Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
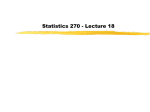
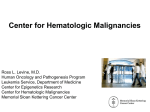
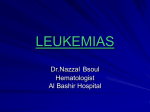
Case Study: Patient with MF has Increasing Blasts, but Not Yet AML -- What to Do? John Mascarenhas, MD Myeloproliferative Disorders Program Tisch Cancer Institute, Division of Hematology/Oncology Mount Sinai School of Medicine New York, New York Co-Presenters Jeffrey C. Bryan, PharmD, RPh Clinical Pharmacy Specialist, Leukemia Division of Pharmacy, University of Texas MD Anderson Cancer Center Houston, TX Otitolola Arterbery, MSN, RN, OCN Clinical Nurse MD Anderson Cancer Center Houston, TX Evolution of Myeloproliferative Neoplasms (MPNs) to Acute Myeloid Leukemia • In general, MPNs are chronic diseases, but some patients have clinical signs of disease progression • Leukemic transformation is a major complication1 – Median survival, 3-6 months – Not meaningfully altered with induction chemotherapy • For patients with myelofibrosis (MF), AML is the most common cause of death2 1. Rampal R, Mascarenhas J. Curr Opin Hematol. 2014;21:65-71; 2. Cervantes, et al. Blood. 2009;113(13):2895-901. Patient Case Study: Michael G. • 54-year old man, diagnosed with JAK2V617F mutation-positive primary myelofibrosis (DIPSS Int-1 risk), was treated with hydroxyurea to manage spleen discomfort. • Four years later (2011), spleen size had increased to 8 cm below the left costal margin. He had fatigue and weakness, drenching night sweats, and 3 episodes of unexplained fever in the past 2 months. Patient Case Study: Michael G. • Re-assessed as DIPSS Int-2 – [4 risk factors, constitutional symptoms (1), Hb <10 g/dL (2), blood blasts 2% (1 [ie, ≥1%]]. • Switched from HU to JAK inhibitor therapy (ruxolitinib) and has done well, with reduced splenomegaly and improvement in constitutional and spleen related symptoms. Case Study (cont.): Michael G. • At a recent visit (1.5 years later), he complained of profound fatigue and weakness and unintentional weight loss. – Hematologic values: WBC 24.5 x 109/L; Hb 10.5 g/dL; platelets 75 x 109/L – Increased myeloid forms on the peripheral blood smear. • 12% blasts by manual count; confirmed by flow cytometry to be myeloblasts. • Bone marrow biopsy – Distorted marrow architecture – Immunohistochemical staining confirmed presence of myeloblasts. Case Study (cont.): Michael G. Q: Does this patient have post-MF AML? A. Yes B. No C. Maybe Case Study (cont.): Michael G. Q: Does this patient have post-MF AML? A. Yes B. No C. Maybe This patient has 12% peripheral blasts – Accelerated phase, but not yet blast phase (AML) Criteria for Leukemic Transformation of MPNs MPN Disease Phase Definition 1 Leukemic transformation (blast • ≥20% blasts in peripheral blood or phase [MPN-BP]) bone marrow Accelerated phase (MPN-AP) Mesa RA, et al. Leuk Res 2007; 31:737–740. • No consensus; ≥10% to <20% blasts widely considered to be in AP • Various degrees of pancytopenia Caring for the Patient with Progressing MF Increased need/frequency of: • Supportive care to manage symptoms caused by low levels of blood cells (bone marrow ‘burns out’) – Medications may include: • Erythropoietin (EPO) to increase red blood cells (RBCs) • Granulocyte colony-stimulating factor (G-CSF) or granulocyte macrophage colony-stimulating factor (GM-CSF) to increase white blood cells (WBCs) • Systemic antibiotics and antiviral drugs to fight infections that the patient’s own WBCs cannot adequately fight on their own – Transfusions to add RBC or platelets if the response to medications is insufficient Caring for the Patient with Progressing MF Increased need/frequency of (cont.): • Monitoring and surveillance by lab visits, office visits, phone calls to patient – hematology, symptoms, performance status • Multidisciplinary care (eg, dietary changes, counseling, support programs, in-patient care if hospitalized) • Patient education (eg, resources on advanced-stage MF; medication changes, HSCT) Q: Within 10 years of PMF diagnosis, what percentage of patients will develop leukemic transformation (MF-BP)? A. 1% B. 5% C. 10% D. 20% E. 50% Q: Within 10 years of PMF diagnosis, what percentage of patients will develop leukemic transformation (MF-BP)? A. 1% B. 5% C. 10% D. 20% E. 50% Rate of Transformation from an MPN to Acute Myeloid Leukemia MPN Subtype at Diagnosis 10-year Leukemic Transformation Rate* Essential thrombocythemia (ET) 1% Polycythemia vera (PV) 4% Primary myelofibrosis (PMF) 20% *From time of MPN diagnosis Rampal, Mascarenhas. Curr Opin Hematol. 2014;21:65-71 Comparison of Blast Transformation Rates Among MPNs (N=826) Tefferi A et al. Blood. 2014; 124(16): 2507–2513. Risk Factors for Leukemic Transformation in Patients with MPNs • PV - Age >70 years or prior exposure to P-32, busulfan, or pipobroman1 • ET - Anemia or platelet >1000 x 109/L2 • MF – Leukocytes >30 x 109/L or abnormal karyotype 3 – PB blasts ≥3% or platelet count < 100 x 109/L4 – Time to development of hemoglobin <10 g/dL, leukocytes >30 x 109/L, platelets <150 x 109/L5 – BM blasts >10% or high-risk karyotype6 – Splenectomy, platelet count <100 x 109/L, PB blasts ≥1% 7 – BM blasts >10%, platelet count <50 x 109/L, chromosome 17 abnormalities (define MF-AP as a necessary step to MF-BP) 8 – Monosomal karyotype9 – Triple-negative mutational status 10,11 1. Gangat N, et al. Leukemia 2007; 21:270–6; 2. Finazzi G, et al. Blood 2005; 105:2664–670; 3. Dupriez B, et al. Blood 1996;88:1013–8; 4. Huang J, et al. Cancer 2008; 112:2726–32; 5. Morel P, et al. Blood 2010;115:4350– 5; 6. Quintas-Cardama A, et al. Clin Lymphoma Myeloma Leuk 2013; 13:315–8; e2; 7. Barosi G, et al. Blood 1998; 91:3630–6; 8. Tam CS, et al. Blood 2008; 112:1628–37; 9. Vaidya R, et al. Blood 2011; 117:5612–5615; 10. Tefferi A et al. Blood. 2014; 124(16): 2507–13; 11. Rumi E et al. Blood 2014;124:1062-9. Effect of Driver Mutations on Incidence of Leukemic Transformation in PMF Rumi E et al. Blood 2014;124:1062-1069. Case Study (cont.): Michael G. • Based on the finding of 10% blasts, our patient’s MF is in the ‘accelerated phase’ (MF-AP), and not yet full transformation into acute leukemia (MF-BP; defined as at least 20% blasts). • His JAK2V617F allele burden increased to 45%; also showed an aberration of chromosome 9p, and an acquired a TET2 mutation (an epigenetic modifier). Q: Does this new genetic information change whether or not his disease in blast phase? A. Yes B. No Case Study (cont.): Michael G. Q: Does this new genetic information change whether or not his disease in blast phase? A. Yes B. No Patient’s profile is still consistent with accelerated phase (defined by up to 20% blasts, not by cytogenetic or mutational status – although some karyotypes may be indicative of poorer prognosis) The process of leukemic transformation is thought to arise from the accumulation of additional genetic events in addition to mutations in the JAK-STAT pathway. Additional mutations are often seen in accelerated phase. Additional Mutations Are Often Seen in MF-AP and MF-BP • The number of chromosomal abnormalities differs between chronic phase MF, MF- AP, and post-MF AML (MF-BP) Klampfi T, et al. Blood 2011;118:167-76. Spectrum of Mutations in MPN-BP and De-novo AML Rampal, Mascarenhas. Curr Opin Hematol. 2014;21:65-71. Possible Mechanisms of MPN Evolution to AML (BP)1,2 • An MPN with wt JAK2 may develop JAK2 mutation • JAK2V617F mutations are not always retained2 1. Rampal, Mascarenhas. Curr Opin Hematol. 2014;21:65-71. 2. Tam CS et al. Blood. 2008;112: 1628-37. Case Study (cont.): Michael G. Q: This 60-yr-old patient with PMF is taking ruxolitinib to manage his splenomegaly and constitutional symptoms. He has progressed to accelerated phase, but not yet blast phase. What would you do? A. Continue on ruxolitinib B. Discontinue ruxolitinib immediately and proceed directly to allogeneic hematopoietic stem cell transplant C. Switch from ruxolitinib to low-intensity AML therapy (eg, azacitidine, low-dose ara-C) D. Induction chemotherapy for de novo AML E. Clinical trial F. Supportive care only Case Study (cont.): Michael G. Q: This 60-yr-old patient with PMF is taking ruxolitinib to manage his splenomegaly and constitutional symptoms. He has progressed to accelerated phase, but not yet blast phase. What would you do? A. Continue on ruxolitinib B. Discontinue ruxolitinib immediately and proceed directly to allogeneic hematopoietic stem cell transplant C. Switch from ruxolitinib to low-intensity AML therapy (eg, azacitidine, low-dose ara-C) D. Induction chemotherapy for de novo AML E. Clinical trial F. Supportive care only Combination Strategies: Ruxolitinib and DNA Methyltransferase Inhibitor in PMF Patients with Elevated Blasts • Combination evaluated in 3 symptomatic patients with cytopenias and elevated blast* counts – Median age 80 years (range: 60 – 88) – All had JAK2 V617F mutation – 2 had PMF and 1 had post-ET MF • Clinical trials are investigating combinations of:2 • Ruxolitinib and azacitidine in patients with Int-2 or high-risk MF requiring therapy (NCT01787487). • Ruxolitinib and decitabine in patients with MPN-AP/MPN-BP (NCT02076191) Tabbaroki A et al. Leukemia & Lymphoma, 2014; Early Online: 1–3; 2. Mascarenhas J. Best Prac Res Clin Haematol. 2014;27:197-208. Treatment Options for MF-AP or MF-BP • There is no ‘standard of care’ and treatment options are very limited. • Patients with severe or advanced MF may be treated with bone marrow transplantation (HSCT). This is currently the only treatment with the potential to cure MF transformed to leukemia.1 • Leukemia treatments may be given with the aim of achieving a favorable response that allows completion of HSCT2 1. Alchalby H, et al. Biol Blood Marrow Transplant. 2014 Feb;20(2):279-81; 2. Cervantes F. Blood. 2014;124(17):2635-42. Median Survival by Treatment Strategy for MPN-BP Mesa, 2005 Tam, 2008 Kennedy, 2013 Passamonti, 2005 Noor, 2011 Thepot, 2010 Entire cohort 2.7 mo 5 mo 6.6 mo 2.9 mo 4.6 mo - Induction chemotherapy 3.9 mo 6 mo 9.4 mo b 5.6 mo 6 mo - Induction chemotherapy and HSCT - - 47 mo - 10.5 mo Low-intensity therapy (eg, JAK2 inhibitor, DNA hypomethylating agent) a 2.9 mo 7 mo 6.6 mo - - 8 mo Supportive therapy 2.1 mo 1.5 mo - 2.5 mo 1.9 mo - a Category B Includes also includes alkylating agents, vincristine, low-dose cytarabine, gemtuzumab. only those MPN-BP patients who achieved CR/Cri Reviewed in Rampal, Mascarenhas. Curr Opin Hematol. 2014;21:65-71. Mesa RA, et al. Blood 2005; 105:973–7; Tam CS, et al. Blood 2008; 112:1628–37; Kennedy JA, et al. Blood 2013; 121:2725–33; Passamonti F, et al. Cancer 2005; 104:1032–6; Noor SJ, et al. Leuk Res 2011; 35:608–13; Thepot S, et al. Blood 2010;116:3735–42. Starting a New Oral Medication: Pharmacy Perspectives Chemotherapy drugs (like those used for AML) may be prescribed for MF patients who are in BP (and sometimes in AP) • Understand the planned treatment transition strategy/ timing to ensure medications are available as needed • Screen for possible drug-drug interactions based on patient’s medication record • Discuss treatment costs, including the patient’s responsibility; identify assistance program if needed • Patient education – How to take the medication – Drug-specific side effects that might develop, what to do, and how to report – How to prevent, minimize, or relieve side effects – Importance of compliance/adherence to treatment schedule – Safe handling A Change in Therapy: Considerations for Stopping Ruxolitinib Therapy • Consider tapering the dose of ruxolitinib gradually rather than stopping abruptly. • After discontinuing ruxolitinib, MF symptoms generally return to pretreatment levels over a period of ~1 week. • Some patients have experienced: fever, respiratory distress, hypotension, DIC, or multi-organ failure • Evaluate and treat intercurrent illness and consider restarting or increasing the dose of ruxolitinib Jakafi prescribing information, 2014. Case Study (cont.): Michael G. • Michael’s MF is risk stratified as Int-2 risk (DIPSS; median survival, 1.5 years), as well classified as MPN-AP • At 60 years of age, induction chemotherapy followed by HSCT is a viable option (if a donor is available and his comorbidity index is appropriate ). • In the absence of a viable HSCT approach, enrollment in a clinical trial of a novel therapeutic approach should be considered. • He still appears to be benefitting from ruxolitinib with respect to spleen reduction and symptom management; he will continue while exploring clinical trial or HSCT options • Gradually taper off ruxolitinib immediately prior to induction chemotherapy or HSCT conditioning therapy Conclusions • This patient’s case illustrates a major unmet need – treatment of patients with MF-AP or MF-BP • Prognosis is poor, no medical therapy has been adequately evaluated in prospective study to demonstrate improved outcomes. • Selected MPN-BP patients who are transplant eligible (with an available donor) and have chemotherapy responsive disease, can have significant improvement in survival if HSCT is completed.1,2 • The effect of ruxolitinib prior to HSCT is being investigated.3,4 • Enrollment in clinical trial should always be considered when available 1. Kennedy JA, et al. Blood. 2013;121:2725-33; 2. Alchalby H, et al. Biol Blood Marrow Transplant. 2014;20:279-81; 3. Jaekel N, et al. Bone Marrow Transplant. 2014;49:179-84; 4. Stubig T, et al. Leukemia 2014;28:1736-64. Conclusions • Recently, treatment response criteria were proposed for use in clinical trials in patients with MPN-BP1 • While JAK inhibitors are effective in improving splenomegaly-related and cytokine-mediated symptoms, therapies that can alleviate cytopenias and decrease BM and PB blasts are needed 1. Mascarenhas J, et al. Leuk Res. 2012;36: 1500–4;