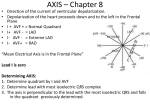
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
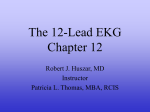
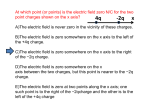
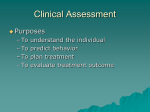
Cardiology / 12 Lead EKG 2016 Advanced EMS Refresher James A Temple BA, NRP, CCP Expected Outcomes • Review basic 12 Lead EKG interpretation • Using the basic understanding of 12 Lead EKG, dig a little deeper to pick up and predict cardiac events and prepare for them. • Review cases using some of the new concepts learned. • WHY? Is This Stuff Easy? • Dr Paul Hinchey (Austin-Travis County) • 12 Lead Over-read? – – – – 90 total STEMI alerts 87% appropriate to at least 1 cardiologist 43% unanimous “true” stemi 18% unanimous “False” positive STEMI alert EMS Expectations (Realistic) • How much training have you had? • How often do we read 12 Leads? • What are you really looking for? Sound like anything else EMS is dealing with currently? Why Do You Have to Be Good at This? • Decrease time to intervention – More lives saved • Why would we let EMS be the weak link in the chain? • We CAN make the difference here! – Pattern recognition – Predicting events – Preventing events 12 Lead Review • • • • • • • • • ST depression ST elevation Q Waves Axis Reciprocal changes T-Wave inversion / morphology R wave progression BBB Hemi-blocks Ischemia Injury Infarct ?????? ?????? Waveform Components: Q Wave First negative deflection before R wave; Q wave includes the negative downstroke & return to baseline Waveform Components: R Wave First positive deflection; R wave includes the downstroke returning to the baseline Waveform Components: S Wave Negative deflection following the R wave; S wave includes departure from & return to baseline Waveform Components: QRS • Q waves – Can occur normally in several leads • Normal Q waves called physiologic – Physiologic Q waves • < .04 sec (40ms) – Pathologic Q • >.04 sec (40 ms) See any Q’s? QTc A dialysis patient presented with dyspnea and a heart rate of 33. His medications included amlodipine and carvedilol. He has a history of hypertension and DM. His BP was 150/45 (bradycardia leads to long run-off time after each systolic beat, leading to low diastolic pressure). He appeared comfortable, in no distress. K = 7.5! Take Homes: 1. Bradycardia should always prompt consideration of hyperkalemia 2. Bradycardia may be the only ECG sign of hyperkalemia Waveform Components: QRS • Q wave – Measure width – Pathologic if greater than or equal to 0.04 seconds (1 small box) Q-waves in acute MI: • 1) QR-waves are common early in anterior MI. • 2) QS-waves are uncommon early in anterior MI; they are common in late presentation. • 3) Q-waves are independently associated with worse outcomes (78% relative increase in 90-day mortality in Armstrong et al.) • 4) Q-waves alone do not necessarily imply irreversibly infarcted myocardium; they should not dissuade from reperfusion therapy. Waveform Components: QS Complex Entire complex is negatively deflected; No R wave present Waveform Components: J-Point Junction between end of QRS and beginning of ST segment; Where QRS stops & makes a sudden sharp change of direction Waveform Components: ST Segment Segment between Jpoint and beginning of T wave Waveform Components: ST Segment • Need reference point – Compare to TP segment – DO NOT use PR segment as reference! ST TP T Wave • Should measure 5 mm in limb leads • Should measure 10mm in chest leads • Concordance • Should NOT be taller than “R”!! Hyperacute T-waves are a sign of a large amount of myocardium at risk and that it is still viable Coronary Arteries • Branch off of the aorta, just above the leaflets of the aortic valve • Three major arteries • Each supplies a specific area Right Coronary Artery • • • • Inferior wall of LV Right ventricle Posterior LV Posterior fascicle of LBB • SA and AV node Left Anterior Descending • • • • • Anterior wall of LV Septum Bundle Branches Hemifascicles Major pumping mass of LV Left Circumflex Artery • Upper lateral wall of LV (Leads I and aVL) • SA node in 45% • AV node in 10% • Posterior wall of LBB • Posterior hemifascicle Lead Groups I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Limb Leads Chest Leads Inferior Wall • II, III, aVF – View from Left Leg – inferior wall of left ventricle I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Inferior Wall • Posterior View – portion resting on diaphragm – ST elevation suspect inferior injury I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Inferior Wall Lateral Wall • I and aVL – View from Left Arm – lateral wall of left ventricle I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Lateral Wall • V5 and V6 – Left lateral chest – lateral wall of left ventricle I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Lateral Wall • I, aVL, V5, V6 – ST elevation suspect lateral wall injury Lateral Wall I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Anterior Wall • V3, V4 – Left anterior chest – electrode on anterior chest I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Anterior Wall • V3, V4 – ST segment elevation suspect anterior wall injury I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Septal Wall • V1, V2 – Along sternal borders – Look through right ventricle & see septal wall I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Septal • V1, V2 – septum is left ventricular tissue I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Evolution of AMI • Hyperacute – Early change suggestive of AMI – Tall & Peaked – May precede clinical symptoms – Only seen in leads looking at infarcting area – Not used as a diagnostic finding Evolution of AMI • Acute – ST segment elevation – Implies myocardial injury occurring – Elevated ST segment presumed acute rather than old Evolution of AMI • Acute – ST segment Elevated – Q wave at least 40 ms wide = pathologic – Q wave associated with some cellular necrosis Evolution of AMI • Age Undetermined – Wide (pathologic) Q wave – No ST segment elevation – Old or “age undetermined” MI STE…? What about the Big Fatties? A normal 12-lead ECG DOES NOT mean the patient is not having acute ischemia, injury or infarction!!! 12 Lead Concepts Lead Groups I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Limb Leads Chest Leads Location? ??? ??? ??? Axis Determination & Deviation • What is Axis? – “the general (mean vector) direction of electrical impulses as they travel through the heart” – “the sum total of all electrical currents generated by the ventricular myocardium during depolarization” – normally from upper right to lower left Axis Determination & Deviation • What do you need to determine the axis of an ECG? – The 12 Lead ECG – Leads CORRECTLY placed on the patient • • • • RA on the right arm LA on the left arm LL on the left leg Not on the chest or abdomen – Knowledge of axis deviation What Is Axis? • Overall direction of travel of electrical impulses as they move through the heart • Normal axis is downward and toward the left 22 Normal Axis • Upright complexes in Leads I, II, III • Forces going toward all three leads • Impulses going toward a positive, make a positive deflection Physiological Left Axis • Normal variant in adults • Common in obesity and athletes • Lead II can show upward or halfway deflection • Lead III is down Pathological Left Axis • Disease process • Suggests anterior hemiblock • Patients are 4 times more likely to arrest with a hemiblock and “chest pain” Right Axis Deviation • Rare occurrence in adults • Almost always pathological • Associated with posterior hemiblock • Lead I down and Lead III up Extreme Right Axis Deviation • Indeterminate axis • Usually ventricular in origin • Down in all three leads, I, II, III To Determine Axis • Run Leads I, II, and III • Leads must be on the limbs! • Look at the net QRS deflection in each lead (does it go up or down, or halfway) • Compare to the rapid axis and hemiblock chart Calculated Axis Angle • Machine calculates this for you • Use it with your chart • Look at the “QRS axis” or the “R axis” on some units • Follow the chart Rapid Axis and Hemiblock Chart Axis Quadrants Quadrants • Left axis -30 to -90 ° • Normal axis -30 to 90° • Right axis 90 to 180° • Extreme Right axis or “No Man’s Land -90 to 180° +120° aVR -150° No Man’s Land -90° -60° aVL -30° LAD +180° 0° I Normal RAD +30° +150° +120° III +90° aVF +60° II Axis Determination • Quick Axis Determination – Determine the net QRS deflection in Leads I and aVF (positive or negative) Normal axis LAD RAD ERAD Lead I aVF Axis Practice ERAD -90 - 180 RAD +90 - 180 I II III Axis HB? up up up norm up up down PhysL up down down Path L Ant LAD -30 - -90 Normal -30 - +90 down up down Right Post down down down ERAD Vent Axis Practice ERAD -90 - 180 RAD +90 - 180 I II III Axis HB? up up up norm up up down PhysL up down down Path L Ant LAD -30 - -90 Normal -30 - +90 down up down Right Post down down down ERAD Vent Axis Practice ERAD -90 - 180 RAD +90 - 180 I II III Axis HB? up up up norm up up down PhysL up down down Path L Ant LAD -30 - -90 Normal -30 - +90 down up down Right Post down down down ERAD Vent Axis Practice ERAD -90 - 180 RAD +90 - 180 I II III Axis HB? up up up norm up up down PhysL up down down Path L Ant LAD -30 - -90 Normal -30 - +90 down up down Right Post down down down ERAD Vent Axis Practice ERAD -90 - 180 RAD +90 - 180 I II III Axis HB? up up up norm up up down PhysL up down down Path L Ant LAD -30 - -90 Normal -30 - +90 down up down Right Post down down down ERAD Vent Imposters Checklist • • • • • LVH? BBB? Pericarditis? Early Repolarization? Paced Rhythms? Bundle Branch Blocks (BBB) • So What? • 25% greater mortality with BBB • When your QRS measures > 170 ms, your ejection fraction is below 50%! • Predictor of those at risk for developing a CHB. • New RBBB and STEMI = increased mortality • V1 and V2 – septal wall (BBB location) – makes sense anatomically CONTEXT • 2-4 % of patients with new LBBB have MI! • LVH can certainly lead to LBBB! • Makes it tough, not impossible, to detect MI with LBBB. Bundle Branch Block • Can be pre-existing condition • Can be caused by ACS • If AMI caused – 60-70% associated with pump failure – 40-60% mortality w/o reperfusion Bundle Branch Block Can Mimic or Hide Evidence Needed to Identify AMI • May Produce – – – – – ST elevation ST depression Tall T waves Inverted T waves Wide Q waves • May Hide – – – – – ST elevation ST depression Tall T waves Inverted T waves Wide Q waves Normal Ventricular Conduction • Normal Conduction – fibers of LBB begin conduction – impulse travels across interventricular septum from left to right • towards + electrode creates small r wave – travels across ventricles causing depolarization of both simultaneously • LV contributes most to complex – impulse travels away from + electrode creates primarily negative complex RBBB • RBBB in V1 – no change in initial impulse travel • small r wave – impulse depolarizes LV by itself since RBBB – RV depolarized by impulse thru muscle • it now contributes to complex – travels toward + electrode creating positive deflection R-S-R´ LBBB • LBBB in V1 – initial deflection altered since travels right to left now • Q wave or small q wave – RV depolarizes unopposed • may produce small r wave – travels across septum to depolarize LV • deep S wave LBBB • 5-13% of LBBB patients have MI • LBBB and tachycardia: – If tachycardia is present with LBBB, it is usually rate-dependent and resolves once rate is controlled. • Underlying rhythm must be supraventricluar! Turn signal Theory of BBB Example: LBBB Example: RBBB BBB? BBB? BBB? BBB? WTH? • What the heck is a fascicle? • LBB has 2 (ant / post) • RBB has one Hemiblocks • Posterior fascicle – Much more difficult to have block greater disease – Less common but more concerning – Supplies majority of inferior wall of LV – If blocked, results in right axis deviation Hemiblocks • Anterior fascicle – Easier to have block; More common – Supplies superior wall of LV – If blocked, results in pathologic left axis deviation Hemiblock Identification • Left Anterior Hemiblock – Pathologic Left Axis Deviation • small q wave in lead I • small r wave in lead III – Normal QRS or RBBB • Left Posterior Hemiblock – Right Axis Deviation • small r wave in lead I • small q wave in lead III – Normal QRS or RBBB • usually does have RBBB – “absence of right ventricular hypertrophy” Precursors to Complete Heart Block • • • • Any Type II AV Block Anyone with disease of both bundles Anyone with two or more of any blocks Examples: – – – – Prolonged P-R & anterior hemiblock RBBB & anterior hemiblock RBBB & posterior hemiblock Prolonged P-R with anterior hemiblock & RBBB Precursors to Complete Heart Block • If recognize precursors to CHB, then: – – – – Have high index of suspicion for CHB Have TCP ready (standby mode) Patient may need a pacemaker Administration of Lidocaine and other ventricular antidysrhythmics may result in CHB • Lidocaine contraindicated in patients with precursors to CHB unless TCP in place and ready Bifascicular Block • Anterior HB and RBBB Bifascicular Block • LBBB Bifascicular Block T Wave Morphology with BBB • Usual QRT waves, in the normal ECG, are positive in leads I, II and V3 through V6. – Concordance • In a LBBB, however, this isn’t true. Because of the changes in the vector or repolarization, T waves in a BBB should move in the opposite direction of the last deflection of the QRS. This is called “discordance.” To put this simply, if your QRS leaves you with a mountain, the T wave should be a valley, and vice versa. LVH and T wave deflection • Concordant positive T waves after a positive QRS are indicative of ischemia, and along with ST elevation is one highly specific sign of AMI in the presence of LBBB. • Depression in reciprocal leads would prove even more definitive. This is important because LBBB places patients at extremely high risk for cardiovascular complication. LVH • Step 1 – Look in V1 and V2 – Pick the deepest negative deflection (S wave) – Count small boxes of negative deflection in that lead – Remember that number • Step 2 – Look in V5 and V6 – Pick the tallest positive deflection (R wave) – Count small boxes of positive deflection – Remember that number • Step 3 – Add the two numbers together – Suspect LVH if the sum is > 35 (> 35 mm) LVH? Vs. MI? Benign Early Repolarization (BER) • Widespread ST elevation • NO PR segment depression • Tall, symmetrical and concordant T waves in the precordial leads. These findings are classic indicators of BER. BER Pericarditis PR Segment Depression Diffuse ST Elevation (Concave) Pt history and Exam Imposter Checklist • QRS <120 ms? – Not BBB, not VBR (Paced) • LVH criteria? • Early Repol? – Any reciprocal changes nix BER! • Pericarditis – Any reciprocal changes nix Pericarditis! Concordance • All V-leads up or down • All up: suggestive of VT but R/O WPW • All down: suggestive of VT, R/O LBBB Assembly Pifalls in WCT • • • • • Reliance on Lead II Reliance on the machine Vital signs/patient presentation Atrial fibrillation SVT is more common? Machine Logic Clinical Logic/Primary Survey • • • • • • Is the QRS >120 ms? Look at axis criteria (can be helpful) Look at the morphology in Leads V1 and V6 Look for concordance (all up or all down) Is AV dissociation present? Patient history/meds Clinical Logic/Primary Survey • • • • • • Is the QRS >120 ms? Look at axis criteria (can be helpful) Look at the morphology in Leads V1 and V6 Look for concordance (all up or all down) Is AV dissociation present? Patient history/meds First Criteria for VT • Extreme right axis • Upright complex in V1 (MCL-1) • 99% diagnostic for VT Example of VT Another Axis Criteria • Right axis deviation • Negative V1 (MCL-1) • 90% specific for VT Morphology Clues to VT • Lead V6 (MCL-6) • Predominately negative deflection in V6 indicates VT Example: RAD + Negative V1 Patient History • Two questions: – Have you had a heart attack before? – Did you have fast heart rates after your MI? • If yes to both, odds of VT are 86% with a wide complex tachycardia Lead V6 Criteria Capture or Fusion Beats • Arrow on the 6th complex indicates an escape beat or fusion beat • If seen it is diagnostic of VT (AV dissociation) Example • 23 y/o male presents with syncope. • Difficulty finding a baseline EKG…REALLY? Winter’s T Waves LAD Occlusion SWEET • A 32 yo type I diabetic woman presented with chest pain, nausea, vomiting and diffuse abdominal pain. She was in DKA with a glucose of 1128, and a K of 5.5. pH = 7.17, pCO2 = 24, HCO3 = 8. Sweet Sweet Sweet Resolution • 95% LAD occlusion Doc in the Box Doc-in-the-Box • 41 y/o male walked in to clinic for CP • Evaluated, sent home. T/P Considerations Size matters… • When T towers over R – BEWARE! • Hyperacute T waves Importance of Context CASE • A male in his 60's with med h/o only significant for HTN and hyperlipidemia presented for CP and SOB. On the day prior, he became very SOB and felt like he was going to pass out when he tried to stand up from bed. This was accompanied by chest heaviness and followed by left chest pain and a stiff sensation in his neck. The pain progressed but he went to bed but awoke in the AM with a heavy and "throbbing" chest. VS were: 122/92, pulse 82, RR 18, O2sat (room air) = 95% Here is his initial ED ECG: There are both precordial T-wave inversions AND Twave inversion in lead III. this is highly suggestive of pulmonary embolism. The better we are with 12 Lead EKG, the more positive impact we will have on the ultimate goal: Patient Survival Atypical • 41 y/o male • 3 days of chest discomfort, worsens with activity. • CP also associated with Dyspnea • Wife “requested” him to visit ED • EKG…. C/C: Dyspnea with assoc CP Case • 27 y/o male called 911 for palpitations and dyspnea. • No previous hx of cardiac issues. • Actions: • What won’t you do? 60 y/o 4 days of CP – some dyspnea CONTEXT is IMPORTANT • 40 y/o male with severe asthma attack • Narrowly avoided intubation • Routine EKG… Whadda ya think? AMS, Kussmauling, hyperglycemic… • The ECG is diagnostic of hyperkalemia, with QRS of 180 ms. The QRS improved immediately after giving 2 doses of Calcium gluconate. K returned at 7.3, with a pH of 6.91, HCO3 of less than 3. After a total of 5 doses of Ca gluconate, 6 doses of bicarb, 4 liters of fluid, and insulin, this patient with extremely severe diabetic ketoacidosis stabilized. You Make the Call… • A middle aged man was heard to be falling in his apartment. He was found very agitated, intermittently screaming (and on presentation was intermittently roaring like a lion). There was no apparent etiology. He required 10 mg of droperidol for sedation. He underwent an ECG as a routine part of the evaluation of possible ingestion: • Reference value: 440 ms • 593 ms is dangerously long and may result in torsade de pointes (polymorphic VT), and could be a result of the droperidol, or of metabolic and electrolyte abnormalities, or to many drugs or even be familial. • In any case, it is unsafe to leave it like this, so we gave 2 grams of Magnesium. A blood gas revealed a pH of 7.75 (entirely a respiratory alkalosis, drawn before intubation and due to his agitation and hyperventilation), which will also cause long QT and torsade. K was 3.2, which will also contribute. • By this time, we had him on the ventilator and so we intentionally slowed his ventilations to lower the pH. Hypokalemia – induced CA! Hypokalemia EKG’s • Promotes Torsades! • Makes sense that Mag Sulfate is indicated! • Hypocalcemia may also present with prolonged QT. Hmmmm… • 65 yo woman called 911 for pain in her upper back (between the shoulder blades) and in the left shoulder and left biceps, and some "mild chest pressure" elicited by the medics. Exam was normal. All but the back pain resolved with nitroglycerine 1730 hrs • ST depression in aVL is earliest indication of IWMI! • V2 ST depression here also suggests Posterior wall involvement! 1745 hrs 16 y/o female syncope while playing BBall • A female in her 60s presented with 3 days of nausea, vomiting, and diarrhea, and not feeling well. She complained of jaw pain and shortness of breath. There was a 30 second episode of syncope, and another one the previous evening, without any tonic clonic movements, tongue-biting, or incontinence. She was ill appearing. She had a remote history of lung cancer many years ago, cured. She had no other medical history. Whadda ya think? You Can Do This! • Hypotension • Shoulder pain • 3 days of symptoms • Inferior MI with RV involvement! Thank You! [email protected] 1820 hrs 1900 hrs 100% RCA Occlusion EKG post cath lab Poor Packer Fan… Missing anything? 90 minutes later… Are you sure? • There is 2-2.5 mm of ST elevation in inferior leads. • There is reciprocal ST depression in I and aVL, with T-wave inversion in aVL. • There is relative ST depression in V2 • There is ST depression from V3-V6. • There is a negative T-wave in V3, and biphasic T-waves in V4-V6. INFERIOR MI?? OOPS… • A 23 year old presented with pleuritic left chest pain radiating to the left arm. He had a recent sore throat. REALLY?? • This male in his 40's had been having intermittent chest pain for one week. He awoke from sleep with crushing central chest pain and called ems. • EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. He arrived in the ED and had this ECG recorded: • Active symptoms / pain Wellens Syndrome Chicken or the Egg? Pitfalls… EMS EKG before NTG