Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
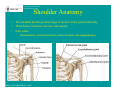
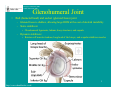
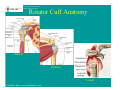
Gregory Cvetanovich, MS3 Gillian Lieberman, MD May 2011 A Compendium of Rotator Cuff Imaging Gregory Cvetanovich, Harvard Medical School Yr 3 Gillian Lieberman, MD Gregory Cvetanovich, MS3 Gillian Lieberman, MD Overview • Patient presentation • Rotator cuff – Anatomy – Function – Pathology • Menu of radiologic tests • Normal rotator cuff anatomy on MRI • MRI examples of rotator cuff tears 2 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Patient Presentation • 53 year-old woman presents to rheumatology clinic for routine follow-up six months after diagnosis of likely seronegative rheumatoid arthritis – Since beginning treatment with MTX, her bilateral joint pain and stiffness resolved with the exception of right shoulder pain – She has experienced right shoulder pain intermittently for a number of years, worsening with overhead activity and improving with rest and NSAIDs – In recent months, the right shoulder pain has worsened and become more frequent, sometimes awakening her at night. • Physical Exam: R shoulder exam significant for pain and weakness with limited ROM presumed secondary to pain – Clinic note does not document other details of shoulder physical exam, such as impingement signs or detailed rotator cuff exam 3 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Shoulder Anatomy • • • The shoulder has the greatest range of motion of any joint in the body Three bones: humerus, clavicle, and scapula Four joints: – Glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic 4 http://www.shoulderdoc.co.uk/ Gregory Cvetanovich, MS3 Gillian Lieberman, MD Glenohumeral Joint • Ball (humeral head) and socket (glenoid fossa) joint – Glenoid fossa is shallow, allowing large ROM at the cost of skeletal instability – Static stabilizers: • Glenohumeral ligaments, labrum, bony structures, and capsule – Dynamic stabilizers: • Rotator cuff muscles/tendons, long head of the biceps, and scapular stabilizer muscles 5 http://www.shoulderdoc.co.uk/ Gregory Cvetanovich, MS3 Gillian Lieberman, MD Rotator Cuff Anatomy and Function • Four muscles and their tendons – – – – – Supraspinatus Infraspinatus Teres minor Subscapularis Mnemonic “SITS” • Originate from the scapula • Form musculotendinous “cuff” that inserts on the proximal humerus (greater and lesser tuberosities) • Function: primary dynamic stabilizers of glenohumeral joint – Muscles actively compress the humeral head in the glenoid fossa – Counterbalance forces from large muscles acting on humerus – Contribute to humeral movement: external rotation (infraspinatus, teres minor), internal rotation (subscapularis), and abduction (supraspinatus) 6 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Rotator Cuff Anatomy Anterior Posterior Lateral UpToDate; http://www.shoulderdoc.co.uk/ 7 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Tendon of Long Head of Biceps • Not part of rotator cuff • Contributes to glenohumeral stability • Intimate anatomic relationship with rotator cuff and labrum – Originates at superior glenoid tubercle – Travels intraarticularly over the humeral head – Travels in bicipital groove between the greater and lesser tuberosities • Biceps tendinopathy and tendon rupture frequently is associated with rotator cuff pathology 8 http://www.shoulderdoc.co.uk/ Gregory Cvetanovich, MS3 Gillian Lieberman, MD Rotator Cuff Pathology • Most common reason for seeking treatment among patients with shoulder pain – 4.5 million office visits and 40,000 surgeries annually in USA • Subacromial impingement – Repetitive compression of rotator cuff between greater tuberosity and acromion – Pain with overhead activities – Risk factors: repetitive overhead activity (e.g. sports, occupations), narrow coracoacromial arch (from anatomic variants of acromion or bone spurs) – Spectrum of disease from subacromial bursitis, to tendinopathy (chronic injury to rotator cuff), to partial and full thickness rotator cuff tears • Rotator cuff tears – Etiology: extrinsic (chronic subacromial impingement) and/or intrinsic (tension overload such as from overhead throwing; tendon degeneration from aging, microvascular disease, and comorbidities such as RA) – Classically, patients have weakness/pain with overhead activities and at night • In reality, many tears are asymptomatic or produce mild pain – Supraspinatus is most commonly torn 9 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Menu of Radiologic Tests for Rotator Cuff • • • • Shoulder plain films Musculoskeletal ultrasound Magnetic resonance imaging MR Arthrography 10 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Companion Patient 1: Acromial Bone Spur on Shoulder Plain Film Plain films of shoulder • • • • Initial imaging modality for shoulder pain of any etiology Typical views include frontal, lateral, and outlet view Typically normal in cases of rotator cuff tear In impingement, outlet view may demonstrate hooked acromion or bone spur Normal outlet view Outlet view demonstrating bone spur (red circle) causing subacromial impingement 11 http://orthoinfo.aaos.org/topic.cfm?topic=a00032 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Companion Patient 2: High Riding Humeral Head on Shoulder Plain Film Plain films of shoulder • Humeral head may be high-riding in large or chronic rotator cuff tears AP view shows high-riding humerus, decreased acromiohumeral distance (black arrows), and secondary arthropathy with osteophytes (white arrow) 12 Moosikasuwan JB, Miller TT, Burke BJ. Rotator Cuff Tears: Clinical, Radiographic, and US Findings. RadioGraphics 2005; 25:1591. Gregory Cvetanovich, MS3 Gillian Lieberman, MD Companion Patient 3: Full-Thickness Supraspinatus Tear on Shoulder Ultrasound MSK ultrasound • Advantages: – Bedside evaluation of rotator cuff – Visualize moving tendons and compare to contralateral – No radiation exposure, low cost • Disadvantages: – Full rotator cuff may not be well visualized – Operator dependent – Limited evaluation of deeper structures such as labrum • Sensitivity for diagnosing rotator cuff tears is similar to MRI • Full thickness rotator cuff tear – Tendon is hypoechoic (fluid replaces the torn tendon) – Enhanced through transmission results in accentuation of cartilage, resulting in two hyperechoic lines from cartilage and cortex (“double cortex sign”) Hypoechoic supraspinatus Double cortex sign (black arrows) 13 Moosikasuwan JB, Miller TT, Burke BJ. Rotator Cuff Tears: Clinical, Radiographic, and US Findings. RadioGraphics 2005; 25:1591. Gregory Cvetanovich, MS3 Gillian Lieberman, MD Magnetic Resonance Imaging Magnetic Resonance Imaging • Highly sensitive and specific for rotator cuff tears • Provides information about chronicity, which informs treatment decisions • Excellent soft tissue visualization, including the labrum and capsule • Disadvantages: expensive, typical contraindications to MRI and gadolinium contrast (if used), CT is superior for evaluating fractures Technical Details • Patient supine, typically with arm slightly externally rotated • Usually performed without IV gadolinium (Gd) contrast • Phased array coil is applied to shoulder for best possible signal/noise ratio and spatial resolution • Using MR scout localizer images, typical imaging planes are – Axial sections from the top of the acromioclavicular joint to the inferior glenoid margin – Coronal oblique images parallel to the plane of the supraspinatus tendon, extending from subscapularis tendon anteriorly to infraspinatus and teres minor posteriorly – Sagittal oblique images are perpendicular to the plane of the coronal images, extending from the lateral aspect of the greater tuberosity to the body of the scapula • Typical sequences include: – Proton density or T1-weighted – define anatomy – Short tau inversion recovery (STIR) or T2-weighted with fat saturation – fluid sensitive 14 Gregory Cvetanovich, MS3 Gillian Lieberman, MD MR Arthrography MR arthrography • • • Inject dilute Gd contrast into glenohumeral joint under fluoroscopic guidance before MRI Creates joint effusion of Gd contrast that facilitates visualization of small rotator cuff tears, especially partial tears of the undersurface of the tendon, and tears of the labrum and capsule CT arthrography is an option when MRI is contraindicated or unavailable Injection of gadolinium into glenohumeral joint via the rotator interval approach 15 BIDMC PACS Gregory Cvetanovich, MS3 Gillian Lieberman, MD Rotator Cuff Tear: Full vs. Partial Tear on MRI • Full-thickness tear: – Tendon is discontinuous on anatomy-defining sequences – High signal (fluid) fills the tendon defect on fluid-sensitive sequences – Ancillary findings: fluid in subacromial space, tendon retraction, highriding humeral head, rotator cuff muscle atrophy, narrow coracoacromial arch (from bone spurs or acromial orientation) – MR arthrography: contrast traverses the rotator cuff tendon and enters the subacromial bursa on T1-weighted fat saturation sequences • Partial-thickness tear: – Articular surface (most common), bursal surface, or intrasubstance – Partial-thickness tendon discontinuity on anatomy-defining sequences – High signal (fluid) fills tendon defect on fluid-sensitive sequences – MR arthrography: contrast fills the defect in the case of partialthickness tears of the articular surface 16 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Rotator Cuff Tear: Sensitivity and Specificity of MRI and MR Arthrography • Full-thickness tear: – Conventional MRI: sensitivity 84-96%, specificity 94-98% – MR arthrography: sensitivity 98%, specificity 100% • Partial-thickness tear: – Conventional MRI: sensitivity 35-44%, specificity 85-97% – MR arthrography: sensitivity 84-95%, specificity 96-100% (data for articular surface tears only) 17 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Normal MRI Anatomy – Coronal Oblique 1 Infraspinatus Teres minor Deltoid MR arthrogram T1, fat suppression BIDMC PACS 18 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Normal MRI Anatomy – Coronal Oblique 2 Spine of scapula Head of humerus Deltoid MR arthrogram T1, fat suppression BIDMC PACS Infraspinatus Contrast in glenohumeral joint 19 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Normal MRI Anatomy – Coronal Oblique 3 Acromion Supraspinatus Tendon of long head of biceps Head of humerus Superior labrum Glenoid Deltoid Inferior labrum MR arthrogram T1, fat suppression BIDMC PACS 20 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Normal MRI Anatomy – Coronal Oblique 4 Distal clavicle Supraspinatus Coracoid process Head of humerus Deltoid Subscapularis MR arthrogram T1, fat suppression BIDMC PACS 21 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Normal MRI Anatomy – Sagittal Oblique Acromion Supraspinatus Tendon of long head of biceps Infraspinatus Head of humerus Teres minor Subscapularis Posterior MR arthrogram T1, fat suppression BIDMC PACS Anterior 22 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Normal MRI Anatomy – Axial Anterior Tendon of long head of biceps (in bicipital groove) Subscapularis Head of humerus Anterior labrum Glenoid Teres minor Posterior labrum Infraspinatus MR arthrogram T1, fat suppression BIDMC PACS Posterior 23 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Back to Our Patient • Shoulder plain films normal • Next step in appropriate workup for suspected rotator cuff tear would be ultrasound or MRI • In this case, MRI was performed 24 Gregory Cvetanovich, MS3 Gillian Lieberman, MD Our Patient: Full-Thickness Supraspinatus Tear on MRI Coronal oblique T2 with fat saturation Sagittal oblique T2 with fat saturation Acromion Fluid in subacromial space Supraspinatus tear Supraspinatus tear Findings: 1) High signal, full-thickness defect of the supraspinatus on this fluid-sensitive sequence, consistent with full-thickness supraspinatus tear. The tear is 8mm in width and there is 2cm of tendon retraction. 2) High signal consistent with fluid in subacromial space 3) Laterally sloping acromion with mild narrowing of distance from humeral head to acromion 25 BIDMC PACS Gregory Cvetanovich, MS3 Gillian Lieberman, MD Our Patient: Full-Thickness Supraspinatus Tear on MRI Coronal oblique proton density Supraspinatus tear Findings: Full-thickness discontinuity of supraspinatus tendon on this anatomy-defining sequence, consistent with full-thickness supraspinatus tear. 26 BIDMC PACS Gregory Cvetanovich, MS3 Gillian Lieberman, MD Companion Patient 4: Partial-Thickness Supraspinatus Tear Coronal oblique T2 with fat saturation Intact supraspinatus tendon fibers inserting on greater tuberosity * Findings: - Partial-thickness disruption of tendons of articular surface of supraspinatus with increased signal on fluid-sensitive sequences. -Consistent with high grade (>50% of tendon) articular surface partialthickness tear of supraspinatus -There is a tear of the superior labrum (*) 27 BIDMC PACS Gregory Cvetanovich, MS3 Gillian Lieberman, MD Companion Patient 5: Massive Full-Thickness Rotator Cuff Tear of Subscapularis, Supraspinatus, and Infraspinatus on MRI Axial proton density Coronal oblique T2 with fat saturation Coronal oblique T2 with fat saturation High-riding humeral head Full-thickness tear of subscapularis, with retraction and atrophy Full-thickness tear of infraspinatus, with retraction and atrophy Full-thickness tear of supraspinatus, with retraction and atrophy 28 BIDMC PACS Gregory Cvetanovich, MS3 Gillian Lieberman, MD Treatment of Rotator Cuff Tears • • • • Treatment options include: – Ice – Activity restriction – NSAIDs – Physical therapy – Glucocorticoid injection – Surgical repair: typically arthroscopic; open technique in some situations Choice of treatment depends on specific clinical scenario, including: – Partial-thickness versus full-thickness tear – Acute vs. chronic vs. acute-on-chronic tear – Age, comorbidities, and compliance of patient Factors that favor non-operative management include: – Partial-thickness tear, chronic tear, elderly patient, patient with multiple comorbidities, non-compliant patient, and tear with minimal or no symptoms Our patient is beginning non-operative treatment with physical therapy 29 Student Name, year Gillian Lieberman, MD Acknowledgements •Gillian Lieberman, MD •Corrie Yablon, MD •Johannes Roedl, MD •Mai-Lan Ho, MD 30 Gregory Cvetanovich, MS3 Gillian Lieberman, MD References • • • • • • • • • • • • • • • • • • Balich SM, Sheley RC, Brown TR, Sauser DD, Quinn SF. MR imaging of the rotator cuff tendon: interobserver agreement and analysis of interpretive errors. Radiology 1997; 204(1):191. Chundru U, Riley GM, Steinbach LS. Magnetic Resonance Arthrography. Radiol Clin N Am 2009; 47:471. Clark JM, Harryman DT 2nd. Tendons, ligaments, and capsule of the rotator cuff. Gross and microscopic anatomy. J Bone Joint Surg Am 1992; 74:713. De La Rosa TL, Wang AW, Zheng MH. Tendinosis of the rotator cuff: a review. J Musculoskel Res 2001; 5:143. De Maeseneer M, Van Roy P, Shahabpour M. Normal MR Imaging Anatomy of the Rotator Cuff Tendons, Glenoid Fossa, Labrum, and Ligaments of the Shoulder. Radiol Clin N Am 2006; 44:479. Ferrari FS, Governi S, Burresi F, Vigni F, Stefani P. Supraspinatus tendon tears: comparison of US and MR arthrography with surgical correlation. Eur Radiol 2002; 12(5):1211. Kassarjian A, Bencardino JT, Palmer WE. MR Imaging of the Rotator Cuff. Radiol Clin N Am 2006; 44:503. Keener JD, Wei AS, Kim HM, et al. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am 2009; 91:1405. Moosikasuwan JB, Miller TT, Burke BJ. Rotator Cuff Tears: Clinical, Radiographic, and US Findings. RadioGraphics 2005; 25:1591. Murrell GA, Walton JR. Diagnosis of rotator cuff tears. Lancet 2001; 357:769. Oh LS, Wolf BR, Hall MP, et al. Indications for rotator cuff repair: a systematic review. Clin Orthop Relat Res 2007; 455:52. Patton, WC, McCluskey GM 3rd. Biceps tendinitis and subluxation. Clin Sports Med 2001; 20:505. Reilly P, Macleod I, Macfarlane R, et al. Dead men and radiologists don’t lie: a review of cadaveric and radiological studies of rotator cuff tear prevalence. Ann R Coll Surg Engl 2006; 88:116. Simons SM, Dixon, JB, Kruse D. Presentation and diagnosis of rotator cuff tears. UpToDate, accessed 5/22/11. Simons SM, Kruse D. Rotator cuff tendinopathy. UpToDate, accessed 5/22/11. Teefey SA, Rubin DA, Middleton WD, Hildebolt CF, Leibold RA, Yamaguchi K. Detection and quantification of rotator cuff tears. Comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. J Bone Joint Surg Am 2004; 86-A(4):708. Wise JN, Daffner RH, Weissman BN, et al. Expert Panel on Musculoskeletal Imaging. American College of Radiology Appropriateness Criteria: Acute Shoulder Pain. Last review date 2010. Accessed 5/22/11. URL: http://www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria/pdf/ExpertPanelonMusculoskeletalImaging/AcuteShoulderPain.aspx Wolff AB, Sethi P, Sutton KM, et al. Partial-thickness rotator cuff tears. J Am Acad Orthop Surg 2006; 14:715. 31