Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
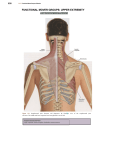
Oleh: Lenny MATERI: REGIO SHOULDER KOMPLEK 2. REGIO ELBOW 3. REGIO WRIST AND HAND 1. SHOULDER COMPLEX Composed of 4 articulations between the sternum, humerus, scapula, and clavicle. 3 synovial joints : Glenohumeraljoint, Acromioclavicularjoint (AC joint), Sternoclavicularjoint (SC joint) 2 functional articulations: Suprahumeral/subacromial, Scapulothoracic, TUJUAN INSTRUKSIONAL Mahasiswa memahami anatomi terapan dan biomekanik shoulder complex dengan cara : 1. 2. 3. 4. 5. Mampu mendefinisikan struktur jaringan spesifik shoulder complex Mampu membedakan topografis dan fungsi antara tiap struktur jaringan spesifik shoulder complex Mampu merinci tentang gerak shoulder complex Mampu menghubungkan struktur jaringan spesifik dengan patologi Mampu menghubungkan struktur jaringan spesifik dengan assessmen dan intervensi PERTANYAAN STUDI Sebutkan sendi pembentuk shoulder complex Sebutkan MLPP dan CPP sendi glenohumeral. Uraikan stabilitas pasif dan pasif sendi glenohumeral. Uraikan osteokinematik dan artrokinamatik sendi glenohumeral. Uraikan pembatas gerak abduksi; rotasi internal dan rotasi eksternal Uraikan arah traksi dan translasi sendi glenohumeral pada gerak abduksi; rotasi internal dan rotasi eksternal. Uraikan fungsi setiap jaringan spesifik pada sendi suprahumeral Berikan posisi palpasi pada: Bursa subdeltoidea; m. Supraspinatus: m. Infraspinatus; m. Subscapularis dan Biceps caput logus. Uraikan osteokinamatik dan artrokinematik sendi Acromioclavicularis; Sternoclavicularis dan Scapulothoracalis. Uraikan keterlibatan intervertebral dan costovertebral- costosternal dalam fungsi shoulder complex Uraikan Scapulohumeralrhythm ANATOMI TERAPAN 1. GLENOHUMERAL JOINT (humeral joint/ shoulder joint) ‘Ball and socket joint’ dibentuk oleh glenoid cavity Skapula yg concave landai menghadap kelateral serong cranio-ventral dan caput humerus yg convex. Jenis sendi: Sendi synovial. Relatif tidak stabil, membutuhkan bantuan stabilisasi dari struktur jaringan lain seperti: Pasif: Labrum, Glenohumeralligaments (Superior, middle, & inferior), Coracoacromialligament, Coracoclavicularligaments, Joint capsule Aktif: Muscular dynamic stabilizers: Rotator cuff, biceps tendon, muscles of scapular motion Gerakan Flexion-extension ROM. Flx: 1800 Ext: 600 stretched end feel (elastic), arthrokinematic: spin. Abduction dlm bidang frontal: ROM 900 elastic harder end feel. Arthokinematic: caudal translation External rotation dlm bidang tranversal ROM 800 elastic end feel, arthokinematic: ventral translation. Internal rotation dlm bidang tranversal ROM 900 elastic end feel, arthokinematic: dorsal translation. Horizontal Abd dan Horizontal Add dlm bidang trasversal ROM 1200 dan 300 elastic end feel. Arthokinematic: ventral translation & dorsal transl. Seluruh komponen diatas memiliki gerak arthrokinematic Traction dg arah lateral sedikit serong ventrocranial MLPP: posisi flexion–abduction 300 sedikit internal rotation. Posisi ‘Bonnet’ CPP posisi abduction – flexion penuh. Capsular pattern ROM: External rotationAbductionInternal rotation 2. SUPRAHUMERAL (JOINT) Merupakan celah antara acromion bagian atas dan head of humeri bagian bawah. Terdapat Bursa subdeltoidea atau subacromialis dan ‘rotator cuff’ muscles (subscapular m, supraspinatus m, dan infraspinatus m), serta tendon long head biceps. Ketika abduction-elevation terjadi benturan antara head of humerus dg acromion, diantisipasi dg humerus external rotation dan atau scapular abduction dan penekanan jaringan isi suprahumeral Dibentuk oleh: Greater tuberosity of the humeral head, inferiorly Coracoid process, anteromedially Coracoacromialarch, superiorly 3. ACROMIOCLAVICULAR JOINT Merupakan plane joint: acromion konkaf menghadap ke medial dan clavicula konveks. Dalam klinis gerakan Elevation-Depression dan Protraction-Retraction Acromion konkaf: arthrokinematic saat elevation terjadi translasi acromion ke cranial dan saat depression translasi ke caudal. Saat protraction translasi ke ventral dan retraction translasi ke dorsal. Gerak Traction: selalu kearah lateral searah acromion ditarik. MLPP: posisi netral CPP: posisi protraction penuh. 4. STERNOCLAVICULAR JOINT Jenis Saddle joint: clavicula konkaf kearah anteroposterior dan konveks kearah craniocaudal. Gerak fisiologis spt AC Joint, gerak arthrokinematicnya saat elevation: caudal translation, saat depression: cranial translation, dan saat retraction: dorsal translation. Traction dg tarikan searah axis longit claviculae MLPP posisi netral CPP posisi protraction Dibentuk oleh: Articulation between the articular end of the clavicle, the clavicularnotch of the manubrium of the sternum, and the cartilage of the first rib 5. SCAPULOTHORACAL (JOINT) Bukan sendi sebenarnya, mrpk pertemuan antara scapula dg dinding thorax, bersama SC joint mrpk tempat bertumpunya extremitas atas terhadap tubuh. Dibatasi: subscapular m. dan serratus anterior m, stabilisasi oleh trapezius, rhomboideus major– minor, serratus anterior, dan levator scapula, Gerakan elevation–depression dan abduction– adduction sesuai dg arah translationnya. Gerak arthrokinematic Traction adalah gerak scapulae menjauh terhadap dinding thorax Secara fungsional bekerja seperti sendi, namun tidak memiliki karakteristik sendi synovial Tidak memiliki support ligamen Menumpu semata-mata pada otot-otot yang menyokong di antara skapula dan thoraks 6. INTERVERTEBRAL JOINTS Sendi intervertebral yg terlibat adalah cervical bawah (C6-7-Th1) dan thoracal atas (Th1-2-3-4) dmn saat gerak bahu flexion atau abdudtion penuh terjadi rotation kearah ipsilateral dan lateral flexion kontralateral. Tinjauan osteo- dan arthro kinematicnya dibahas dalam Cervical- dan thoracal-spine. 7. COSTOVERTEBRAL-TRANSVERSAL Costa 1 – 2 – 3 – 4 secara bertahap mengikuti gerak lengan seperti intervertebral joint dg winging dan rotation. Gerak osteokinematic dan arthrokinematicnya dibahas dlm thoracal spine. INNERVATION Persarafan shoulder complex oleh segment C(3), C4, C5, C6, C7, (C8-Th1), Area dermatome terbagi atas C3 (bag leher), C4 (bag pundak), C5 (bag deltoid sampai lateral lengan atas), C6 (dorsal lengan atas hingga lengan bawah), C7 (bag medial lengan atas dan bawah), C8-Th1 (lengan bawah hingga kelingking). Sarap perifer yang memelihara menurut area nervina terbagi atas (lihat gambar) Cabang saraf dari saraf sympathic segment C3 = Th 3, C4 = Th4 dan seterusnya Th8 oleh Th8 DAFTAR PUSTAKA Frankle and Nordin, Biomechanic, Churchill Livingstone, Eidinburgh, Ed. 4, 1998. Goodman, c.c. and Boissonault, W.G., Pathology, implication for the hpysical therapist, WB Saunders Co, Philadelphia, 1998. Hall, SJ, Basic biomechanic, Mc Graw Hill, Boston, 2003 Kapanji, IA. Physiology of joint Vol I Upper extremity, Churchill Livingstone, Eidinburgh, 1986. Rasch, PJ, Kinesiology, Lea and Febiger, Philadelphia, 1998