Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
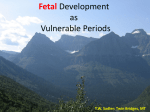
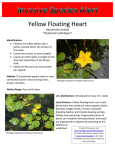
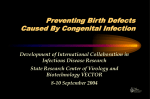
MICHIGAN DEPARTMENT OF COMMUNITY HEALTH Birth Defects The Michigan Monitor Spring 2010 Volume 4, Issue 1 Following trends, promoting prevention and linking families to resources Health Disparities and Birth Defects Health Disparities and Birth Defects 1 Risk Factors for Heart Defects 1 Prevalence and Mortality Rates 2 CSHCS Enrollment 3 Public Health Implications 3 Resources 3 Program Updates 4 Points of Interest 9Black infants repre‐ sent 18% of Michigan live births and 26% of infants in the MBDR born in 2004‐2006. 9Racial disparities exist in the rates of birth defects and in the rates of risk fac‐ tors for birth defects. 9Maternal exposures of cigarette smoking and alcohol consump‐ tion can increase the risk of a baby being born with a heart defect. Health disparities impact both women’s health and pediatric health care in Michigan, as they do nationally. Disparities affect reproductive outcomes, including birth defects. At the same time, disparities in pediatric health care mean that children with birth defects who are from minority groups may have poor outcomes long term relative to those of whites.1,2 This issue of the Michigan Monitor explores certain health disparities per Michigan Birth Defects Registry (MBDR) reporting. Michigan data from 2004‐2006 reveals that black infants are over‐represented in the MBDR, where about 26% of those reported are black, compared to about 18% of all Michigan births. White infants make up about 70% of those reported to the MBDR, while they account for about 78% of all Michigan births. We begin to explore the racial disparity seen in the MBDR reporting by looking specifically at the prevalence of congenital heart defects, as well as select behavioral risk factors, mortality rates and enrollment in Children’s Special Health Care Services (CSHCS). Risk Factors for Congenital Heart Defects Drinking In the US, congenital heart defects (CHDs) occur in 9 out of 1000 live births. Only about 15% have a known cause.3,4 Research has shown that a woman’s socioeconomic and lifestyle risk factors such as maternal age, marital status, education, occupation, income, smoking, and alco‐ Smoking hol use are associated with CHDs.5 Smoking may increase the risk of CHDs by up to 48 percent, while alcohol consumption during the first trimester may double the risk of some CHDs.5,6 These potential risks are in addition to proven associations between low birth weight and maternal smoking and other fetal developmental ef‐ fects from alcohol exposure (fetal alcohol spectrum disorders). Due to these negative effects, the Healthy People 2010 campaign set the goal of increasing abstinence from tobacco and alcohol during pregnancy to 99% and 94%, respectively.2 To assess abstinence from these substances during pregnancy, we used MBDR data to All Birth Defects Heart Defects PRAMS 95 100 93 evaluate women who gave birth to an in‐ 87 88 86 89 84 90 81 fant with any birth defect, and women 76 80 73 74 73 who gave birth to an infant with a CHD. 70 We used the Michigan Pregnancy Risk As‐ 60 50 sessment Monitoring System (PRAMS), a 40 population‐based survey sent to mothers 30 2‐6 months after delivery, to assess general 20 trends in tobacco and alcohol abstinence 10 during the last three months of pregnancy. 0 Michigan has not met the Healthy People White Black White Black 2010 goals. All three sources show blacks Abstinence from Tobacco Abstinence from Alcohol were slightly more likely to abstain from tobacco and alcohol during pregnancy, Figure 1. The prevalence of abstinence from tobacco and alcohol during pregnancy: MBDR 1996‐2006,7 PRAMS 2006.8 than whites. Percent Inside this issue: Page 2 Volume 4, Issue 1 Congenital Heart Defects Nationally, the prevalence of heart defects has increased from Rate (per 10,000 live births) 300.0 62 cases to 90 cases per 10,000 live births from 1968 to 1997. In Michigan, the prevalence of CHDs reported by 2 years of age (1996‐2006) has remained relatively stable for whites (about 155 per 10,000), but has increased from about 182 cases to 264 cases per 10,000 live births for blacks. Research has shown that some increase in prevalence may be due to advances in technology and improved diagnostic techniques, but the reason for this gap between CHD rates in the white and black populations remains unknown. 4 The Birth Defects Program continues to research potential causes for the racial disparity. Some possible explana‐ tions include: improved access to care for blacks, maternal age differences, and differences in diagnostic methods for infants with multiple anomalies or low birth weight. 3 250.0 200.0 150.0 100.0 White Black 50.0 Total 0.0 1996-2002 1997-2003 1998-2004 1999-2005 2000-2006 Birth Year Figure 2. Seven year moving prevalence rate of heart defects diagnosed by 2 years of age, by race: MBDR, 1996‐2006.7 Ventricular and Atrial Septal Defects 30 While the overall prevalence rate for heart defects is higher for blacks than for whites, the rates for specific types of heart defects vary by race. In Michigan, as shown in Figure 3, the prevalence rate for atrial septal defects (ASDs) alone is higher in blacks, but the rate for ventricular septal defects (VSDs) alone is higher in whites. Other research has shown that heart defects such as trans‐ position of the great arteries and coarctation of the aorta occur more often in whites, while patent ductus arteriosus defects occur more often in blacks.3 Rate (per 10,000 live births) 25 20 15 10 White, ASD White, VSD 5 Black, ASD Black, VSD Normal Heart 0 1996-2002 1997-2003 1998-2004 1999-2005 Birth Year 2000-2006 Figure 3. Seven year moving prevalence rate of ventricular and atrial septal defects, without any other condition, diagnosed by 2 years of age, by race: MBDR, 1996‐2006.7 Figure 4. Diagram of normal heart, ASD and VSD.9 Infant Mortality and Congenital Heart Defects 6.0 Rate (per 10,000 livebirths) Infant mortality due to congenital heart defects has decreased 22.2%, on average, from 4.5 to 3.5 deaths per 10,000 live births from 1996‐2006.7 As seen in Figure 5, the infant mortality rate due to CHDs for both blacks and whites has decreased at about the same rate, but the black infant mortality rate has remained about 24% higher, on average, than the rate for whites. More‐ over, in whites, about 66% of infant deaths due to CHD occurred by three months of age while in blacks, about 60% of deaths occurred by three months of age. Nationally, infant mortality due to CHDs has declined by about 40% and is about 20% higher for blacks than for whites.4 Racial disparities are seen in overall infant mortality rates. The cause for disparities in CHD mortality is still unknown, but may be explained by access to care, compli‐ cations from additional defects, or other factors.4 5.0 4.0 3.0 Black Total White 2.0 1.0 0.0 1996-2002 1997-2003 1998-2004 1999-2005 2000-2006 Birth Year Figure 5. Seven year moving infant mortality rates due to con‐ genital heart defects by race, Michigan, 1996‐2006.7 Page 3 Volume 4, Issue 1 CSHCS Enrollment White Of children reported to the MBDR (born in 1996‐2005) who 50 45 40 35 30 25 20 15 10 5 0 Percent may have been eligible to receive Children’s Special Health Care Services (CSHCS) for a CHD, less than 45% were enrolled. CSHCS eligibility is based on diagnosis, severity, and chronicity, and enrollment is voluntary. Figure 6 shows the average percent of eligible children with CHDs who were enrolled by race. Of those who may be eligible for CSHCS due to a CHD, an average of about 38% of whites and about 32% of blacks were enrolled. Results must be interpreted with care as this data is dependent on the CHD being reported to the MBDR. More information is needed about the type and severity of the heart defects, individ‐ ual family circumstances and provider referral practices to better understand the variation in enrollment. Black 41 36 30 31 33 35 38 33 40 Total 43 41 40 35 34 23 1996-1997 1998-1999 2000-2001 2002-2003 2004-2005 Birth Year Figure 6. Average percent of eligible children with heart de‐ fects enrolled in CSHCS, by race: MBDR, 1996‐2005.7 Public Health Implications and Future Directions In Michigan, congenital heart defects occur in about 1.5 in 100 live births in whites and about 2.6 in 100 live births in blacks. The reason for this racial disparity is unknown. It may be partially explained by racial disparities in risk factors. Research focused on modi‐ fiable risk factors for CHDs, such as tobacco and alcohol use, obesity, and glycemic control of diabetes, is needed for evidence‐based, culturally appropriate, prevention and intervention services. These services are more ef‐ fective when targeted to specific populations. As set forth by Healthy People 2010, encouraging healthy lifestyles for all women may decrease the number of pregnancy complications associated with tobacco and alcohol use. Information and Resources From MDCH (www.Michigan.gov/mdch): The Tobacco Control Program (www.Michigan.gov/tobacco) has resources to help Quit Smoking. Fetal Alcohol Syndrome Pro‐ gram (www.Michigan.gov/fas) and the Bureau of Substance Abuse and Addiction Services (www.Michigan.gov/mdch‐bsaas) have resources to prevent, diagnose and treat Fetal Alcohol Syn‐ drome. Michigan birth defects statistics per MBDR reporting can be found online. MDCH has programs aimed at understand‐ ing causes and supporting action to prevent infant mortality. Learn more about Children’s Special Health Care Services is online at www.michigan.gov/cshcs. For information on congenital heart defects visit: the March of Dimes’ Pregnancy and Newborn Health Education Center; the Centers for Disease Control and Prevention’s National Center on Birth Defects and Developmental Disabilities; the National Institute of Health’s National Heart, Lung and Blood Insti‐ tute, and Nemours’ Kids Health. Find support and connect with other families at CongenitalHeartDefects.com. References 1. Flores G, and The Committee on Pediatric Research. Technical Report Racial and Ethnic Disparities in the Health and Health Care of Chil‐ dren. Pediatrics. 2010; 125: e979‐e1020. Published online Mar 29, 2010. Downloaded 30 Mar 2010 from www.pediatrics.org. 2. Maternal, Infant, and Child Health: Healthy People 2010, http://www.healthypeople.gov/document/html/volume2/16mich.htm 3. Botto LD, Correa A, Erickson JD. Racial and temporal variations in the prevalence of heart defects. Pediatrics. 2001; 107; e32. DOI: 10.1542/peds.107.3.e32. 4. Botto LD, Correa A. Decreasing the burden of congenital heart anomalies: an epidemiologic evaluation of risk factors and survival. Pro‐ gress in Pediatric Cardiology. 2003; 18: 111‐121. 5. Kuciene R, Dulskiene V. Maternal socioeconomic and Lifestyle factors during pregnancy and the risk of congenital heart defects. Medicina. 2009; 45 (11). 6. Tikkanen J, Heinonen OP. Risk factors for atrial septal defect. European Journal of Epidemiology. 1992; 8: 500‐515. 7. Michigan Birth Defects Registry (MBDR) Data, 1996‐2006. 8. Protas B, Korzeniewski S, Grigorescu V. Michigan PRAMS Report 2006: Michigan Department of Community Health; Family and Com‐ munity Health, November 2008 9. Septal Defects. Pediatric Cardiac Center at the Children’s Hospital and Research Center. Found on 26 March 2009 at http://www.pediheartcho.org/septaldefects.htm Program Updates Following trends, promoting prevention and linking families to resources For more information or to receive future editions, please contact: Birth Defects Program Division of Genomics, Perinatal Health And Chronic Disease Epidemiology 201 Townsend St, CV-4 P.O. Box 30195 Lansing, MI 48913 Phone: Toll Free 1-866-852-1247 Hospital staff can now access the new web‐based electronic birth certifi‐ cate (EBC) reporting module on any PC with internet access. Staff can use the EBC module to add birth defect reports to the Michigan Birth Defects Registry (MBDR) at any time after a birth as been registered with the state. Visit the Mihealth Training page at the following link to take the online course for reporting birth defects using the new web‐based EBC: http://training.mihealth.org/coursedetail.htm#defect Acknowledgements We would like to thank the CSHCS Program and the MBDR Steering Committee for their continued support and contributions. You can find the Michigan Monitor online at www.michigan.gov/genomics ♦ ♦ Michigan is now smoke‐free. Smoking is prohibited in most public places in Michigan, as of May 1. ♦ About 9 out of every 1,000 babies is born with a heart defect. As many as 1.3 million Americans are living with heart defects. Suggested Citation Reimink B, Ehrhardt J, Bach J, Grigorescu V. Michigan Department of Community Health. Michigan Monitor. Volume 4, Issue 1. Spring 2010.