Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Atrial fibrillation wikipedia , lookup
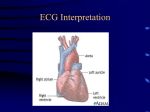
New Hampshire EMT-Intermediate Cardiology New Hampshire Division of Fire Standards & Training and Emergency Medical Services Objectives Describe the incidence, morbidity, and mortality of cardiovascular disease. Discuss prevention strategies that may reduce morbidity and mortality of cardiovascular disease. Identify the risk factors most predisposing to coronary artery disease. Objectives Describe the anatomy of the heart, including the position in the thoracic cavity, layers of the hear chambers, and location and function of cardiac valves. Identify the major structures of the vascular system. Describe the distribution of the coronary arteries and the parts of the heart supplied by each artery. Differentiate the structural and functional aspects of arterial and venous blood vessels. Objectives continued Define the following terms that refer to cardiac physiology: Stroke volume Starling’s Law Preload Afterload Cardiac output Blood pressure Describe the electrical properties of the heart. Describe the normal sequence of electrical conduction through the heart and state the purpose of this conduction system. Objectives continued Describe the location and function of the following structures of the electrical conduction system: (C-1) SA node Internodal and interatrial tracts AV node Bundle of His Bundle branches Purkinje fibers Define cardiac depolarization and repolarization and describe the major electrolyte changes that occur in each process. (C-1) Describe an ECG. (C-1) Explain the purpose of ECG monitoring and its limitations. (C-1) Objectives continued Define the following terms as they relate to the electrical activity of the heart: Isoelectric line QRS complex P wave State the numerical values assigned to each small and each large box on the ECG graph paper for each axis. Define ECG artifact and name the causes. Correlate the electrophysiological and hemodynamic events occurring throughout the entire cardiac cycle with the various ECG wave forms, segments and intervals. Relate the cardiac surfaces or areas represented by the ECG leads . Given an ECG, identify the arrhythmia. Describe a systematic approach to analysis and interpretation of cardiac dysrhythmias. Objectives continued Describe the dysrhythmias originating in the sinus node and the ventricles. Describe the process and pitfalls of differentiating wide QRS complex tachycardias. Describe the term “cardiac arrest”. Describe the arrhythmias seen in cardiac arrest. Identify the critical actions necessary in caring for the patient with cardiac arrest. Explain how to confirm asystole using the 3-lead ECG. List the clinical indications for defibrillation. Describe the most commonly used pharmacological agents in the management of cardiac arrest for EMT-Intermediates. Identify resuscitation. Identify circumstances and situations where resuscitation efforts would not be initiated. Identify local protocol dictating circumstances and situations where resuscitation efforts would be discontinued. Objectives continued Integrate the pathophysiology principles to the assessment of the patient with cardiac arrest. Synthesize assessment findings to formulate a rapid intervention for a patient in cardiac arrest. Describe the conditions of pulseless electrical activity. Value and defend the urgency in rapid determination of and rapid intervention of patients in cardiac arrest. Identify the location of the structures listed in cognitive objective #2. Demonstrate how to set and adjust the ECG monitor settings to varying patient situations. Demonstrate a working knowledge of various ECG lead systems Demonstrate satisfactory performance of psychomotor skills of basic and advanced life support techniques according to the current American Heart Association standards and guidelines, including: Cardiopulmonary resuscitation Defibrillation Demonstrate how to record an ECG Incidence Prevalence of cardiac death outside of a hospital Prevalence of warning signs and symptoms for cardiac emergencies Supportive statistics Supportive statistics Increased recognition of need for early reperfusion Morbidity/ mortality Reduced with early recognition Reduced with early access to EMS system Risk factors Age Family history Hypertension Lipids Male sex Smoking Carbohydrate intolerance Possible contributing risks Diet Female sex Obesity Oral contraceptives Sedentary living Personality type Psychosocial tensions Prevention Strategies Early recognition Education Alteration of life style Anatomy of the Heart Anatomy of the heart Tissue Layers Pericardium: protective sac surrounding the heart. Two layers. Myocardium: middle layer of the heart, unique muscle cells that have the ability to conduct electrical impulses from one muscle cell to another, thus allowing the heart to contract Endocardium: inner layer of heart, bathed in blood Tissue Layers Pericardial Membrane Chambers Atria: superior chambers that receive incoming blood Right & Left Ventricles: inferior chambers that pump blood out of the heart Right & Left Heart Valves Tricupid Valve: right aterioventricular valve; 3 cusps or leaflets Bicupid (Mitral) Valve: left aterioventricular valve; 2 cusps or leaflets Pulmonic Valve: right semilunar valve Aortic Valve: left semilunar valve Coronary Circulation Left Coronary Artery Anterior Descending Artery Circumflex Artery Right Coronary Artery Posterior Descending Artery Marginal Artery Blood flow of the heart Cardiac Cycle Right and left Ventricles contract together Pressure of contraction produces closure of AV valve and opens aortic and pulmonic valves Systole: Contraction phase, usually referring to ventricular contraction Disatole: relaxation phase, usually referring to ventricles, much longer than systole (.52 seconds versus .28 seconds) As rate increases, length of diastole decreases with less reduction in length of systole Phase during which most coronary artery filling occurs (about 70%) Vascular System Arterial System arteries arterioles capillaries Venous System venules veins Cardiac Physiology To understand EKGs you must thoroughly understand the pumping actions of the cardiac cycle Diastole: relaxation phase Systole: contraction phase Cardiac Physiology Stroke volume Starling’s Law Preload Afterload Cardiac Output Blood Pressure Electrical Properties of the Heart Sinoatrial (SA) node Internodal and interatrial tracts Atrioventricular (AV) node Bundle of His Bundle branches Purkinje fibers Depolarization Process by which muscle fibers are stimulated to contract by the alteration of the electrical charge of a cell. Accomplished by changes in electrolyte concentrations across the cell membrane. Intrinsic Rates Pacemaker cells capable of self initiated depolarization Found throughout conduction system except AV node SA node: 60-100/minute intrinsic rate AV Junction tissue: 40-60/minute intrinsic rate Ventricles (bundle branches & Purkinje fibers): 20-40/minute intrinsic rate Repolarization Once cells have depolarized, the electrolytes are pumped back to their resting or polarized state. This process is called repolarization. Autonomic nervous system relationship to Cardiovascular system Medulla Carotid sinus and baroreceptor Location Significance Parasympathetic system Sympathetic Alpha-vasoconstriction Beta Inotropic Dromotropic Chronotropic ECG Monitoring EGC Monitoring Electrical activity of the heart Does NOT indicate mechanical activity of the heart. Must take a pulse. ECG Components Relationship of ECG to the heart Dysrhythmias are the most common complication within the first few hours of chest pain Life-threatening – usually ventricular fibrillation Non-life-threatening – may require prehospital intervention Warning dysrhythmias – may be forerunners of life-threatening dysrhythmias and require pre-hospital intervention Basic concepts of ECG monitoring ECG is graphic display of heart’s electrical activity Body acts as a giant conductor of electrical current ECG obtained by applying electrodes on body surface which detect changes in voltage of cells between sites of the electrodes Basic concepts of ECG monitoring Voltage may be positive (upward deflection) or negative (downward deflection) These changes are input to ECG machine, amplified and displayed visually on a scope and/or graphically on ECG paper Recorded as a continuous curve of waves and deflections called the electrocardiogram (ECG) Monitoring lead: any lead that shows very clear wave forms, very often, lead II Information that can be gained from a monitoring lead or rhythm strip: How fast the heart is beating How regular the heartbeat is ECG Graph Paper Artifact Deflections on the ECG display produced by factors other than the heart’s electrical activity such as: Standardization (calibration) marks Muscle tremors/shivering Patient or vehicle movement Loose electrodes 60-cycle interference Machine malfunction Steps to rhythm interpretation 1. Estimate Heart Rate 2. Is the rhythm regular? 3. Are there P waves? 4. Is the QRS wide or narrow? 5. Is there a relationship between P waves and QRS complexes? 1. Estimate Heart Rate 1. Estimate Heart Rate Is the atrial rate the same as the ventricular? Using the 300 rule, what is the rate? What is the rate? 2. Is the rhythm regular? Is it regular? Is it irregular? 2. Is the rhythm regular? Is it regular? Is it irregular? 2. Is the rhythm regular? Is it regular? Is it irregular? Are there any ectopic beats? 3. Are there P waves? Are the P waves regular? What is the morphology? (upright rounded and uniform) Do all the P waves look alike? 3. Are there P Waves? Are the P waves regular? Is there one P wave for every QRS? What is the morphology? (upright, rounded and uniform) Are there more P waves then QRSs? Do all the P waves look alike? 3. Are there P Waves? Are the P waves regular? Is there one P wave for every QRS? What is the morphology? (upright, rounded and uniform) Are there more P waves then QRSs? Do all the P waves look alike? 3. Are there P waves? Are the P waves regular? Is there one P wave for every QRS? What is the morphology? (upright, rounded and uniform) Are there more P waves then QRSs? Do all the P waves look alike? 4. Is the QRS wide or narrow? Normal range < 0.12 4. Is the QRS wide or narrow? Normal range < 0.12 5. Is there a relationship between P waves and QRS complexes? Normal PR interval = 0.12 – 0.20 Are all the PR intervals’ constant? Is the PR interval measurement within normal limits? If the PR interval varies, is there a pattern to the change in measurements? 5. Is there a relationship between P waves and QRS complexes? Normal PR interval = 0.12 – 0.20 Are all the PR intervals’ constant? Is the PR interval measurement within normal limits? If the PR interval varies, is there a pattern to the change in measurements? Ectopic Beat (Complex) •1. Estimate Heart Rate •2. Is the rhythm regular? •3. Are there P waves? •4. Is the QRS wide or narrow? •5. Is there a relationship between P waves and QRS complexes? •1. Estimate Heart Rate •2. Is the rhythm regular? •3. Are there P waves? •4. Is the QRS wide or narrow? •5. Is there a relationship between P waves and QRS complexes? •1. Estimate Heart Rate •2. Is the rhythm regular? •3. Are there P waves? •4. Is the QRS wide or narrow? •5. Is there a relationship between P waves and QRS complexes? •1. Estimate Heart Rate •2. Is the rhythm regular? •3. Are there P waves? •4. Is the QRS wide or narrow? •5. Is there a relationship between P waves and QRS complexes? Rhythms of the SA Node Sinus Rhythm Sinus Bradycardia Sinus Tachycardia Sinus Arrhythmia Sinus Rhythm 1. Rate: 60 - 100/minute 2. Is the rhythm regular or irregular? Regular 3. Are there P waves? Yes PR Interval: 0.12 - .0.20 seconds 4. Is the QRS wide or narrow? Narrow 5. Is there a relationship between P waves and QRS complexes? Yes 1:1 ratio Normal Sinus Rhythm Sinus Bradycardia 1. Rate: < 60/minute 2. Is the rhythm regular or irregular? Regular 3. Are there P waves? Yes PR Interval: normal to slightly prolonged 4. Is the QRS wide or narrow? Narrow 5. Is there a relationship between P waves and QRS complexes? Yes 1:1 ratio Sinus Tachycardia 1. Rate: > 100/minute 2. Is the rhythm regular or irregular? Regular 3. Are there P waves? Yes PR Interval: normal to slightly shortened 4. Is the QRS wide or narrow? Narrow 5. Is there a relationship between P waves and QRS complexes? Yes 1:1 ratio Sinus Arrhythmia 1. Rate: 60 - 100/minute 2. Is the rhythm regular or irregular? Irregular 3. Are there P waves? Yes PR Interval: Normal 4. Is the QRS wide or narrow? Narrow 5. Is there a relationship between P waves and QRS complexes? Yes 1:1 Ventricular Rhythms Idioventricular rhythm Accelerated idioventricular rhythm Premature ventricular complex (ventricular ectopic) Ventricular tachycardia Ventricular Fibrillation Idioventricular Rhythm 1. Rate: 20 - 40/minute 2. Is the rhythm regular or irregular? regular 3. Are there P waves? No PR Interval:None 4. Is the QRS wide or narrow? Wide 5. Is there a relationship between P waves and QRS complexes? No P Waves Accelerated Idioventricular Rhythm 1. Rate: 40 - 100/minute 2. Is the rhythm regular or irregular? regular 3. Are there P waves? No PR Interval: none 4. Is the QRS wide or narrow? Wide 5. Is there a relationship between P waves and QRS complexes? No P waves Premature Ventricular Complex (PVC) 1. Rate: depends on underlying rhythm 2. Is the rhythm regular or irregular? Irregular 3. Are there P waves? None in the PVC PR Interval: None 4. Is the QRS wide or narrow? Wide; bizarre appearance 5. Is there a relationship between P waves and QRS complexes? None in PVC Ventricular Tachycardia 1. Rate: 100 - 250/minute 2. Is the rhythm regular or irregular? regular 3. Are there P waves? None or dissociated PR Interval: None 4. Is the QRS wide or narrow? Wide; bizarre appearance 5. Is there a relationship between P waves and QRS complexes? No Ventricular Tachycardia Ventricular Tachycardia Ventricular Fibrillation 1. Rate: Indeterminate 2. Is the rhythm regular or irregular? Chaotic 3. Are there P waves? None PR Interval: None 4. Is the QRS wide or narrow? None 5. Is there a relationship between P waves and QRS complexes? No P waves, no QRS complexes Ventricular Fibrillation Ventricular Fibrillation Asystole 1 . Rate: Indeterminate 2. Is the rhythm regular or irregular? No rhythm 3. Are there P waves? None PR Interval: None 4. Is the QRS wide or narrow? None 5. Is there a relationship between P waves and QRS complexes? No P waves, no QRS complexes Asystole Check your patient. (apneic/pulseless) Check your leads. Check Connections to monitor. Check more then one lead. What are these rhythms? What are these rhythms? Asystole P.E.A. Pulseless Electrical Activity There is electrical activity on the monitor, but there is no pulse The Hs & Ts Hypovolemia Hypoxia Hypothermia Hydrogen Ions (acidosis) Hypo/hyperkalemia Hypoglycemia Tamponade Tension Pneumo Thrombosis, pulmonary (embolism) Thrombosis, coronary (ACS) Toxins (OD) Trauma (hypovolemia) Reversible causes for Hs Hypovolemia = give them fluid Hypoxia = oxygenate and ventilate Hypothermia = warming Hydrogen Ions = can be treated by the paramedic with sodium bicarbonate Hypo/hyperkalemia: hyperkalemia can be treated by the paramedic with sodium bicarbonate Hypoglycemia = D50 Reversible causes for Ts Tamponade: Pericardiocentesis Tension Pneumo: Needle decompression Thrombosis, pulmonary (emboli): Surgery, thrombolytics Thrombosis, coronary (ACS): Thrombolytics Toxins (OD): Depends what agent overdoses on. Narcan. Trauma: fluids Many treatments are done by paramedics or physician, early recognition of PEA and early paramedic intercept can be life saving QUESTIONS? Special Thank You to: Christopher Rousseau, NREMT-I