Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
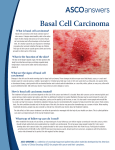
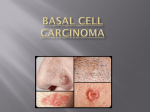
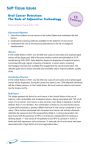
LESSON 5 SKIN AND SOFT TISSUE CONDITIONS Inflammatory conditions, Neoplasms, Others OBJECTIVES By the end of this lesson, you should be able to: 1. Describe rare infections of the skin 2. Classify neoplasms of the skin 3. Describe the main types of Benign growths of the skin 4. Describe the main vascular lesions of the skin 5. List premalignant lesions of the skin 6. Describe the major malignancies of the skin – BCC, SCC, MM 7. Describe cystic lesions of the skin 8. List other lesions of the skin Rare infections of the skin 1. Fourniers gangrene 2. Hydradenitis suppurativa 3. Lupus Vulgaris Fourniers Gangrene • Neclotising fasciitis (meleney’s streptococcal gangrene) • Causes destructive invasive infection of the skin, subcutaneous tissue and deep fascia with relative sparing of muscle • Caused by either polymicrobial involving anaerobes and facultative species such as coliforms or non gp A strep or monomicrobial due to beta haemolytic strep • Common site is groin, genitalia, lower abdomen • Treatment – Wide excision, antibiotics Hydradenitis suppurativa • Chronic suppurative process caused by apocrine gland hyperplasia • Common in 2nd and 3rd decades of life; F>M • Common site is axillae; also groin and perineum • Due to destruction from keratin plug leading to rupture into dermal and epidemal region and subsequent superinfection • Can present with severe pain • Treatment – metronidazole or erythromycin for long period can be curative • Surgical excision and skingrafting if conservative Lupus vulgaris • TB of the skin • Commonest in 10-25 yr of age • Common site – face, appear as brownish nodes (apple-jelly) followed by ulceration, slow • Blood expressed shows TB tubercles • Mucous membranes of mouth & nose may be affected • Treatment is anti TB or surgical excision if healing delays • Sq cell carcinoma can occur on lupus scars NEOPLASMS Neoplasms are abnormal growths of the skin They are classified into: 1. Benign growths 2. Premalignant growths 3. Malignant grwowths Benign Growths 1. 2. 3. 4. 5. 6. 7. 8. 9. Congenital Naevi (birth marks) Keratin Horns Saborrhoeic Keratosis Dermatofibroma Molluscum fibrosum Pilomatrixoma Sabeceous adenoma Cylidroma Rhinophyma Congenital naevi • Congenital (verrucous, epidermal) naevi are common entities which may single or multiple • They appear at birth or in early childhood • They are warty growth of brownish colour • A bit large horny excrescences may also occur • • • • • • • • • Keratin horn A papilloma with excess keratin formation Seen in old people Saborrhoeic keratosis Also called basal cell papilloma, seborrhoeic wart or senile wart Caused by overgrowth of epidermal keratinocytes Usually in large numbers and pigmented Occur on trunk, face and arms In middle life or elderly F=M, usually not seen as a disease and therefore not mentioned. Treatment is by curretage, diathermy or shave excision Dermatofibroma (fibroma) • Also called sclerosing angioma, histiocytoma, fibroma simplex, subepidermal nodular fibrosis • Occurs on the skin as a firm indolent, single or multiple nodules • May follow minor trauma or insect bites which initiate tissue reaction • Usually in extremities • In all age after puberty with M=F • Small, well defined nodule, touching the epidermis • Treatment is by Excision Molluscum fibrosum • Polypoid or filiform soft freshy skin tags that occurs on the neck, trunk or face • Associated with seborrhoeic warts • Frequently pendiculated, round, soft, elastic frequently pigmented lesions • Treatement is by excision or cautery Rhinophyma • “Potato nose” • This is a glandular form of acne rosascea • The skin of the nose becomes markedly thickened and sabeceous follicles opening are easily seen • Capillaries become dilated and the nose assumes a bluish-red colour • It can rarely be a basal cell carcinoma • Treatment is by surgery to improve the condition Vascular lesions • Structural and morphological anomalies due to faulty embryological morphogenesis • Present at birth, grows with the child and does not regress • Can lead to underlying soft tissue or bone hypertrophy • They are grouped into: 1. High-flow – arterial malformations, AV malformations 2. Low-flow – lymphatics, venous, capillary, combined 3. Ectasias – Telengenctasia ( spider naevi) Miscallaneus vascular lesions • Pyogenic granuloma – arise from minor trauma, acquired, vascular lesion of the skin and mucus membrane. Look like haemagiomas • Macular stains – salmon patch, present at birth over the fore head in the midline and over the occiput; disappear by age 1 yr Benign Pigmented lesions 1. Simple melanocytic tumour • Derived from neurocrest cells • Increased melanocytes from benign pigment naevi which include • Lentigo – in basal cell layer of epidermis • Junctional naevi – localized aggregations projecting into the dermal • Dermal naevi – entirely within the dermis • Compound naevi – features of both junctional and dermis naevi Café au lait spots • Light brown flat macules that are of often apparent at birth • Solitary lesion or increased numbers in syndromes such as neurofibromatosis and albrights syndrome Premalignant lesions • Actinic Keratosis • Bowen’s disease • Erthyroplastic of Querat ( Bowen’s disease of the grans penis) • Radiodermatitis • Chronic scars • Sabeceous epidermal naevus • Porokeratosi Actinic Keratosis • Also known as senile keratosis, solar keratosis • Formed by areas of epidermal dysplasia giving rise to cutanous scaling usually observed in sunexposed fair skin • Potentially malignant • Solitary lesion should be excised • Multiple lesions might clear with 5-fluorouracil Bowen’s disease • Intraepidermal squamous cell carcinoma that is potentially malignant and appears as a persistent, progressive flat red scaly or crusted plaque • Mostly found in the elderly • Triggered by solar radiation • Untreated, 3-5% will develop invasive squamous cell carcinoma • Treatment is by complete excision Erythroplasia of Querat • • • • • Bowen’s disease of the penis Occurs usually in uncircumcised males Radiodermatitis Due to excessive exposure to X-ray irradiations Presents with early erythema which progresses to desquamation and pigmentation • Eventually leads to squamous cell carcinoma Chronic scars • • • • • Carcinoma develops in a chronic scar Referred to as Majolin’s ulcer Grows slowly, relatively avascular Painless since the scar contains no nerves No secondary lymph nodes deposit until it spreads to normal tissue Sabeceus Epidermal naevus • Frequently affecting the scalp • Initially appears as a raised papular yellow areas developing into a papillomatous area as the child matures • 10% developes into basal cell carcinoma • Treatment is complete excision Porokeratosis • Characterized by annular plaques with horny borders • 13% may transform into basal cell carcinoma Malignant Lesions 1. 2. 3. 4. 5. Basal cell carcinoma Squamous cell carcinoma Virrucous carcinoma Kerato acanthoma Malignant melanoma Basal cell carcinoma (rodent’s ulcer) • • • • • Commonest kind of skin cancer Commonly affects ages 40-79yr >50% affects males 85% affects neck region Arises from pluripotent basal layer of dermis and hair follicles • Metastasis is rare • Presents as spots which do not heal • Has nodular appearance with rolled edges BCC cont… • Classified into: 1. Nodular – 50-54% 2. Superficial – 9-11% 3. Cystic - 4-8% 4. Pigmented – 6% 5. Morpheic – 2% Treatment of choice is by surgical excision (85-95% success) Other modes of treatment are Electrodessication and curretage(85-100% success, radiotherapy (92% success since BCC is very radiosensitive Squamous cell carcinoma (SCC) • Arises from areas with premalignant lesions or chronic irritation • More inflammatory and indurated than BCC • Squamous layer of the skin is involved in development of cancer • Related to radiation with UV light • Follows chronically ulcerated lesions and scars • Metastasis is mainly via lymphatic to regional nodes • Treatment of choice is surgical excision. • Radiotherapy can be used for large unresectable tumours Verrucous carcinoma • These are well differentiated SCC which invade locally but rarely metastasize • Commonly occurs in palms of the hands and the soles of the feet where they are referred to as carcinoma ciniculatum Malignant Melanoma • This a pigmented malignant tumour arising from epidermal melanocytes • Described by Hippocrates in 5th century BC • 1/3 to ½ develop in premalignant lesions or areas of chronic irritation • It has no sex predilection • Commonest site is the sole of the foot • May also occur in the eye, mucocutaneus junctions • Risk factors – albinism, tropical climate, life style, poor socioeconomic status, Xeroderma pigmentosa, Hutchinson’s freckles Malignant melanoma cont… 4 parameters of histological grading 1. Depth 2. Ulceration 3. Mitotic rate 4. Regression Malignant melanoma cont…. • Clinical features • Clinically presents in 5 types 1. Superficial spreading – commonest 64% 2. Nodular – most malignant – 12-25%, in young 3. Acral-lentiginous 4. Amelanotic – occurs in palms, sores and subungual regions – worst prognosis, may be pinkish or hypopigmente, may present with regional lymph nodes 5. Lentigo maligna – least common 7-15% Malignant melanoma cont… • Unknown before puberty • Development of malignancy in a mole should be suspected if the following signs occur: – Major signs – Change in size, shape or colour – Minor signs –inflammation, crusting or bleeding, sensory change eg itch, diameter >5mm • Spread is via: – Local spread – Lymphatics – by embolism or permeation – Haematogenous spread – to lung, liver, brain, skin, small intestines – secondary sites deposits are back in colour Malignant Melanoma cont…. Treatment • Treatment of choice is surgical – wide excision with a margin of normal tissue of 1-2cm – do not excise beyond the deep fascia • Regional node dissection of involved – diagnosis by FNAC recommended • Malignant Melanomas in children are very rare Other malignancies affecting the skin • • • • • • • Dermatofibroma protuberans Kaposis sarcoma Angiosarcoma Lymphagiosarcoma Primary cutaneous malignant lymphoma Merkes cell tumour Metastatic malignant tumours Other lesions of the skin • Cysts • • • • –Epidermoid cysts (sebaceous cyst) –Pilar cyst –Implantation dermoid cyst Callosity Corn Warts Venereal warts and moist warts Epidermal Cysts (sebaceous cysts) • Cysts containing keratin and its breakdown products surrounded by a wall of stratified sq keratinized epithelium • Have a punctum • Inherited in autosomal dominant fashion • Common sites – face, neck, shoulder and chest • Can be solitary but often are multiple • Suppuration may occur if superinfected • May form “sebaceous horn” if content slowly leaks • Treatment – Excision but when inflammed – I&D • May recur if not completely excised Pilar cysts • Multiple lumps in the scalp • Have no punctum • Histologically – similar to external root of the hair follicle Implantation Dermoids • From deep implantation of a fragment of dermis by penetrating injury • Traumatic inclusion cysts may appear on the palmar surface of the hand, buttock or knees Callosity • Localized thickened or hardened patches of hyperkeratinized skin. Acquired, superficial, circumscribed yellowish-white lesions • Occurs at pressure areas or friction areas of the hands, feet. Not painful. Require no treatment Corn • Horny induration of the curticle with a hard center caused by undue pressure. Chiefly found on the toes and feet. • Treatment is by surgical excision or application of abrasive chemical e.g. 50% podophyllin Wart • A viral induced tumour that undergoes spontaneous resolution. Contangious, usually in immunosuppressed patient • Tends to affect areas of trauma e.g beard, genitalia, hands, feet • Have no 100% cure – Curretage, diathermy, or 50% podophyllin can be used Venereal Warts and Moist wart • Referred to as papillomata accuminata • Warty papillomatous lesions occuring at most areas of the genitalia Conclusion Rare infections of the skin Neoplasms of the skin Benign Vascular lesions Premalignant Malignant – BCC, SCC, MM Cysts Other lesions 4/30/2017