Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
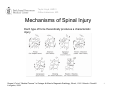
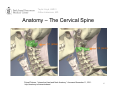
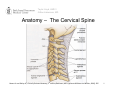
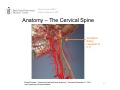
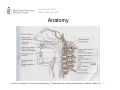
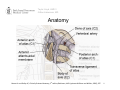
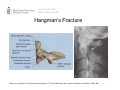
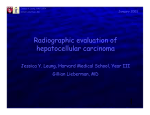
Taylor Lloyd, HMS 3 Gillian Lieberman, MD Cervical Spine Trauma and Relevant Imaging Modalities Taylor Lloyd, Harvard Medical School III Dr. Gillian Lieberman, MD November 2011 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Outline • • • • • • Case Presentation Mechanisms of Injury Differential Diagnoses Imaging Modalities Anatomy Film Interpretation 2 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Case 1 • 43 year old female restrained driver in motor vehicle crash at 40mph • Airbag deployed • Felt immediate neck pain without radiation • No weakness of extremities, bowel, or bladder dysfunction • Also experiencing some hip pain • What are the structures of concern? • What is the role of imaging? 3 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Mechanisms of Spinal Injury Each type of force theoretically produces a characteristic injury Rogers LF et al. “Skeletal Trauma.” In Grainger & Allison's Diagnostic Radiology, 5th ed., 1016. Orlando: Churchill Livingston, 2008. 4 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Differential Diagnosis (Structures of Concern) • Spinal cord injury • Compression (hemorrhage, edema, spondylolethisis) • Transection • Vertebral fracture • Unstable • Stable • Ligamentous injury • Unstable • Vascular injuries • Vertebral arterial injury: in some case series, up to 46% of patients with MAJOR blunt cervical trauma 5 Taylor Lloyd, HMS 3 Gillian Lieberman, MD NEXUS guidelines : To image or not to image.. Based on prospective, observational study, n=34,069 High sensitivity, 99.0% (95% CI 98-99.6%) Low specificity, 12.9% Cervical spine radiography is indicated unless ✗ the patient meets ALL 5 criteria: ✔– ✔– ✔– ✗ – No posterior midline cervical tenderness No evidence of intoxication Normal level of alertness No focal neurologic deficit – No painful distracting injury Hoffman JR. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X‐Radiography Utilization Study Group. N Engl J Med. 2000;343(2):94. 6 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Menu of Tests • Plain Film – 3 views (lateral, odontoid, AP) • CT – With sagittal and coronal reconstructions • MRI 7 Taylor Lloyd, HMS 3 Gillian Lieberman, MD To CT or not CT.. Based on meta-analysis of 7 randomized control trials and cohort studies, wherein 3 studies n >1000 Study inclusion criteria: CT and plain films in the setting of blunt cervical spine trauma. Gold standard varied CT pooled sensitivity, 98% (95% CI, 96-99%) Plain film pooled sensitivity, 52% (95% CI, 47-56%) Recommendations: – CT is preferred modality for high-risk patients – Insufficient evidence that CT should replace plain films in patients at low risk of C-spine injury Holmes JF, Akkinepalli R. Computed tomography versus plain radiography to screen for cervical spine injury: a meta-analysis. J Trauma. 2005;58(5):902 8 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Anatomy – The Cervical Spine C1 (atlas) C2 (axis) Primal Pictures. “Interactive Head and Neck Anatomy.” Accessed November 11, 2011. http://anatomy.tv/interactivehead. 10 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Anatomy – The Cervical Spine Moore KL and Dalley AF, Clinically Oriented Anatomy, 5th edition (Baltimore, MD: Lippincott Williams and Wilkins, 2006), 505. 11 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Anatomy – The Cervical Spine Vertebral Artery (superior to C1) Primal Pictures. “Interactive Head and Neck Anatomy.” Accessed November 11, 2011. http://anatomy.tv/interactivehead. 12 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Anatomy Moore KL and Dalley AF, Clinically Oriented Anatomy, 5th edition (Baltimore, MD: Lippincott Williams and Wilkins, 2006), 507. 13 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Anatomy Moore KL and Dalley AF, Clinically Oriented Anatomy, 5th edition (Baltimore, MD: Lippincott Williams and Wilkins, 2006), 507. 14 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Anatomy Anterior views with cross-section of occipital condyles, atlas (C1), and axis (C2) Moore KL and Dalley AF, Clinically Oriented Anatomy, 5th edition (Baltimore, MD: Lippincott Williams and Wilkins, 2006), 487. 15 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Steele’s Rule Superior View of Atlanto-Occipital Joint Anterior Posterior Moore KL and Dalley AF, Clinically Oriented Anatomy, 5th edition (Baltimore, MD: Lippincott Williams and Wilkins, 2006), 510. 16 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Case 1 Status-Post MVA Fracture CT Coronal and Sagittal Planes Cross-Referenced 17 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Case 1 Status-Post MVA Fracture 18 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Hangman’s Fracture: Traumatic spondylolysis of C2: often a result of head hyperextension UPON the neck Posterosuperior view of hangman’s fracture of C2 vertebra Moore KL and Dalley AF, Clinically Oriented Anatomy, 5th edition (Baltimore, MD: Lippincott Williams and Wilkins, 2006), 488. 19 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Hangman’s Fracture Moore KL and Dalley AF, Clinically Oriented Anatomy, 5th edition (Baltimore, MD: Lippincott Williams and Wilkins, 2006), 488. 20 Taylor Lloyd, HMS 3 Gillian Lieberman, MD MRI Findings T2 Weighted MRI, Sagittal Cross‐Section 21 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Undisplaced Hangman’s Fracture Fracture of the pars interarticularis Rogers LF et al. “Skeletal Trauma.” In Grainger & Allison's Diagnostic Radiology, 5th ed., 1018. Orlando: Churchill Livingston, 2008. 22 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Hangman’s Fracture with Subluxation Widely displaced neural arch fracture Subluxation of C2 upon C3 Rogers LF et al. “Skeletal Trauma.” In Grainger & Allison's Diagnostic Radiology, 5th ed., 1018. Orlando: Churchill Livingston, 2008. 23 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Widely Displaced Hangman’s Fracture Fragment anterior and inferior to C2 vertebral body Wide separation of fracture fragments Locking of C2 facets anterior to C3 Rogers LF et al. “Skeletal Trauma.” In Grainger & Allison's Diagnostic Radiology, 5th ed., 1018. Orlando: Churchill Livingston, 2008. 24 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Our Patient Halo brace 25 Taylor Lloyd, HMS 3 Gillian Lieberman, MD Acknowledgements: • • • • Dr. Ammar Sarwar Dr. Karen Lee Dr. Gunjan Senapat Dr. Gillian Lieberman 26