Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
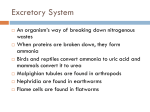
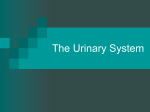
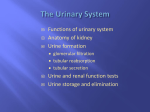
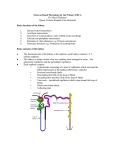
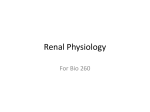
BY2202 The Kidney and Urinary Tract Origin, Form and Function 2 Dr. Neil Docherty Todays Objec-ves • To link functional phenomena (filtration, reabsorption, secretion) to functional endpoints (focus on volume regulation) • With respect to blood volume and cellularity, to describe the kidney as an effector of and responder to neurohormonal control • To detail the basic functional anatomy of the lower urinary tract and explain the basis for urinary continence The Renal Tubule Summary of Regions • • • • • • • Proximal convoluted tubule Proximal straight tubule Thick>thin descending limb of Loop of Henle Thin>thick ascending limb of Loop of Henle Distal convoluted tubule Connec>ng tubule Collec>ng tubule Functionality Associated With Nephron (8 KEYWORDS) The phenomena of FILTRATION, REABSORPTION and SECRETION As tuned by INTRINSIC and EXTRINSIC control mechanisms Leads to delivery on the key func>ons of • EXCRETION • VOLUME REGULATION • pH REGULATION N.B. Two types of nephrons Cortical (more excretory) Juxtamedullary (more involved in volume regulation) The Nature and Selectivity of The Glomerular Filter A selectively permeable barrier between blood and tubule lumen is formed It is essentially 3-layered 1) Endothelial layer 2) Basement membrane and 3) Visceral Epithelium Selectivity based on size (4.4nm) charge (-ve species repelled) Concept Check -‐Why filter the blood? The Glomerular Filtration Rate (GFR) And Its Determinants The overall GFR is the total volume of fluid filtered by the glomeruli of both kidneys per unit time NET PRESSURE (SINGLE NEPHRON) NET RATE (GLOBAL RENAL FUNCTION) Stroke Volume (SV)=70ml Heart Rate (HR)=72bpm CO=HR*SV=5040ml/min Renal Blood Flow(RBF)=20-‐25% of CO =Approximately 1L/min Renal Plasma Flow (RPF)=RBF*1-‐haematocrit =1000*0.6 =600ml/min Presuming pressures detailed on the right 20% of the RPF is subject to filtra>on =600*0.2=120ml/min =180L/day =Total ECF volume of body is filtered around 10 -mes/day! Alter Arteriolar Calibre-Alter The GFR Concept Check What would be the effect on the GFR of efferent arteriolar vasoconstriction? Filtration, Reabsorption and Secretion in The Tubule WASTE-Filter or secrete then excrete (e.g creatinine) NUTRIENT-Filter and reasorb (e.g. glucose) WATER/SALTS/IONS=Filter and fine tune reclamation or regulate secretion to achieve osmotic/volume and pH balance Following Reabsorption in The Tubule Filtrate from Bowman's capsule flows into the proximal tubule. Here all of the glucose, and amino acids, >90% of the uric acid and ~60% of salts are reabsorbed. A large volume of the water follows them by osmosis As the fluid flows into the descending segment of the loop of Henle, water con>nues to leave by osmosis 25% and reabsorp>on of salts (25%) in ascending segment In the distal tubules, more sodium is reclaimed by ac>ve transport, and s>ll more water follows by osmosis (5%). Final adjustment of water content of the urine occurs in the collec-ng tubules (10% of reabsorp>on) Concentration of The Urine • The kidneys filter the blood to rid it of waste and fine tune its composi>on/volume • Urine is the effluent from this process • Aim is maximum waste removal in minimal volume (ability to change volume depending on circulatory volume) • 180L of filtrate per day-‐only 1% (1-‐2L/day) excreted as urine Key Ques>on-‐How does the kidney manage to reclaim so much of the filtrate? Concentration of The Urine Relies on The Countercurrent Multiplier From Two Slides Back As the fluid flows into the descending segment of the loop of Henle, water con3nues to leave by osmosis with exclusive reabsorp3on of salts in ascending segment N.B. Urinary Concentra>on basically facilitated by • The countercurrent arrangement of the limbs of the Loop of Henle • Differen>al permeability to water therein • Arrangement of post-‐glomerular capillaries in parallel Visualising The Countercurrent Multiplier Values are mOsm (measure of osmotic strength) Example of Nutrient Reabsorption Glucose Reclamation in The Proximal Tubule • Same transport process as that seen in small intes>ne (seek lectures 18 and 19) • Saturable Concept Check Saturability of renal glucose transport explains the term diabetes mellitus. Can you make sense of this statement? Sensing of Filtration Pressure and Filtered Sodium Load Allow The Kidney To Monitor and Balance ECF Volume and Tonicity Imagine an acute decrease in blood volume 1) How will this affect CO? 2) How will this affect pressures in the renal blood vessels? 3) How will that in turn affect GFR? 4) How might the change in GFR affect sodium levels in the forming urine? • THE KIDNEY WILL ACT TO NORMALISE BLOOD FLOW AND ENHANCE RECLAMATION OF SODIUM AND WATER • IT DOES SO BY SENSING THESE CHANGES IN SPECIALISED AREAS OF THE RENAL BLOOD VESSELS AND TUBULE (THE JUXTAGLOMERULAR APPARATUS-JGA) • A MAJOR EFFECTOR OF HOMEOSTATIC CORRECTION IS THE RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM (RAAS) The Juxta-Glomerular Apparatus Afferent arteriolar pressure Macula densa in the distal tubule (salt sensor) Sympathe>c nervous input Juxtaglomerular cells renin release In Our Example An acute decrease in circula>ng blood volume reduces CO and GFR. This reduces stretch of the afferent arteriole and also reduces delivery of sodium to the macula densa through reduc>ons in GFR. More generally the drop in blood pressure has caused a reflex ac>va>on of renal sympathe-c nerves All of these changes conspire to induce juxtaglomerular cells to release the enzyme renin Renin and Angiotensin II Production In Our Example • Renin in turn causes genera>on of Angiotensin II (AngII) • The pressor effects of AngII are mul>ple N.B. Inhibi>on of AngII produc>on or receptor engagement is the cornerstone of treatment of hypertension We will focus on one mechanism-‐The Aldosterone Effect Aldosterone Links Renal Sodium Handling To Blood Volume and Pressure THE ALDOSTERONE EFFECT In the distal tubules, sodium is reclaimed by ac>ve transport, and s>ll more water follows by osmosis (5%). Final adjustment of water content of the urine occurs in the collec-ng tubules (10% of reabsorp>on) Aldosterone enhances the above (slow steroid hormone effect) through transcrip>onal mechanisms governing sodium channel and pump expression. Target of some diure>cs (e.g. spironolactone-‐ an aldosterone antagonist) Interes>ng Correlate-‐Hyperaldosteronism 1) Primary-‐Conn’s Syndrome 2) Secondary-‐Renal artery stenosis In Summary In Summary An acute decrease in circula>ng blood volume reduces CO and GFR. This reduces stretch of the afferent arteriole and also reduces delivery of sodium to the macula densa. More generally the drop in blood pressure has caused a reflex ac>va>on of renal sympathe-c nerves All of these changes conspire to induce juxtaglomerular cells to release the hormone renin which in turn causes genera>on of AngII. Among the pressor effects of AngII is induc>on of aldosterone synthesis and release from the adrenal cortex. This increase distal sodium and water reclama-on increasing volume and repressurising system On the Contrary • Increased pressure, GFR and salt delivery to the macula densa oppose renin release • High venous pressure/increased venous return to heart stretches right atrium wall • This releases atrial natriuretic peptide which effectively opposes everything on last slide • Hence promoting urinary sodium loss “natriuresis” and “depressurising” of the system The Kidney is An Oxygen Sensor and Influences Red Blood Cell Produc-on (Erythropoesis) Renal fibroblasts and oxygen sensing Storage and Expulsion of The Urine Blood Tubules Minor Calyx Major Calyx Renal Pelvis Ureter Bladder Urethra Substances cleared by renal excretion The Ureters-Location Muscular tubes taking urine from the kidneys to the bladder 30cm in length, 3mm lumen inside Retroperitoneal (attached to posterior wall of abdomen) Structure and Function of The Ureter Three Layer Structure 1) Transitional epithelium 2) Longitudinal and circular muscle 3. Adventitia (continuous with renal capsule) Function Pacemaker driven peristalsis The Uretero-Vesicular Junction Flap Valve Design to Prevent Reflux Urine passes out of the ureter into the bladder Firstly though, the ureter tunnels through the bladder wall This causes a flap valve to be made preventing urine from Refluxing into the ureter from bladder when full or during pressure increase at urination The Bladder-Location Hollow muscular organ for temporary storage of urine Located medially in the abdomino-pelvic cavity The Bladder-Gross Anatomy Ligaments attach superior part to the umbilicus Ligaments attach inferior,anterior and posterior parts to the Pelvic and public bone URETHRA The Bladder-Wall Structure SMOOTH MUSCLE SKELETAL MUSCLE Coordination of voluntary and involuntary muscle contraction required for continence and micturition Urinary Continence Today’s Learning Outcomes From today’s lecture you should be able to; 1) Link functional phenomena (filtration, reabsorption, secretion) to functional endpoints (with focus on renin-angiotensinII and aldosterone dependent mechanisms of volume regulation) 2) Briefly explain the role of the kidney as an oxygen sensor and source of hormonal control of red blood cell production (erythropoesis) 3) Detail the basic functional anatomy of the lower urinary tract and explain the basis for urinary continence • Any Ques>ons? [email protected]