Cataflam) Rapidly absorbed; metabolism occurs in liver by demethylation, deacetylation, and glucuronide conjugation. Delayed-release, entericcoated form is diclofenac sodium, and immediate release form is diclofenac potassium. Has relatively low risk for bleeding GI ulcers. Celecoxib (Celebrex) Primarily inhibits COX-2. COX-2 is considered an inducible isoenzyme, induced during pain and by inflammatory stimuli. Inhibition of COX-1 may contribute to NSAID GI toxicity. Seek lowest dose of celecoxib for each patient. Depending on the size and type of the meniscus tear, and the physical demands of the patient, these may be the only treatments necessary. A cortisone injection can be a helpful treatment to reduce inflammation within the joint, but it will not help heal the meniscus tear. If these treatments fail to provide relief, a surgical procedure may be recommended. 36 Surgical Management of Meniscal Tear When Surgery is Necessary If meniscus tear symptoms are not significant, surgery can often be delayed or avoided altogether. Many people live normal, active lifestyles despite having a meniscus tear. It is only when the meniscus tear becomes symptomatic, and interferes with activities, that surgery to treat the meniscus tear should be considered. Surgery has the best results when the primary symptoms of the meniscus tear are mechanical. This means that the meniscus tear is causing a catching or locking sensation of the knee. Operative management Once a decision has been made to proceed with operative management, further decisions regarding the surgical treatment of the meniscus tear need to be made Intraoperatively, a decision has to be made whether to repair, excise, or leave the tear in the meniscus alone. Arthroscopic Meniscectomy for Meniscus Tears: A meniscectomy is a procedure to remove the torn portion of the meniscus. This procedure is far more commonly performed than a meniscus repair. The meniscectomy is done to remove the damaged portion of meniscus, while leaving as much healthy meniscus as possible. The meniscectomy usually has a quick recovery, and allows for rapid resumption of activities. 37 Arthroscopic probing of a posterior horn complex meniscal tear with multiple flaps. Arthroscopic view of medial meniscus after excision of flap tear. Meniscus Repair In some situations, surgeon may offer a meniscus repair as a possible surgery for damaged or torn cartilage. Years ago, if a patient had torn cartilage, and surgery was necessary, the entire meniscus was removed. These patients actually did quite well after the surgery. The problem was that over time, the cartilage on the ends of the bone was worn away more quickly. This is thought to be due to the loss of the 38 cushioning effect and the diminished stability of the joint that is seen after a meniscus is removed. When arthroscopic surgery became more popular, more surgeons performed partial menisectomies. A partial meniscectomy is performed to remove only the torn segment of the meniscus. This works very well over the short and long term if the meniscus tear is relatively small. But for some large meniscus tears, a sufficient portion of the meniscus is removed such that problems can again creep up down the road. How is the meniscus repair performed? Techniques of meniscus repair include using arthroscopically placed tacks or suturing the torn edges. Both procedures function by reapproximating the torn edges of the meniscus to allow them to heal in their proper place and not get caught in the knee causing the symptoms. Meniscus Transplantation Meniscus transplantation consists of placing the meniscus from a donor patient into an individual who has had their meniscus removed. The ideal patient for a meniscus transplant is someone who had their meniscus removed, and subsequently begins to develop knee pain. Meniscus transplant is not performed for an acute meniscus tear, rather it is performed when removal of the entire meniscus has caused persistent pain in the knee. 39 Physiotherapy Management A meniscus tear is a common knee joint injury. The knee will heal and whether surgery will be needed depends in large part on the type of tear and how bad the tear is. Rehabilitation Program A rehabilitation program helps to regain as much strength and flexibility in knee as possible. Rehabilitation program probably will include physical therapy and home exercises. The goals of rehabilitation are to restore range of motion, strength, and endurance of the knee. A rehabilitation program usually includes treatment with a physical therapist at a therapy center and home treatment in home or at a gym or health club. Physical therapist will design a program that guides through exercises to reach these goals on a schedule that takes into account health status, age, and activity expectations. Recovery from a meniscus tear depends on many factors. If the tear is minor and symptoms go away, doctor may recommend a set of exercises to increase flexibility and strength. Rehabilitation following meniscectomy Initial phase When the patient first reports to outpatient physical therapy 4-7 days after surgery, he or she usually is able to bear full weight or as much weight as tolerated on the involved leg. Modalities are used as needed to decrease pain or swelling, including heat/ice contrasts, ice alone, transcutaneous electrical nerve stimulation (TENS), electric galvanic stimulation, and Ultrasound. As needed, the patient should perform flexibility exercises for the lower extremity musculature, 40 including the hamstrings, quadriceps femoris, hip flexors, hip adductors, and calf muscles. Static Quadriceps Contractions This exercise is used to prevent quadriceps muscle degeneration and weakening in the acute stages of injury and/or directly after injury. In this stage weight bearing or more difficult exercises may be either not advised or too difficult. This exercise may be started as soon as pain will allow and can be done on a daily basis. Contract the quadriceps muscles at the front of the thigh, keep toes pointed to the ceiling. Hold for 10 seconds. Relax and rest for 3 seconds. Repeat 10 to 20 times. This can be performed either flat on the floor, or with a foam roller or rolled up towel under the knee. Static Hamstring Hold This exercise is used to maintain the strength of the hamstring muscles when other exercises may be too difficult. Again it may be started as soon as pain will allow and can be done on a daily basis. Lie on the stomach Bend the knee to raise the foot up to about 45 degrees 41 Hold for count of 10 and lower slowly . Repeat 10 to 20 times. This can be progressed by increasing the length of hold, as well as using some external force such as a partner to increase the resistance or ankle weights. Static Hamstring Contractions This exercise is more difficult than the one above and also helps in increasing the range of movement in the knee joint. This involves contracting the hamstring muscles without movement - by pushing against a static object. One can do this by attempting to either bend the knee or extend the hip, or both. The easiest way of doing this is getting a partner to resist the movement. One can also push against a wall, chair or the floor. Hold for 10 seconds. Relax and rest for 3 seconds. Repeat 10 to 20 times. 42 Straight Leg Raises (SLR) This exercise is more difficult than the static quadriceps exercise as it involves lifting the entire weight of the leg against gravity. It mainly targets the knee extensors (the quadriceps) but also functions in strengthening the hip flexors (Rectus Femoris and Iliopsoas muscles). Position the patient sitting on the floor with both legs straight out in front of the therapist. Keeping the knee completely straight, lift the entire leg off the floor Hold for 10 seconds. Relax and rest for 3 seconds. Repeat 10 to 20 times. 43 Knee Extension This exercise specifically targets the quadriceps muscle group. It may be used relatively early in the rehab process but care should be taken not to overload the injured leg. Always seek professional advice before beginning weight training Always start each session with a light warm-up set of repetitions before increasing the weight or resistance. Keeping your bottom firmly on the bench, straighten and lower the injured leg in one smooth movement. An alternative exercise involves using a resistance band to provide the resistance. Tie one end of the band to a table leg or other stable structure Leg Curl Again, this exercise strengthens the hamstring muscles. You can perform this with either ankle weights, a resistance band or a weight machine. If using ankle weights or a resistance band, lay on your front. Attach the band around your ankle and also around something sturdy, close to the floor behind you. 44 Always start resistance band exercises with the band just under tension, if it is slightly slack, shorten the length you are using by tying it shorter. Bend the knee, bringing the heel towards your buttocks, as far as you comfortably can. Slowly reverse this movement and return to the starting position under control. Aim for 3 sets of 10 repetitions initially with light weights/low resistance and gradually increasing. Hip Raises (Bridging) Lie on your back with your knees bent and feet flat on the floor. Lift your hips up off the floor as far as they will go, hold for 3 seconds and lower. Repeat 10 to 20 times. To progress this exercise, increase the length of time that the hips are held up, initially to 5 and then to 10 secs 45 Calf Raises Raise up and down on the toes on the edge of a step in a smooth movement > Play video Aim for 3 sets of 20 repetitions. This exercise can be progressed to single leg calf raises as fitness and tolerance increases Squatting This is arguably the best exercise to increase quadriceps muscle strength. Nevertheless, extreme care should be taken with this exercise as it involves large loading of the quadriceps muscles and the knee joint itself Squat down half way to horizontal and return to standing. Try to sink down through the knees, keeping the back straight and not allowing your knees to move forwards past your toes Return to the start position and repeat . Aim for 3 sets of 10 repetitions during rehabilitation. Progress this exercise by adding weight or moving to single leg squats. Later in the rehabilitation process, squats can be progressed to horizontal (90 degrees flexion at knee and hip) 46 Hip Flexor Exercises Start with the band tied around your ankle and also something close to the floor. Make sure you have something to hold on to. Raise the knee up towards the chest, against resistance Slowly return to the start position and repeat. Aim for 3 sets of 10 repetitions. If one do not have rehabilitation band or suitable weights then this exercise can be done without resistance. However in this situation more reps should be added to the rehab program. 47 Hip Adduction Exercises The hip adductors are better known as the groin muscles. Attach a resistance band around your ankle and then fasten it to a secure object, to the side of you. Start with the leg out to the side, away from the body, with the knee straight. Pull the leg across your body as far as comfortable, before slowly returning back to the start position Hip Abduction Exercises The hip abductors are vital components in gait as they allow the hips to support the weight of the body. Thus strengthening exercises for this muscle group is vital to any lower limb rehabilitation program. These can be performed in lying in the acute stage and progressed into standing with a resistance band. Tie the band around your ankle and around a sturdy object to the side of you. Start with the leg to be worked on the opposite side to the attachment point 48 While keeping the leg straight, take leg out to the side as far as comfortable Slowly return to the start position. This exercise can be progressed using elastic bands to increase resistance. Intermediate phase The patient should have full ROM to begin this phase. Modalities are continued as indicated by symptoms. Flexibility and strengthening exercises are continued, increasing resistance as tolerated. If the quadriceps femoris muscle is strong enough (i.e, if the patient can lift 10 lb during short-arc quadriceps femoris muscle exercise), the running program may be initiated. The first stage of the running program is jogging in place on a trampoline. Unless pain or swelling occurs, the patient gradually progresses to jogging for 10-15 minutes. Advanced phase During the advanced phase, the patient continues to progress in strength-training exercises while beginning to return to sports activities. Track running may begin when the patient is able to run on the treadmill for 10-15 minutes at a pace of 7-8 minutes per mile (depending upon the 49 patient's previous activity level). Once mileage on the track has reached 2-3 miles, agility drills and sport-specific activities may be performed. Proprioceptive Exercises Proprioception can be considered as the body's ability to sense where it is in space. In the event of an injury this mechanism becomes disrupted and proper training is needed to re-educate the muscles to fire at the right time to allow further injury prevention. The most common way to achieve this is to first stand and then walk on an uneven surface. As balance continues to improve proprioceptive exercises can progressed as follows: Two footed stand on wobble board -aim to maintain balance for as long as possible Progress to one legged (injured side) wobble board exercises Practice hopping on the injured leg on an uneven surface Gradually increase difficulty by throwing a ball against a wall and catching it while standing on the wobble-board. Aim to challenge yourself by throwing the ball outside your comfortable center of gravity. Proprioceptive exercises should be continued even after a return to full fitness to prevent future injury. Below is an example of a muscle strengthening program following a meniscal tear or surgery. As with all rehabilitation programs, the type of exercises, their frequency and intensity is dependant on the patient's own functional ability and will vary from person to person. Hence the below table offers only sample information and figures and should only be carried out as pain allows. 50 Phase Rehabilitative Strengthening Exercises Daily Routine (Repetitions X Daily Frequency) Functional Activities 1 10 X 3 In some cases non-weight 1.Static Quadriceps Week 0 10 X 3 bearing on the injured leg is 2.Static Hamstrings Pre5X2 advised. Use crutches if 3.SLR’s operation necessary 2 1. Static Quadriceps 10 X 3 Week 0-1 2. Static Hamstrings 10 X 3 Carry out weight bearing After using therapeutic elastic 5X3 status as advised by Surgery band 5X3 surgeon. 3. SLR's 10 X 3 If weight bearing has been 4. Double Calf Raises 10 X 3 advised, concentrate on gait 5. Hip Abduction re-education drills. 6. Hip Flexion 3 1.Leg raises using 10 X 3 Weeks 1- therapeutic elastic 5X3 2 band 5X3 Light Cycling and swimming 2.Half-way Squats 5X3 as pain allows 3.Small range lunges Twice Daily 4.Single calf raises 5.Proprioceptive drills 4 1.Full Squats 10 X 2 Some light jogging and Weeks 2- 2.Full range Lunges 10 X 2 perhaps short range sprints 3 3.Single leg squats 5X3 may be attempted at this 4.Proprioceptive drills 3 Times Daily stage. 5.Change of direction Once Daily Increase resistance on drills cycling machine 5 1.Full Squats 10 X 3 At this stage it may be Weeks 3- 2.Full Lunges 10 X 3 possible to return to sport 5 (extra weights may be specific training. Care should added to shoulders to 3 times daily be taken when returning to increase difficulty of Once Daily contact or impact sports. these exercises) Short intervals are advised 3.Proprioceptive drills rather than over exertion in 4.Sprinting drills with the early period of return. change of direction Non Surgical rehabilitation The program for non operative rehabilitation is similar in principle to the program that follows meniscectomy. Cryotherapy and nonsteroidal anti-inflammatory drugs (NSAIDs) play a very important role in the management of non operative meniscal injury. These medications help control the amount of swelling and provide some pain relief. Sometimes, aspiration is useful to decrease the effusion, and, rarely, an athlete may need a judicious 1-time corticosteroid injection. Although not routinely 51 advocated, an injection may provide an athlete with a way to control the irritation within the knee so that performance may not falter. Maintenance of ROM of the knee is important, as are muscular strength and endurance. A reasonable goal before return to athletic activity is strength of the injured lower extremity within 20-30% of the contra lateral side. Initially, activity modification is useful, particularly in athletes who are "weekend warriors." The time frame for return to activity depends on a number of factors. Returning to competition depends on the demands and motivation of the athlete, as well as on the severity of the meniscal tear. 52 PROGNOSIS Prognosis A torn meniscus is certainly not life threatening and once treated, the knee will usually function normally for many years. A meniscal tear that catches, locks the knee, or produces swelling on a frequent or chronic basis should be removed or repaired before it damages the articular (gliding) cartilage in the knee. A meniscal tear that produces discomfort but does not produce any of the symptoms mentioned above may be less likely to damage the rest of the knee. One may choose to "live" with this type of meniscal tear instead of treating it operatively. Following a partial menisectomy most patients are able to resume to normal non-sporting activities comfortably in a few days. Generally light sports such as biking and swimming are well tolerated in 1-2 weeks. Heavy sports such as running, basketball and tennis usually take longer. The long-term prognosis depends on how much meniscus was lost from the tear. Naturally occurring (aging) arthritis is accelerated depending on the amount of meniscus lost. There are new techniques designed to repair those menisci that are repairable and replace that portion of the meniscus which is lost. Entire menisci can be replaced using cadaver transplants. 53 PREVENTION Although it is important to be able to treat meniscus injury, prevention should be your first priority. Some of the things you can do to help prevent a meniscus injury 1. Warm Up properly A good warm up is essential in getting the body ready for any activity. A well-structured warm up will prepare your heart, lungs, muscles, joints and your mind for strenuous activity. 2. Avoid activities that cause pain This is self-explanatory, but try to be aware of activities that cause pain or discomfort, and either avoid them or modify them. 3. Rest and Recovery Rest is very important in helping the soft tissues of the body recover from strenuous activity. Be sure to allow adequate recovery time between workouts or training sessions. 4. Balancing Exercises Any activity that challenges your ability to balance, and keep your balance, will help what is called, proprioception: - your body's ability to know where its limbs are at any given time. 5. Stretch and Strengthen To prevent meniscus injury, it is important that the muscles around the knee be in top condition. Be sure to work on the strength and flexibility of all the muscle groups in the leg. 6. Footwear Be aware of the importance of good footwear. A good pair of shoes will help to keep your knees stable, provide adequate cushioning, and support your knees and lower leg during the running or walking motion. 7. Strapping Strapping, or taping can provide an added level of support and stability to weak or injured knees. 54 CASE ASSESSMENT – 1 Name : P. Sujatha Age : 40 years Gender : Female Occupation : House wife Address : Rapur Chief complaints : Pain around right knee joint Pain increases during night Difficulty in walking and stair climbing Presence of Swelling around right knee joint History Present History : Pain around right knee joint and increases during night Past History : She had a fall from height and got direct injury to knee Medical History : She has taken analgesics for pain relief Surgical History : No Surgical history Personal History : No history of Hypertension and Diabetes Mellitus Pain Assessment Site : Around knee joint Side : Right Side Duration : One Month Character of pain : Not Radiating Aggravating Factors : During movement and walking Relieving Factors : At Rest 55 VAS Scale: On Observation Built : Moderate Attitude of Limb : Slightly flexed Skin Colour changes : No Changes Seen External Appliances : No usage Tenderness : Grade II Muscle Spasm : Present Warmth : Present Swelling : Present On Palpation On Examination Range of motion of knee joint. Passive: Movement Right knee Left knee Flexion 0-110 Degrees 0- 130 degrees Extension 110- 0 Degrees 130- 0 Degrees Active: Movement Right knee Left knee Flexion 0-100 Degrees 0- 130 degrees Extension 100- 0 Degrees 130- 0 Degrees Manual muscle testing Muscles Right knee Flexors Grade – 4 Extensors Grade – 3 Deep Tendon Reflexes Left knee Grade – 5 Grade – 5 Jerk Right Left Knee + ++ Ankle ++ ++ Plantar ++ ++ 56 ADL : Activities like walking and stair climbing is difficult Special Test : Apley’s grinding test – Positive Mcmurray test- Positive Lachman’s Test – Negative Anterior Drawer Test - Negative Investigations X- Ray : Bony abnormalities are seen MRI : Meniscal tear Provisional Diagnosis : Meniscal Injury Pain : Ultra Sound, TENS, Cryotherapy Swelling : Crep bandage, Elevation of limb Joint Movement : Limb mobilization Muscle strength : Isometrics to hamstrings, Treatment Isometrics to Quadriceps Straight Leg Raises Leg Extension exercises Home Programme Static and dynamic quadriceps exercises are taught Stair climbing is advised to avoid. Prognosis Pain get decreased Range of motion get increased ADL activities like walking and stair climbing are improved. 57 CASE ASSESSMENT - 2 Name : K. Arjun Age : 35 Years Gender : Male Occupation : Sports Master Address : Podalakur Chief complaints : Pain around left knee during walking Weakness is felt Difficulty in Walking Difficulty in stair climbing Decreased movement History Present History : Pain around left knee during walking Weakness is felt Decreased movement Past History : He had a slip during foot ball play and under gone surgery before two months Medical History : Analgesics for pain relief Surgical History : He had surgery before two months Personal History : No History of hypertension and Diabetes Mellitus Pain Assessment Site : Around Knee Side : Left side Duration : Two months Character of pain : Not Radiating Aggravating Factors : During movement and at work Relieving Factors : At Rest 58 VAS Scale: On Observation Built : Moderate Attitude of Limb : Slightly flexed Skin Colour changes : Not Seen External Appliances : No Usage Tenderness : Grade II Muscle Spasm : Positive Warmth : Positive Swelling : Positive On Palpation On Examination Range of motion of knee joint. Passive Movement Right knee Left knee Flexion 0-130 Degrees 0-110 Degrees Extension 130-0 Degree 110-0 Degrees Active Movement Right knee Left knee Flexion 0-130 Degrees 0-100 Degrees Extension 130-0 Degree 100-0 Degrees Manual muscle testing Muscles Right knee Flexors Grade – 5 Extensors Grade – 5 Deep Tendon Reflexes Left knee Grade – 3 Grade - 3 Jerk Right Left Knee ++ + Ankle ++ ++ Plantar ++ ++ 59 ADL : Activities like walking, stair climbing, jumping are difficult. Investigations Provisional Diagnosis : Post operative Knee pain Pain : Ultra Sound, IFT, Cryotherapy Swelling : Crep bandage, Elevation of limb Treatment Week 0-1 after surgery : Static Quadriceps Static hamstrings Straight leg raises Calf raises Hip abduction Hip Flexion Week 1-2 after surgery : Half way squats Lunges Single Calf raises Proprioceptive exercises Week 2-3 after surgery : Full squats Full lunges Proprioceptive exercises Single leg squat Week 3-5 after surgery : Full squats Full lunges Proprioceptive exercises Home Programme Static and dynamic quadriceps exercises are taught Stair climbing is advised to avoid. Prognosis Pain get decreased Range of motion get increased ADL activities like walking, stair climbing and jumping are improved 60 CONCLUSION Meniscal tears are common and can be part of degenerative change within the knee joint or secondary to trauma. They can cause symptoms that affect the function of the joint and require surgical intervention. The majority of symptomatic tears require arthroscopic partial meniscectomy but in a few select cases the tear may be amenable to repair done as an open or arthroscopic procedure. Effective rehabilitation should be there for spontaneous recovery. Rehabilitation interventions seek to promote recovery and independence in daily activity, to promote better health and prevent secondary complication. The utilization of effective treatment intervention focus on real life environments can cause successful attainment of functional outcomes. By the proper rehabilitation programme treated for five weeks of the present case with meniscal injuries have been shown to improve functional outcome and allowed the patient to regain independence in daily life. It is concluded that, with proper rehabilitation program, we can regain patient functional activity to maximum level and prevent secondary complication. 61 BIBLIOGRAPHY Achleshwar Gandora “Gross Anatomy”, 1st Edition, 2000, Jaypee Brothers Medical Publications B.D. Chaaurasia’s “Human Anatomy”, 4th Edition, 2004, Satish Kumar Jain for CBS Publishers and Distributors. Caralyn Kisner “Therapuetic Exercises” 4th Edition, 2002, Jaypee Brothers Medical Publications. Chaudhari “Medical Physiology” 2nd Edition, New Central Book Agency (Pvt.,) Ltd., C. Rex “Clinical Assessment and Examination in Orthopaedics”, 1st Edition, 2002 Jaypee Brothers Medical Publications. Colour Atlas of Clinical Orthopaedics, 2nd Edition, Jones, Owen. Mosby Wolfe Publishers. Cynthia C. Norkins Mela D. Levangie “Joint Structure and Funciton” 2nd Edition, 2001 Jaypee Brothers Medical Publications. David J. Magee “Orthopaedic Physical Assessment”. Jayant Joshi & Prakash Kotwal “Essential of Orthopaedics & Applied Physiotherapy” 2007 Published by Elsevier Pvt. Ltd., John Ebinezer “Text Book of Orthopaedics” 2nd Edition 2000, Jaypee Brothers Medical Publications. 62 Caren Atikison Fionacaults Anne Marie Hassen Kamp “Physiotherapy in Orthopaedics” 2nd Edition, 2005 British Library Cataloging in publication Data. Maheswari “Essential Orthopaedics” 3rd Edition May 2005 Mahata Publishers. Natarajan’s “Text book of Orthopaedics & Traumautology” 6th Edition, 2005, All India Publishers and Distributors. Patricia A. Downie “Cash Text Book of Orthopaedics & Rheumatology for Physiotherapy” 1st Edition, Jitten Dar P Vij for Jaypee Brothers Medical Publications. Stuart B. Povter “Tidy’s Physiotherapy” 13th Edition Published by Elsevier Pvt., Ltd., S.Sundar’s “Text Book of Rehabilitation” 2nd Edition Jaypee Brothers Medical Publications. 63