Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Journal of Clinical Laser Medicine & Surgery
Volume 11, Number 5, 199.3
Mary Ann Liebert, Inc., Publishers
pp.233-241
Second Generation Photodynamic Agents: A Review
By ETHAN D. STERNBERG. PH .D. and DAVID DOLPHIN, PH.D.
ABSTRACT
Over the last decade, laser treatment of neoplastic diseases bas become routine. The ability of these light~
induced therapies to effect positive results is increased with the utilization of photosensitizing dyes. The
approval of Pbotofrin® in Canada as a first generation photodynamic therapeutic agent for the treatment of
some forms of bladder cancer is being followed by the development of other agents with improved properties.
At this time a number of second generation photosensitizing dyes are under study in phase IIII clinical trials. A
review of the status of these trials along with mechanistic aspects is reviewed in this article. In addition, a
review of the status of lasers to be utilized for photodynamic therapy gives some indication of which instru·
ments could be considered for this therapy in the future.
INTRODUCTION
P
hotodynamic therapy (PDT) is a therapeutic modality that
utilizes a photosensitizer and visible light to create a roxic
environment to biological systems. PDT is utJIized in fields
ranging from cancer therapy to viral inactivation of solid tumors
and the treatment of leukemia (Fig. 1). The historical perspec~
tive of this methodology in the field of cancer is not within the
domain of this review but has been reviewed elsewhere.! We
will endeavor to enlighten the reader on the mechanistic aspects
of the phototoxic effect, show how these relate to different
therapeutic protocols, and review some aspects of recent clini~
cal trials for both the first and second generation compounds
being studied at II number of clinical sites throughout the world.
Photofrin® is the first generation compound for PDT and has
become most familiar to the readers of thi~ joumal. 2 It consists
of an oligomeric mixture of hematoporphyrin, a nonmetallaled
derivative of the porphyrin found in hemoglobin (Fig. 2). This
drug has undergone clinical trials throughout the world and hs!.
been found to be effective in treating a number of cancers. ~
Trials for the therapy have been instituted in a number of hospi~
tals throughout the world. Quadra Logic Technologies in partnership with Lederle Laboratories has recently filed a new drug
application (NOA) in a number of countries including Japan,
Belgium, and Denmark and will have filed in the rest of Europe
and the United States by the time of pUblication of this review.
A Notice of CompHance from the Canadian Health Protection
Branch was received in April J993 for Ihe lise of Photofrin® in
the treatmenf of superficial bladder cancer. This was a very
important landmark since it was the first approval for PDT
anywhere in the world.
Photofrin® is activated at 630 nm using an argon pumped dye
laser. This wavelength is chosen since the strong absorptions
due to oxy· and deoxyhemoglohin in the visible region become
weaker than (he longest wavelength absorption band of Photof4
rin®. As the absorption of the natural chromophores (principally the hemoglobins) decreases then the effective depth of
penetration increases with increasing wavelength (Fig. 3). In
addition to absorption, scattering of photons also limits the
effective penetration depth. In practice. light at 690 nm travels
twice as deep as that at 630 nm. On moving from 690 nm into
the near infrared (~OO "m) only an additional JO% effective
depth of penetration is achieved. Clearly then, second generation photosensitizers will be most effective when they absorb
and can be activated at wavelenglhs longer than that used to
activate Photofrin e (630 om). In addition. successful second
generation photosensitizers must exhibit Jess prolonged skin
photosensitivity than seen with Photofrin®. where a patient's
skin may remain photosensitive to strong sunlight for up to 4-6
weeks. s The side effects, small in comparison fo those seen
with chemotherapy or radiation therapy, could limit the use of
Photofrin® in non~life threatening indications.
Department of Chemisb'y, University of British Columbia, Vancouver, B.C., Canada and Quadra Logic Technologies Inc., Vancouver, British
Columbia, Canada.
233
Sternberg and Dolpbin
234
A
c
D
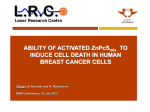
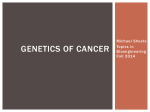
FIG. J. Feline T cells were treated with 2 ~gJml of BPDMA and .20 J/cm 2 of light. (A) Normal cells. (8) Initial damage on close
inspection shows small holes. (C) These holes increase in size after time. (D) Cell membranes arc complclcly nlptured. Reprinted
with permission from North cl a1. 49 Blood Cells 18: 129-[40.
THE PHOTODYNAMIC EFJ:1'"ECT
The processes hy which light creates a photoloxic effect in
the presence of a dye are still under debate . There are two
categories of energy transfer that may occur.t. The first step for
both of these is absorption of light by a dye. Typically the dye is
and
n=
an extended aromatic system such as rnerocyanine, methylene
hlue, or a variety of porphyrin derivatives (Fig. 4) . An excited
stale of the dye is generated that can interact with a biomolecule
via an ~Iectron transfer mechanism reSUlting in the destruction
of the hiomolecule and the bleaching of the dye (Fig. 5) . This is
known as a Type I photo process and the foonation of radicals
during such proce.c;ses may result in additional damage due
to ~ub,<;equent radical chain or oxidation reactions . A more
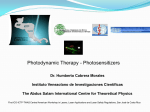
550nm 630nm 700nm
FIG. 3.
FIG. 2.
Photofrin® is a purified fraction of oligomers of he-
matoporphyrin.
800nm
0-7
Relative effective light dose versus wavelength (nm).
Light pencrratcs tissue better in region!>. near the inti·ared. Only
a moot!rate increase is found ill going from 700 to 800 nm.
Second Generation Photodynamic Agents
23S
~
CH,3SCH2CH2cHCR
~HR
102
FIG. 4. (top) Methyle~ blue; (middle) merocyanine; (/JOItom) tetraphenylporphyrin.
interesting process occu~ when the energetically exciled chromophore. after imersystem crossing from the singlet excited
state 10 the triplet slale, interacts with ground state triplet oxygen. This interaction results in the fonnation of singlet oxygen
e00 and the dye returns to it." original singlet ground state
ready to absorb another photon and to initiate another catalytic
cycle and the fOllTlation of more singlet oxygen. Although singlet oKygen has a short lifetime (approximately 6 ~sec in water
and a little longer in cell membranes), it has the ability to
readily react with a wide variety of biomolecules as shown in
Fig. 6. The~ latter reactions can cause the destruction of vari.~
ous biological components and shut down numerous biological
processes. Singlet oxygen is generated catalytically and the rltle
of singlet oxygen generation depends on some of the crileria
described below. In the case of several phototoxins the quantum
yield for singlet oxygen production is around 0.7. 7 Three
criteria determine the efficacy of a sensitizing dye, in 11 non-
+
hv
, -¢:
Sensitizer
9
I
e
~
2
10
2
biological system. The molecular extinction coefficient (E.)
measures the ability of a sensitizer to absorb light falling on it at
a specific wavelength effectively. The quantum yield of bleach~
ing of the pholo~ensitizer detemlines its lifetime when undergo~
ing a Type I photo process, and the quantum yield for singlet
oxygen production measures the ratio for the number of photons
absorbed to the number of singlet oxygen molecules produced.
These three criteria are relatively easy values to measure, how~
ever. relating these parameters to in vitro and especially in vivo
cyloloxicity is difficult.
The environment of a phototoxin not only determines which
biological systems nre most disrupted by PDT but also determines the efficiency of the sensitizer, becau~ of photobleach~
iog and the photo properties of the tissue. This synergism complicates the biologjcal studies in that it is possible that the site of
the greatest concentration of the dye may not define the site of
cell death. Thus the development of dyes for PDT differs from
the classical development of pharmaceutical compounds where
one hopes to find a drug that interacts with a specific binding
site and then further modify the drug to interact more effectively
with that binding site. 8
+ e
•e
Sensitizer
e
FIG. 6. Biomolecules such as cholesterol (A). methionine
(8), guanidine (C), and histidine (D) give a number of products
ranging from hydropcroxides to sulfoxides.
.61
Sensitizer
.3 Sens itizer·
30
•
Type I
Type II
FIG. S. Two types of reactions can occur from the photoex.cited state of a sensitizer 5 . They may react directly with a
substrate via electron transfer Hnd bleach (Type 1). or undergo
intersystem crossing, react with oxygen, and generate singlet
oxygen.
PHOTOTOXJNS IN BIOLOGY
Many photodynamic agents have been investigated for their
abilities to induce a phototox.ic effect. Compounds that are near
or currently in clinical trials range from a totally synthetic
tetrahydroxytetraphcnylchlorin (1) developed by Bonnell and
Bercnbawn9 (tnd zinc phalocyanine (3) being used by ClBA~
GcigyJO to the modified n~tural product monoaspartylchlorin eo
(4) being investigated by Nippon Petrochemical, II tin etiopurpunn (2) synthesized by Morgan et aI., 12 and benzoporphyrin
derivative monoacid (BPOMA) (5), which we at QLT and
Sternberg and Dolphin
236
CI
HO~"'''
"
CO:;!CH.:s
"~
01<
1
3
"' 'iHH
H H
01<
!:02h
CO',zH
FIG. 7.
4
700
Various photosensitizers in, or approaching clinical
FIG. 8. Four analogues of sulfonated phthalocyanines are
strucLurdlly similar but have significant differences in phototoxicity. (A) X = (H.H,H,SO,H); (B) X = (H,H,SOJH,SO)H);
(C) X = (H,SO,\H,S03H,SO.,H); (D) X = (SO)H,SO.,H,
trials.
SO]H,SOlH).
Ledene Laborutories are developing l3 (Fig. 7). All of these
compounds have absorption maxima beyond 650 nm and ex.~
tinction coefficient at their maximal long wavelength abso~
tion at least IO-foJd over that of Photofrin® at 630 om. Figure 7
illustrates the near red absorption maxima of several of these
newer photosensitizers.
Two sites of destrucLion are generally acknowledged to be
important to the in vitro damage 10 cells. TIle cell membrane is
susceptible to a number of as~ults by singlet oxygen. 14 Proteins within the membrane, on PDT treatment. may be modified
and have their ability to channel ions disrupted. Although lipid
peroxidation can occur routinely on PDT the changes in membrane permeability in models such as red hlood cells seem to be
associated with damage to proteins . l~ Memhranes within the
cell such as those associated with the Iysosomes have also been
suggested as sites of cell destruction. A further site of destruction is associated with mitochondria . 16 Isolated mitochondria
have sbown that photosensitization by Photofrin® created a loss
of oxidative phosphorylation that could be traced to oxidation
of thiols, in carrier proteins, by singlet oxygen. 17 The modit1cation of other enzymatic processes has also been observed in
vitro. For instance, aldehyde-3-phosphate dehydrogenase has
been shown to lose the integrity of the SH sites in the active
center after PDT. 18 Changes in activity. conformation, and
fluores(''ence along with an increase toward protease susceptability are some examples of such destmction in this cxtensi vely studied enzyme. Magnetic resonance imaging (MRI) has
shown a dramatic drop in ATP levels immediately after PDT,I?
probably as a result of cell repair mechanisms being activated .
Even nuclear enzymes are affected by PDT. 20 In the calSC of
DNA repair, photodynamic treatment of L929 cells generates
nuclease activity that is nonnally controlled by ADP-ribosylation. The effect of direct single-strand damage to DNA has been
noted with select photosensitizers in some systems. Recent
studies suggest a dominant fonn of destruction associated with
the DNA may correspond to interruption of microtubulin formation by a low-density lipoprotein delivered photosensiLizer
such as with Pholofrin®. 21
The site at which tumor damage occurs is related not only to
where the sensiti7.er causes damage in the cell but also to the
morphology of the tumor. (t has heen observed depending on
the hydrophilicity of the photosensiti7..er, that a higher concentration can be found around the tumor as compared 10 that of
surrounding tissue. 22 This increase in concentration may ~
accounted for by either specific upwkc by a lipoprotein-associated mechanism as ~een with other drugs or by simple physical
morphology of leaky Lumor vasculature and poor lymphatic
drainage. Richter et al. have shown that low-density lipoprotein
(LDL) bound BPDMA reduces the amount of drug in the skin
while destruction of the tumor remains the same. 2 .l II is known
that LDL binding sites are higher on cancer cells and it is a topic
of intense interest in the field or drug delivery. 24 Formulation of
a drug may 00 important in optimizing (his increalie in drug
localization perhaps by an LDL delivery system. In the case of
BPDMA, the fonnulation that is utilized for clinical trials are
unilamellar vesicles (Iiposomes) to help solubilize the hydrophobic drug and direct it to its lipoprotein-dominated delivery
mechanism . 2~ Lipo~ome..~ are alw being investigated for use in
the delivery of zinc phthalocyan;ne,2(, a compound that normally ha~ extremely poor 501ubility even in organic solvents.
The water-soluble NEP6 also accumulates in tumors although it
is readily taken up in the blood by ~erum albumin. 27 Perhap~
even in th is case, initi al delivery of the drug is dominated by the
lipoprotein fraction of Mood even though a majority of il hinds
to the serum albumin.
It may nor only be the actuat destruction of cancer cells that
results in tumor ablation during PDT but also that of the micro(neo)vasculature. 28 Some control over the biological behavior
of the photosensitizer associated with its structure has been
observed. A series of modified aluminum phthalocyanines
(Fig. 8) in which the parent molecule has sulfonation ratios
ranging from 1 to 4 has shown that the more lipophilic monosulfonated compounds are marginally more effective than the tetrasulfonatcd compound in terms of absolute phototoxicity in
vivo .29 However, in vitro experiments show that the very hy~
drophilic telrasulfonated material has poor photosensitizing
abilities. Some property of the ;,~ vivo delivery system to the
vasculature has increased the more hydrophobic compound's
efficacy. Such possible vasculature destmction has been dem*
onstrated by a numbcrofrcsearchers . Morgan et aJ. have shown
that rddioactive microsphcres are held up to a greater extent in
tumors after PDT. JO MRI has been used to show that the relax*
ation coefficients (T r T 2) of water around the tumor RfC dntmatically changed soon after PDT.3' A new technique thaI utilizes
laser doppler mt!asurements can generate information much like
that given by MRI about blood flow of a recently treated tu-
mor.32
237
Second Generation Photodynamic Agents
Perhaps the most interesting :1!>pect of PDT is associaLed with
(he immunological effects of posttreatment. Most of the significant studies in this field have been carried out with HpD. a
slightly less pure [Offil of Photofrin®, which was initially developed in the 1950s by Cohen and Schwartz as a radio protectorl
sensilizer. 3J In the dark HpD has been observed by Canti et al.
to cause increase in bone marrow and spleen hypercellularity in
mice. 34 This compound has been used to rescue mice from
nu.liation therapy for leukemia. Photodynamic therapy in mice
in contrast has shown immunosuppression as indicated by sensitivity 10 dinitronuorobenzene. :l.~ Observation of patients after
!>uccessful treatment for bladder cancer showed an increase in
chronic inflammatory cells. J6 Further observations have shown
a relationship between the cytokine~, interleukin-l~, interleukin-2, and tumor necrosis factor-lX concentrations and the level
of PDT trealrnent 1n patients. More direct evidence of cytokine
release was found hy Evans el al. who observed "tumor necrosis
factor" release by macrophages after PDT.37 Bellnier has
used combination therapy of PDT and tumor necrosis factor to
increase tumor response ..1R Thromboxane has also been found
10 be released shortly after PDT. V) It is also suspected that nitric
oxide, better known as endothelium releasing factor (EDRF),
which is related to guanylate cyclase, may be a consequence of
macroph age ac (i vation. 40 Th is is not surpris i ng in that at least in
the case of Photofrin®, a minor constituent of the drug is protoporphyrin IX, a cofactor in the cascade in nitric oxide formation.
LIGHT DELIVERY DEVICES
In the Ia.'>t several years QLT and Lederle have set up total
laser systems that meet international clinical standards. Among
the areas to review were the safety. equivalency of clinical
lasers to a reference standard, compatibility of existing fiber
optics and power meters, verification of manufacturers specifications, conformance with international regulatory require~
lnents, and suitability for the clinical setting. This i:s an ongoing
process.
For PDT many types of lasers have been evaluated. The mosl
common type in use is the argon pumped dye laser (APDL).
This has been used exclusively in the QLT/Lcdcrlc Photofrin~
Phase III clinica.l trials in North America. Recently, APDLs
such as the Lambda Plus from Coherent Medical have been
engineered specifically for PDT with Photofrin® as the toxin. Il
produces upward of 1.9 W from the tip of the fiber at 630 nm,
which is more than enough power [or most clinical requirements. Other lasers that have been considered for use with
Photofrin® are (he copper vapor pumped dye lasers and the gold
vapor lasers. These pulse systems suffer from several problems
such as lack of technical compatibility for the clinical setting,
developing light dosage standards to relate to the APDLs. and
high peak pulse energy output lhat lend~ to degrade the optical
fibers.
The utilization of a KTP Y AG to pump a dye in the region of
630 nm has been achieved and an ex.ample of such a system has
been made by Laserscope. At the primary output of 1066 nm
this laser can be utilized for general Y AG surgical applications.
When the output in frequency doubled to 532!lm it can pump a
dye laser 10 a number of standard frequencies. This laser provides a high frequency pulse of -- J0 kHz with a relatively low
flower output of I kW, which should prove to maintain fiber
integrity. The last ~everal years have seen the development of {l
new type of laser that has the potential to be comp8ct, require
little or no cooling, and should work directly from a wall plug.
These solid state diode lasers have shown that clinically significant output (-- 3 W) can be achieved at 630 nm and thus may be
considered in the future for use with Photofrin®. 41
For second generation compounds the diode laser. KTP Y AG
pumped dye lasers. and the standard APD laser are being reviewed. Clinical trials at present are concentrating on utilizing
research type APDL. However, as the second generdtion drugs
move through clinical trials it becomes mon: likely that a diode
laser designed for the drug's specific wavelength will be developed.
In the case of psoriasis or cutaneous cancers it may be practical to u~e nonlascr light sources such liS arc lamps. fluorescent
tubes, and light emitting diodes since the light does not have to
be concentrated into a small a!C<t. These light sources will
require all the clinical equivalency t.1udies, which have been
nccessary for the lasers.
At present PDT requires the utilization of a laser couploo to a
fiber optic system incorporated info an endoscope. Fiber optic
systems have been developed with specific treatments in mind.
In the instance of cutaneous cancer il GRIN lens is utiliz,ed to
spread the light to a cone. Thi.s allows light dosages to be easily
calculated by taking into account the transmitted power from
the tip, the time, and the distance from the tip to the treatment
field. Bladder cancer requires the incorporation of a sphere
diffuser into the above system. Newer systems have utilize.d a
balloon catheter to center the fiber as the balloon expands the
bladder to be roughly spherical. This, in combination with an
intrabladder detector, should ensure constant and even light
dosimetry. 42 Cylindrical geometries that are found in the esophetgus or the bronchi can be treated by fibers developed with
cylindrical output. A fiber with a cylindrical output tip of up to
2.5 cm in length i!. passed into the treatment area and placed
parallel to the tumor. Improvements to !hi~ system include the
development of a balloon catheter with detector probes on the
wall. In combination with this a face of the balloon has been
darkened generating a lantern effect. In the case of a very large
tumor the fiber can be placed directly into it. 43
CLINICAL TRIALS
The details and complexity of preclillical studies and clinical
trials are even more complicated for PDT than for a "traditional" drug since both drug and light are involved. Toxicity
must examine the traditional "dark" effects as well as those
generated on illumination. For the most part none of the drugs
described above ha<; been repolted to have any Inherent dark
toxicity in doses ranging much higher (X 10-X 1(0) than the
therapeutic dose. After stability and toxicity of the appropriate
drug fonnulation are addressed, il is necessary in a Phase I
clinical trial to investigate drug dosage, time of irradiation after
injection, pharmacokinetics, human drug toxicity, and, most
importantly, the extent of skin photosensitivity during and after
238
treatment. The development of most standard therapeutic
agents generally does not have 10 correlate drug dosage to skin
toxicity and light activation of drug. For these reasons initial
clinical trials in PDT have been directed toward investigating
the use of the drug for treatment of skin cancers. In these studies
a comhined review of toxicity toward the skin while deriving
information about the light doses necessary to damage the tumor can be detennined. Of course such infonnation gives an
indication of the efficacy toward the IUmor, which is not generally the goal of initial clinical trials.
A profile of drugs in Phase I investigations 10 date has shown
that after initial injection the drug takes some hours to accumulate in the tumor and the skin. One hopes to irra<.liate at some
time after the injection so that therapy can proceed on the same
day. Time of accumulation into the tumor as compared to the
skin or other tissue may not be ideal for all the new drugs. In the
case of Photofrin® a dosage of approximately 2.5 mg/kg i~
st(tndard .44 Irradiation occurs some 4H to 72 hr after injection at
a time when the drug has a higher concentration in tumor
compared to that in surrounding tissue. A typical light dosage
from the APDL is 150-250 J/cm 2 for treatment of a lung tumor.
In the case of bladder cancer the light is diffused over the entire
surface of the organ to give a light dosage of 150 J/cm 2 •4~ With
the above dosage of drug, skin photosensitivity may last about
4~ weeks. Most photosensitizers are also good fluorophores.
This property may allow the clinician to eventually determine
the level of drug in both the skin and tumor before and after
irradiation, which could be useful both for delennining the site
of treatment and for calculating the appropriate light dosage
during therapy.
Four second generation drugs are currently in Phase Tclinical
trials. These are BPDMA, with which the authors are most
familiar, monoaspactylchlorin e 6 • mesQ-tetra(m-hydroxyphenyl)chlorin (mTHPC), and tin eliopurpurin. Since much of the
preclinical and clinical research is of a proprietory nalure, information on the progress of Ihese drugs toward a submission of a
new drug application (NDA) is rather limited. None exists, as
of yel, for the tin etiopurpurin.
There is a pllblished Hccounl on the treatment of 4 patients
using mTHPC and it is known that additional patients have been
enrolled in the study. 46 mTHPC is somewhat hydrophilic and
rapi<.lly accumulates in malignant mesothelioma. The drug is
delivered in a mixture of polyethylene glycol, ethanol, and
water and is formulated just prior to injection. The ratio of drug
in tumor as compared to surrounding muscle was determined to
be 7: 1 and 14: 1 relative to skin. These ratios are higher than the
2-4: 1 found for Photofrin® in human..I\. The circulating concentration of the drug 48 hr after injection was found to be 0.15
mg/ml. while the half-life of the drug in circulation was approximately 12 hr. Dosages ranged from 0.075 to 0.3 mg/kg with a
light irradiation of 10 J/cm 2 at 650 nrn. At the lower dosage
50% necrosis of the lumor was shown while the next higher
dosage showed 80% necrosi~ and the final dosage 100% necrosis to a depth of 1 em. Derailed histological profiles of the tumor
and surrounding tissues described the extent and area of lissue
damage. Description of skin photosensitivity studies was sparce
and the studies appeared not to be carried out under controlled
conditions with a solar simulator. However, some anecdotaJ
data were noted. Skin photosensitivity appeared to begin some
time after injection (3-10 days); it does appear, however, thai
Sternberg Bnd Dolphin
significant clinical photosensitivity has been observed in some
patients up to 10 days after treatment, which may place limitations on the use of this drug in PDT.
Phase I clinical trials for the water~soluble monoClspartylchlorin C6 began at the same time as for BPDMA and were
examincd against the same skin tumors described below. 47
Drug doses were assigned in the range 0.5 to 2 mg/kg with
concurrent increases of tight dosage from 12.5 to 200 J/cm 2 . As
in the ca~e of BPD <.Irug dosages were limited to (he lower
concentrations because of the initial positive responses found.
Skin sensitivity in the lowl.!r dosages used (0 .5 mglkg) lasted up
to 7 days. This drug has strong binding to serum albumin~ and
it appears to circulate for a much longer lime than other PDT
drugs; in fact the drug is readily detectahle 4 weeh after treatme-nt while 80% of the initial concentration is detected in the
blood 10 days after injection.
The second generation photosensitizer BPDMA is a semisynthetic porphyrin derivative that has been found to be effective in
treating a number of cancers in vivo along with purging of
viruses from blood:19 In the ongoing clinical trial information
about the pharmacokinetics, skin photosensitivity along with
tumor response has been reported. 50 The patients had a range of
cancers Ihat included basal cell carcinoma, metastatic breast
carcinoma, metastatic gRstrointestinal carcinoma, and metastatic amelanotic melanoma. Drug dosages ranged from 0.25 to
0.5 mg/mg in the patients who were infused 3 hr prior to
irradiation while light dosages administered by a laser tuned to
690 nm ranged from 50 to 150 J/cm 2 for the low drug dosages to
50 J/cm 2 for the high drug dosage. Sixty-four cutanoous tumors
were treated and followed for several months after treatment.
Overal1 tumor response was 63%, while 100% response.~ were
noled for the higher drug and light dosages . ~J
Since the major purpose of the first generation trial was to
judge skin photosensitivity the most extensive studies for UV N
VIS light were carried out with the utilization of a filtered xenon
arc lamp source onto normal skin soon after light treatment of
the tumors while UVB light was generated from fluorescent sun
lamps. Testing of UVB sensitivity showed no response for the
carly patients, so these assays were discontinued. Marked skin
photosensitivity to UV A/VIS light was noted early after treatment. On the day of treatment the challenged light dose was
reduced for the higher drug dosages so that minimal erythema
dose (MED) could be noted. Close examination of light exposure onto the patients ranging up to 9 days after treatment for
high drug dosages shows u logarithmic loss of photosensitivity.
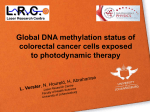
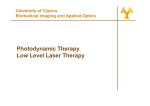
An overall phannacokinetic profile of drug serum concentration
is reviewed in Fig. 9. It is noted that the drop of all drug dosage
levels down from the maximum concentration corresponded to
-I hr. The relationship between these results and the corre~
sponding clearance of drug from sk.1n has yet to be investigated.
All the drugs investigated to date have exhibited distinct
clinical responses. The maximum effective drug do~e corresponding to minimum skin sensitivity has yet to be determined
for any of these materials. However, general approaches toward
optimizing such a differential can be applied to all of them.
Wilson 5 and others have suggested that a minimum drug dose
that would then be treated with a large light dose would illicit
the best response over all clinical responses, especially if moderate bJeaching of the drug occurs. Several other approaches
may be considered when optimizing light dosage for clinical
239
Second Generation Photodynamic Agents
-:J' ',000
~
Q>
5
500
200
""§
100
~
u
~
20
~~
~e:
0..
o
8.
~O
9.
10
5+----r--~----T---~--~
o
6
12
18
24
30
TIME (h)
10.
FIG. 9. Post injection plasma concentration versus time profiles of BPDMA in blood with a doseage of 0.25 mglkg in
humans.
11.
respunses, which could include fractionation of the light
dosage.
12.
13.
ACKNOWLEDGMENTS
We wish to thank our colleagues at Quadra Logic Te<:hnologies and Lederle Laboratories for their assi~tan{;e in preparing
this manuscript, especially Michael Stonefield and Ron Caroll
for their comments on light delivery devices.
14 .
15.
REFERENCES
I. Dougherty, T. S., Henderson, B. W., Schwartz. S ..
Winkelman, J.W., and Lipson, R.L. (1992). Historical
perspective, in: Photodynamic Therapy: BaJic Princi·
pIes (md Clinical Appliwt;on.~. B. W. Henderson and
16.
T.J. Dougherty (eds.) New York: Marcel Dekker. pp .
1033-1050.
Coulter, A. (1990). The slatus of photodynamic therapy
research: An overview of current and future cancer clinical treatments . J. Clin. Laser Med . Surg. 8,2- 11.
Marcus. S.L. (1992). Photodynamic therapy of human
cancer. Proc. IEEE 80.869-889.
Kessel, D ., Byrne, CJ., and Ward, AJ. Pho{Qscnsitizing dyes related to hematoporphyrin derivative: StnlCture activity relationships. in: Plwrodyllomic: Therapy:
Basic Principles and Clinical Applicatiolls. B. W. Henderson and T.J. Dougherty (eds). New York: Marcel Dekker, pp. 124-143.
Starr, W.M .• Wilson, B.C., and Patterson, M.S.
(1992). Light delivery and 0plical dosimetry in photodynamic therapy, in: Photodynamic Therapy: Basic Principles ami Clinical Applications. B.W . Henderson and
T.J. Dougherty (eds). New York: Marcel Dekker. pp.
335-369.
Turro, N.J. (1965). Molecular PhOlochemi.'ilry. New
York: W.A. Benjamin.
Sternberg, E., Dolphin. D., Scurlock, R.O., Rougee,
M. , and Ben sasson , R. V. (1992). Photophysical proper-
17.
2.
3.
4.
5.
6.
7.
18.
19.
20.
21.
ties of benzoporphydn derivatives, second generation
candidates for photodynamic therapy. J. Photochem.
Photobiol., submitted .
Portoghese, P.S. (1992). Th.e role of concepts in structure activity relationship srudies of opioid ligands. J.
Mcd. Chern. 35. 1927-1938.
Bonnetl, R .. and Bercnbaum, M. (1991). Dihydroporphyrins and methods of treating tumors, U.S. Patent
Number 4.992.257.
Rosenthal, I. (1991). Phthalocyanines a~ photodynamic
sensitizers. Photochem. Photobiol. 53,859-870.
Aizaw8, K .• Okunaka, T., Ohcanij. T., Kawabe, H.,
Yasunaki, Y .• Ohtomo, N., Nil.himiya, K., Konaka,
c., Kalo, A., Hayata, Y., and Sailo, T. (1987). Localization of mono-L-aspartylchlorin (NePe(,) in mouse tissues. Photochem. Photohiol. 49, 789-793.
Morgan, A.R., Garno, G.M., Keck, R.W., Erikson,
L.D., and Selman, S.H. (1990). Metallopurpurins and
light Effect on transplantable rat bladder tumors and
murine skin. Photochem . Photobiol. 51, 5~9-592.
Richrer, A.M., Waterfield, E., Jain, A.K., Sternberg,
E.D .• D<llphin, D., and Levy, J. (1990) . III vitro evaluation of four structurally related benzoporphyrin derivati ves . Photochem. Photobiol. 51 • 495-500.
Schathurst, A .A., Van Stevenick, J., Went, L.N., and
Suurmonl, D. (1972). Pholod ynami C damage of erythrocyte membranes caused by protoporphyrin in protoporphyria and in normal red blood cells. Clio. Chim . Acta
161-170.
Ben·Hur, E., Orenstein, A . • Livinc, A., and Rosenthal,
J. (1990). Photosensitized ox idation of human red blood
cells: Cation effects on volume changes and relevance to
blood vessel occlusion . Lasser Life Sci. 3,255-262.
Satet, C .• and Moreno, G. (1990). New trends in photobiology photosensitizers of mitochondria: Molecular and
cellular aspects . J. Photochem . Photobiol. B. BioI. 5.
133-150.
Davies. KJ.A., Lin, S.W., and Pacitici, R.E. (1987).
Protein damage and degradation by oxygen radicals IV:
Degradation of denatured proteins . J. BioI. Chern. 262,
9914-9920.
Prinszc, C., Dubbelman. T.M .A.R., and Stevcninck. J.
Van (1990). Protcin damage induced by small amounts
of singlet oxygen or hydroxyl radicals. Biochim. Biophysic. Ada 1038, l52-157.
Hilf. R .. Gibson, S.L. Penny, D.R .• Ceikler, T.L.. and
Bryant. R.G. (1987). Early biochemical responses to
PDT monitored by NMR spectroscopy. 1. Photochem.
PhOlobiol. 46, 819-823.
Dunnelman. T.M.A.B., Prinsze, C., Penning, L.C.,
and van Slevenick, J. (1992) . Photodynamic therapy:
Membrane and enzyme photobiology. in: Photodynamic
Therapy: Basic: Prin.ciples and Clinical Applications.
R.W. Henderson and TJ. Dougherty (eds). New York:
Marcel Dekker, pp. 37-46.
Dubbelman, T .M.A.R., Van Stevenillck, A.L., and
Van Steveninck, J. (1983). Hematoporphyrin induced
photo-oxidation and photodynamic cross-linking of nucleic acids and their constituents. Biochim. Biophys.
Acta 719.47-52.
240
22. Henderson, B.W .. and Dougherty, T.l. (1992). How
does photodynamic therapy work? J. Photochem. PhotobioI. 55, 145--157.
23. Richter, A.M., Waterfield, E .• Jain, A.K., Canaan,
AJ., Allison, B.A., and Levy. lG. (1993). LiposomaJ
delivery of a photosensitizer, henzoporphynn monoacid
ring A (BPD) to tumor and tissues in a mouse model.
Photochem. Pho{obio\., 57, 1000-1006.
24. de Schmidt, P.c., and van Berkel, T.J. (1990). LDLmediated drug tnrgetting, in: CriJiclll Reviews in Therapeutic Drug Carrier Sy~·t~ms. Boca Raton, FL eRC
Press, 7, pp. 99-119.
25. Vitols, S. (1991). Uptake oflow-density lipoproteins by
malignant cells-Possible therapeutic applications.
Cancer Cells 3, 488-495.
26. Reddi, E.S., Cernuschi, S., Biolo. R., and Jovi, G.
(1990). Liposome- or LDL-administered Zn(II)phthalocyanine !Hi a photodynamic agent for tumors
III. Effect of cholesterol on phannacokinetics and phototherapeutic properties. La.~ers Med. Sci . :; , 139343.
27. Kessel, D., Whitcomb, K.J .. and Schulz, V. (1992).
Lipoproteins-mediated distribution of N-aspartyl ch lorin
e 6 in the mouse. Photochem. Pbotobiol. 56, 51-56.
28. Henderson, B.W. (1990) . The significance of vasculalUre photosensitization in PDT. SPIE Inst. Ser. IS6,
153-166.
29. Paquette, B., and Van Lier, I.E. (1992). Phthalocyanines and related compounds: Structure activity relationship... , in: Photodynamic Therapy: Basic Principles and
Clinical Applications. B.W. Henderson and TJ.
Dougherty (OOs.). New York: Marcel Dekker, pp. 145156.
30. Morgan, A.R . , Kreimer-Birnbaum, M .. Garbo, O.M.,
Kecks, R.Q., and Selman, S.H. (1987). Proc. SPJE Int.
Soc. Opt. 847, 185--188.
31. Dodd, NJ.F., Moore, J.V., Poppitt, D.G., and Wood,
B. (1989). In vivo magnelic resonance imaging of the
effects of photodynamic therapy. Br. J. Cancer 60, 160167.
32. Wieman, T.J., Mang, T.S . , Fingar, V.H., Hill, T.G.,
Reed, M.W.R., Corey, T,S" Nguiyen, V.G., and Render, E.R. (1990). Effect of photodynamic therapy on
blood flow in nomlal and tumor blood vessels. Surgery
104,512-517.
33. Cohen, L., and Schwartz, S. (1966). Modifications of
radiosensitivity of porphyrin!; 11. Transplanted rhabdomyosarcoma in mice. Cancer Res. 26, 1969-1976.
34. Canti, G., Franco, P., Marelli, 0., Ricci, L., and
Nicolin, A. (1984). Hematoporphyrin derivative rescue
from (oxicity caused by chemotherapy or radiation in
murine leukemia model (LI2lO). Cancer Res 44, 15511556.
35. EImers, C.A .. Hnd Bowen. K.D. (1986). Immunological suppression in mice treated with hematoporphyrin
derivative. Cancer Res. 46, 1608-1611.
36. Schumaker. B.P., and Hetzel, F.W. (1987). Photodynamic therapy in the treatment of bladder carcinoma.
Photochem. Photobiol. 46, 899-90 1.
Sternberg and Dolphin
37. Evans, S., Matthews, W .. Perry, R., Fraker, D ..
Norton, J., and Pass, H.I. (1990). Effects of PDT of
tumor necrosis factor production by murine macrophages. JNCI 82, 34-39.
38. Bellnier. D.A. (1991). Patentiation of PDT in mice with
recombinant human necrosis factor-a. Photochcm. Photobiol. 8,203-210.
39. Fingar, V.H., Wieman, T.J., amI Dunk. K.W. (1990).
Role of thromooxane and prostacyclin release of photodynamic therapy induced tumor destruction. Cancer
Res. 50,2599-2603.
40. 19narro, LJ. (1989). Heme-dependent activation of soluble guanylate cyclase by nitric oxide: Regulation of
enzyme activity by porphyrins and metal1oporphyrins
seminars in Hematology 26,63-76.
41. Geels, R.S .. Baur. D.P., Treat, D.W., Bringars, R.D.,
Welch, D.F., and Scifres, D.R. (1992). 3W CW Laser
diodes operating at 633 nm . Electrical LeU. 28, 10431047.
42. Marynissen, l.P.A., Jansen, H., and Starr, W.M.
(1989). Treatment systems for whole bladder wall photodynamic therapy with in vivo monitoring and control
of light dose rate and dose. J. Urol. 142, 1351-1357.
43. Monnier, P., Savary, M., Fontolliet, C., Wagnieres,
G .. Chatelain, A .• Cornaz, P ., Despeursinge, C.H., and
Van Den Bergh, H. (1990). Photodetection and photodynamic therapy of "early" squamous cell carcinoma of
Ihe pharynx, esophagus and tracheobronchial lree. Lasers Med. Sci .. 5, 149-169.
44. Marcus, S.L. (1992). Clinical photodynamic therapy:
The continuing evolution, in: Photodynamic Therapy:
Basic Principles a/ld Clinical Applications. B.W. Render~on and TJ. Dougherty (eds). New York: Marcel Dekker, pp. 219-269.
45. (a) Nseyo, V.O., Lindahl, S.L, and Merril D.C.
(1990). Whole bladder wan photodynamic therapy.
Urology 36, 398-404. (b) Clinical package for Photofrin dll available from Quadra Logic Technologies Inc.,
Vancouver, B.C., (604) 872-7881.
46. Ris, H.B .. AltermaU, H.I .• IndcrbitzL R., Hess, R.,
Nachfur, B., Stewart, J.C.M., Wang, Q., Lim, C.K.,
Bonnett, R., Berenbaum. M.e., and Althaus, U.
(1990). Sr. 1. C1lem. 64, 1116-1120.
47. Allen, R.P . , Kessel, D., Than-at, R,S" and Volz, W.
(1992). Photodynamic Iherapy of superficial malignancies wirh NPe6 in man, in: Photodynamic Therapy a71d
Biomedical Lasers, P. Spinelli. M. Doll Fante, and R.
Marchesini (eds.). The Netherlands: Elsevier Science
Publishers B. V .• pp. 441-446.
48. Private communication, R.P. Allen, University of California Davis, Medical School.
49. North. 1., Ncyndorff, H., King D., and Levy. J.G.
(1992). Viral inactivation in blood and red cell concentrates with benzoporphyrin derivative. Blood Cells 18,
129-140.
50. Sternberg, E., and Dolphin, D. (1992). An overview of
second generation drugs for photOdynamic ther-dPY including BPDMDA (benzoporphyrin derivative), in:
PhoTodynamic Therapy and Biomedical Lasers. P.
Second Generation Photodynamic Agents
Spinelli~
M. Dal Fante, and R. Marchesini (cds.). The
Netherlands: Elsevier Science Publishers B. V., pp.
470-474.
51. Lui H, Hruza, L., Kollias, N., Wimberly, J. t Salvatori,
V., and Anderson, R.R. (993). Pmc. SPIE. lnt. Soc.
Opt. 1987, 147-151.
241
Address reprint requests to;
Ethan D. Sternberg, Ph.D.
Depanmenr oj Chemistry
University of British Columbia
2036 Main Mall
Vancouver, B.C .. Canada V6T IZI