Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Traveler's diarrhea wikipedia , lookup
Plant disease resistance wikipedia , lookup
Gastroenteritis wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Urinary tract infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Infection control wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
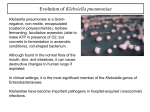
2011 International Conference on Food Engineering and Biotechnology IPCBEE vol.9 (2011) © (2011)IACSIT Press, Singapoore Challenge to healthcare: Multidrug resistance in Klebsiella pneumoniae Archana Singh Sikarwar1 and Harsh Vardhan Batra2 1 Faculty of Medicine and Health Science, International Medical University, Bukit Jalil,Kuala Lumpur, Malaysia 2 Scientist E, Defense Research Development and Establishment, Gwalior, India Abstract. Klebsiella pneumoniae has been associated with different types of infections and one of the important aspects of Klebsiella associated infection is the emergence of multi-drug resistant strains particularly those involved in nosocomial diseases. For our studies we have collected fifty – nine clinical isolates, from different places of India as this study was conducted in India. Morphologically resembled Klebsiella were recovered from respiratory, UTI and pus cases. Out of fifty- nine clinical isolates, twenty were found positive for K.pneumoniae at biochemical characterization. These clinical isolates of K.pneumoniae were further tested for antimicrobial sensitivity and most of them were found to be multidrug resistant. All confirmed K.pneumoniae isolates were resistant to carbenicillin and one among them recovered from sputum sample of a pneumonic patient was resistant to all the antimicrobial agents tested except exhibiting a partial susceptibility to amikacin. Klebsiella pneumoniae strains from clinical cases in our study were found highly susceptible to quinolones, aminoglycoside, amykacin and gentamycin. At the same time over 60% strains were resistant to chloramphenicol and tetracycline. We also found that 28 to 76% of them were resistant to cephalosporins (ceftizoxime and cefotaxime). Keywords: Klebsiella pneumoniae, Antimicrobial sensitivity, multidrug resistance 1. Introduction Klebsiella are ubiquitously present and reported worldwide. In recent years, Klebsiellae have become important pathogens in nosocomial infections [1]. The importance of Klebsiella species in the ever increasing number of gram negative aerobic bacillary nosocomial infections in the United States [2] and India [3] has been well documented. Epidemic and endemic nosocomial infections caused by Klebsiella species are leading causes of morbidity and mortality [4]. In addition to being the primary cause of respiratory tract infections like pneumonia, rhinoscleroma, ozaena, sinusitis and otitis, it also causes infections of the alimentary tract like enteritis, appendicitis and cholycystitis. They are frequently associated with the infections of urinary tract, genital tract, and the eyes. Statistical data and evidences from researches prove that multidrug resistance bacteria are emerging worldwide which is a big challenge to healthcare. Multidrug resistant bacteria cause serious nosocomial and community acquired infections that are hard to eradicate using available antibiotics. Moreover, extensive use of broad-spectrum antibiotics in hospitalized patients has led to both increased carriage of Klebsiella and the development of multidrug-resistant strains that produce extended–spectrum beta-lactamase (ESBL). Epidemic strains of cephalosporin resistant K.pneumoniae have been associated with increased morbidity and mortality in hospitalized patients [5]. Since 1983, nosocomial outbreaks of ESBL producing K.pneumoniae infections in Europe [6], the United States and South America have been described [7,8]. Between 1990 and 1992, 5% of K.pneumoniae clinical isolates produced ESBLs [9]. In France, 10 to 30 % of K.pneumoniae strains are reported to produce plasmid mediated ESBLs of the TEM or SHV families [7]. We have started our studies with following aims and objectives: • To analyze the severity of multidrug resistance of Klebsiella pneumoniae in India 130 • Challenges faced by healthcare community in India during treatment of multi drug resistant K.pneumonic patients.to overcome this problem. • To come up with some suggestions to overcome multidrug resistant problem. 2. Materials and Methods We have collected standard and clinical isolates of K.pneumoniae from different places of India and utilized them for their antibiotic resistant ability. 2.1. Bacterial strains: Standard culture of K.pneumoniae strain 3296 was collected from Yamaguchi University, Japan whereas total fifty nine clinical isolates were collected from different places of India. Out of all, fifty - four clinical isolates of Klebsiella species were recovered from pus, urine and sputum samples from Armed Force Medical College, Pune, India, four samples from pneumonic patients and one UTI sample from Patel Chest Hospital, New Delhi, India. 2.2. Biochemical characterization: All the clinical isolates were examined morphologically for colony characteristics on agar media. Those exhibiting mucoid colonies were processed for biochemical testing. Biochemical test employed were urease production, citrate utilization and fermentation of sugars. Sugar fermentation tests performed were sucrose, glucose, mannitol, lactose, adonitol, dulcitol, melibiose and esculin. Indole test and H2S production on TSI agar, oxidase, catalase and nitrate were also carried out. Besides these tests, motility and growth of organism in potassium cyanide were also checked. For biochemical tests standard procedures were used [10]. 2.3. Antibiotic sensitivity testing: Standard and positive clinical samples of K.pneumoniae were grown on nutrient agar. After 24 hours incubation at 37oC, fresh colonies of K.pneumoniae were grown in a tube containing 5mL of a tryptic-soy broth followed by overnight incubation at 37°C until it achieves the turbidity. Next day, dipped a sterile nontoxic swab into the broth and rotated the swab several times, pressing firmly on the inside wall of the tube above the fluid level to remove excess inoculum from the swab. Organism was inoculated over the dried surface of a Muller-Hinton agar plate by streaking the swab over the entire sterile agar surface three times, rotating the plate 60oC each time . We have placed the antibiotic discs evenly on the surface of the agar plate by using a sterile forceps then plates were placed in incubator at 37°C. After 24 hours of incubation, we examined each plate and reported the organism to be susceptible, moderately susceptible (intermediate), or resistant for antibiotics. 3. Results The standard and clinical isolates of Klebsiella were examined by battery of biochemical tests. Standard K.pneumoniae cultures showed positive reactions for urease production, citrate utilization, catalase reaction and fermentation of sugars like glucose, lactose, sucrose, mannitol, adonitol, melibiose and esculin. Organisms showed negative test for indole production. There was no H2S production on Triple Sugar Iron agar but growth of organism was seen in KCN. All fifty-nine clinical isolates exhibiting colonies similar to Klebsiella species were tested biochemically. Thirty-six clinical isolates showed typical common biochemical reaction pattern similar to the one seen with Klebsiella species, being positive to glucose, lactose, sucrose, mannitol and negative to oxidase and indole. When tested by second battery of biochemical reactions that included some rare sugars (adonitol, melibiose, esculin and dulcitol), twenty of them exhibited reactions attributable to majority of K.pneumoniae sub species pneumonia strain, being positive to adonitol, melibiose, esculin, urease and citrate. They also showed growth in KCN. The rest of the isolates had variable reactions with these tests. 131 Antibiotic sensitivity testing of twenty confirmed K.pneumoniae clinical isolates was done on Muller – Hinton agar plates. On the basis of resistance to antibiotic, strains were categorized in three groups. One group had strains which were susceptible (over 85%) to quinolones and aminoglycosides. The second group had strains which were moderately susceptible (intermediate) to antiribosomal antibiotics (chloramphenicol and tetracycline) with 62% resistant strains. The third group contained strains which were resistant to semisynthetic penicillins, ampicillin, carbenicillin (76-100%) and to co-trimoxazole (76%). Results are shown in fig 1. Fig 1: Antibiotic resistance pattern of Klebsiella pneumoniae isolates 4. Discussion In vitro data showed a wide range of beta-lactams, aminoglycosides, quinolones and other antibiotics are useful for treatment of klebsiellae infections [11, 12, and 13]. The clinical isolates of K.pneumoniae were tested for antimicrobial sensitivity and most of them were found to be multidrug resistant. All the Klebsiella pneumoniae isolates were resistant to carbenicillin and one among them recovered from sputum sample of a pneumonic patient was resistant to all the antimicrobial agents tested except exhibiting a partial susceptibility to amikacin. In such cases the disease is prone to progress to permanent debilitation or death of the patient if, isolation and identification of the causative agent and the subsequent antimicrobial susceptibility testing is not carried out at the early stage of the disease. In our studies, K.pneumoniae strains from clinical cases were found highly susceptible to quinolones and aminoglycoside, amikacin and gentamycin. At the same time over 60% strains were found resistant to chloramphenicol and tetracycline. Twenty-eight to 76% of them were resistant to cephalosporins (ceftizoxime and cefotaxime). Cephalosporins have been widely used as monotherapy and in combination with aminoglycosides for the treatment of Klebsiella infection. Plasmid encoded resistance to broad spectrum cephalosporins is becoming a widespread phenomenon in clinical medicine. These antibiotics are inactivated by an array of different extended spectrum beta lactamases (ESBLs) which have evolved by stepwise mutation of TEM/SHV type beta lactamases. Plasmid encoding these enzymes has been encountered in several members of the family enterobacteriaceae, but are, for unknown reasons, most often harboured by K.pneumoniae [14]. Epidemic and endemic nosocomial infections caused by ESBL producing K.pneumoniae represent a persistent problem in many parts of the world, especially in ICUs [15 and 16]. The emergence of multidrug resistant strains particularly those involved in nosocomial diseases and the alarming rise in resistance to SHV and ESBL producing groups of 132 antibiotics result in high morbidity and mortality. Early identification of agent, therefore, is important for timely management of patients. Klebsiella has been associated with different types of infections and one of the important aspects of Klebsiella associated infection is the emergence of multi-drug resistant strains particularly those involved in nosocomial diseases.The alarming rise in resistance to SHV and ESBL producing groups of antibiotics result in high morbidity and mortality.TEM- and SHV type ESBL producing Klebsiella pneumoniae were extensively reported worldwide after it was first identified in enterobacterial isolates from India [17]. The high prevalence of these drug resistant strains has further necessitated the requirement of a rapid and accurate identification system for K.pneumoniae. In our studies, we have found that out of fifty – nine clinical isolates, twenty clinical isolates were found positive for K.pneumoniae at biochemical characterization. When these clinical isolates of K.pneumoniae were further tested for antimicrobial sensitivity and most of them were found to be multidrug resisitant. The isolates were highly susceptible quinolones and the aminoglycosides. Over sixty percent strains were resistant to chloramphenicol and tetracycline but all the isolates were resistant to carbenicillin. 5. Conclusion Statistical data and evidences from researches prove that multi drug resistant bacteria are emerging worldwide which causes many public health problems and challenges to healthcare. Moreover, uses of broad spectrum antibiotics, insufficient aseptic condition and technique with inadequate control of infections spread had aggravated this problem. Recently, WHO warned society during press release and stated that antibiotics may lose their power to cure disease if action is not taken now against antimicrobial resistance problem [18]. WHO also recommended six ways to overcome multi drug resistant problem, those are: • Committing to a comprehensive, financed national plan with lines of accountability and community engagement; • Strengthening surveillance and laboratory capacity; • Ensuring a regular supply of good-quality medicines; • Regulating and promoting rational use of medicines and proper patient care; • Enhancing infection prevention and control in health settings; and • Fostering innovation, research and development 6. Acknowledgement I gratefully acknowledge the Director of the Defense Research and Development Establishment, Gwalior, India for encouragement and support. This work was funded by the ministry of Human Resources, Government of India, (Graduate Aptitude Test Examination) scholarship. I would also like to thank Dr J.Uchiyama (Yamaguchi University, Japan), Armed Force Medical College, Pune and Patel Chest Hospital, New Delhi for providing us standard and clinical bacterial isolates. 7. References [1] P.Nordamann, G.Cuzon and T. Naas. The real threat of Klebsiella pneumonia carbapenemase-producing bacteria. Lancet Infec Dis. 2009, 9 (4): 228-236 [2] J.R. Graybill, L. W. Marshall, P. Charache, C.K.Wallace and V.K.Melwin. Nosocomial pneumonia: A continuing major problem. Am.Rev.Respir.Dis. 1973, 108 :1130-1140. [3] N.B. Mathur, A. Khalib,R. Sarkar and R.K. Puri. Mortality in neonatal septicaemia with involvement of mother in management. Ind. J. Pediatri. 1991, 28 (ii) 1259-1264. [4] S.J. Cryz, R.Furer and R. Germanier. Protection against fatal klebsiella pneumonia burn wound sepsis by passive transfer of anticapsular polysaccharide. Infect. Immun.1985, 45 :139-142. [5] A.D. Dean, A.J. Dean, A.H. Burton and R.C.Dicker.Epi-Infoversion 5: a word processing database and statistics 133 programme for epidemiology on microcomputers.VSD. Inc Stone Mountain Ga 1990. [6] G. Arlet, M. Rouveau, I. Casin, P.J.M. Bouvet, P.H. Lagrange and A. Phillippon. Molecular epidemiology of Klebsiella pneumonia strainsthat produce SHV-4 B-lactamase and which were isolated in 14 french hospitals. J.Clin.Microbiol. 1994, 32: 2553-2558. [7] G.A.Jacoby and A.A.Medeinos. More extended spectrum B-lactamases. Antimicrob. Agents. Chemother.1991, 35: 1697-1704. [8] V. Jarlier, M.H. Nicolas, G Fournier and A. Philippon. Extended broad spectrum B-lactamases conferring transferable resistance to newer beta-lactame, agents in Enterobacteriaceae hospital prevalance and susceptibility patterns. Rev. Infect. Dis.1988, 10 : 867-878. [9] L. Verbist. Incidence of multiresistance in gram-negative bacterial isolates from intensive care unit in Belgium – a Surveillance study. J. Infect. Dis. Supp.1991, 70: 45-53. [10] R. Cruickshank . Medical Microbiology 1980, 12th eds. (revised reprint) Edinburg: Churchill Livingstone. 170 – 189. [11] S. A. Weisenberg , D. J. Morgan , R. Espinal-Witter and D. H. Larone .Clinical outcomes of patients with Klebsiella pneumonia carbapenemase-producing K.pneumoniae after treatment with imipenem or meropenem. Diagn Microbiol Infect Dis. 2009, 1, [Medline]. [12] Y. R. Chan, J. S. Liu , D. A. Pociask , M. Zheng , T. A. Mietzner , and T. Berger . Lipocalin 2 is required for pulmonary host defense against Klebsiella infection. J Immunol. , 2009, 15, 182 (8) 4947-56 . [13] J. M. Adams-Haduch , B. A. Potoski , H. E. Sidjabat , D. L. Paterson and Y. Doi . Activity to Temocillin against KPC-Producing Klebsiella pneumonia and Escherichia coli. Antimicrob Agents Chemother. 2009, 30, [Medline] [14] G.A. Jacoby. Genetics of extended spectrum beta-lactamases. Eur. J. Clin. Microbiol. Infect. Dis., 1994, 13: 2-11. [15] G. Arlet, M. J. Sanson-le-Pors, G. Rouveau, O. M. Fourinier,B. Schlemmer and A. Phillippon. Outbreak of nosocomial infections due to Klebsiella pneumoniae producing SHV-4-B-Lactamase. Eur. J. Clin. Microbiol. Infect. Dis. 1990, 9: 797-803. [16] K.S.Meyer, C. Vrban, J.A. Eagan, B.T. Berger and J.T. Rahal. Nosocomial outbreak of Klebsiella infection resistant to late-generation cephalosporins .Ann. Intern. Med., 1993, 119:153-358. [17] A. Karim, L.Poirel, S. Nagarajan and P. Nordmann. Plasmid- mediated extended-spectrum B- lactamase (CTX-M3 like) from India and gene association with insertion sequence ISEcp1. FEMS Microbiol. Lett. 2001, 201:237-241. [18] S.Young Soo, WHO, Western Pacific region, press release, 7 April 2011. 134