Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Polycomb Group Proteins and Cancer wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Heritability of IQ wikipedia , lookup
Y chromosome wikipedia , lookup
Genetic engineering wikipedia , lookup
History of genetic engineering wikipedia , lookup
X-inactivation wikipedia , lookup
Neocentromere wikipedia , lookup
Human genetic variation wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Population genetics wikipedia , lookup
Behavioural genetics wikipedia , lookup
Oncogenomics wikipedia , lookup
Designer baby wikipedia , lookup
Genetic testing wikipedia , lookup
Microevolution wikipedia , lookup
Public health genomics wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
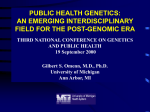
Newsletter for health care providers regarding services from the Human Genetics Laboratory at UNMC Remembering Warren Sanger, Our Leader by John Keenan, UNMC public relations Warren Sanger, Ph.D., director of the Human Genetics Laboratory and director of genetic medicine at the Munroe-Meyer Institute (MMI), died February 5th, 2015 at the age of 69. Board certified in clinical cytogenetics and PhD medical genetics, Dr. Sanger was a founding fellow of the American College of Medical Genetics and Genomics and the leader of our genetics laboratory for over 40 years. He was also a professor in the departments of pediatrics and pathology and microbiology and author or coauthor of almost 300 peer-reviewed publications. With the passing of Dr. Sanger, our laboratory team lost our beloved leader, and the genetics world lost a giant. But if Dr. Sanger’s stature in the world of genetics was imposing, you wouldn’t have known it by the way he ran his lab and his department – one of the reasons we will all miss him so much. “I think Warren can be best summed up in that every single person, no matter their station in life, called him Warren,” said Tanner Hagelstrom, Ph.D., the interim director of the lab. “He was not Dr. Sanger, famous scientist. He was Warren. He was a friend to everyone.” He believed in that personal touch not only for himself, but for the lab. “He believed strongly that clinical perspective was critically important to the interpretation of laboratory tests,” said genetic counselors Dani Bishay and Rachel Barbar. “Before many labs chose to do so, he added genetic counselors to the laboratory for this perspective. While colleagues knew that Warren was always a phone call away to answer clinical questions, he specifically trained us to do the same. We are happy to field clinical or testing questions for you and your patients.” Jennifer Sanmann, Ph.D., associate laboratory director, said the lab was a reflection of Warren’s vision, hard work, and compassionate soul. “Like so many of my colleagues, I was fortunate to call Warren both my mentor and my friend for more than a decade,” she said. “Committed to empowering his team, Warren has well-prepared us for the day when he is no longer just a few short steps down the hall with a cup of coffee, a welcoming smile, and words of gentle guidance. As we forge ahead without our beloved leader, know that we do so with the lessons that he taught us in tow: honesty, humility, compassion, and an unparalleled commitment to patient care.” That commitment showed in the way Warren “grew” the laboratory over more than 40 years – through personal visits and phone conversations, not pitches or persuasion, said marketing specialist Nikki Hackendahl. “That is a quality so unique amid a market of large commercial laboratories, budgets, and sales teams. While I cannot promise to embrace his love for fishing, moving forward I do extend his personal promise to provide you with individualized service.” UNMC Human Genetics Laboratory Newsletter | 2015 vol 1 New Look, Same Promise The University of Nebraska Medical Center (UNMC) recently released a new logo (see above). As part of the UNMC family, all of our laboratory materials will also adopt this look. These branding changes have been applied to most of our printed and online material; however, you may still see the old logo on things previously disseminated prior to the change, especially test collection kits and test request forms, during this time of transition. To ensure the most current information is available to your facility and patients, we encourage you to begin using materials containing the new logo. Please contact our marketing specialist if your facility is in need of printed materials, such as test request forms or patient brochures. Collection kits are currently being updated, but kits containing the old logo do not need to be replaced unless expired. Newsletter On behalf of our entire Human Genetics Laboratory team, we would like to personally thank you for putting your trust in our expertise. We promise to uphold what you have come to know and expect as Dr. Sanger’s “patient-first” commitment and welcome your feedback regarding how we can better meet the needs of you and your patients. 2015 volume 1 This Newsletter is produced by the Human Genetics Laboratory, part of the Munroe-Meyer Institute, at the University of Nebraska Medical Center. For additional printed copies, or other information, please contact: Nicole (Nikki) Hackendahl, BS Marketing Specialist 402-559-6935 | [email protected] UNMC Human Genetics Laboratory 985440 Nebraska Medical Center Omaha, NE 68498-5440 402.559.5070 [email protected] unmc.edu/geneticslab The Human Genetics Laboratory Team University of Nebraska Medical Center est. 1974 MISSION: To provide accurate and affordable genetic testing and interpretation for the patients we serve. Newsletter | 2 Laboratory Expands To Hereditary Cancer Testing Approximately 1 in 3 people in the United States will develop cancer in his or her lifetime.1 In order to identify genetic changes that are known to predispose a person to a particular type of cancer (and some other noncancerous conditions), our laboratory has developed 7 tissuespecific hereditary cancer panels. In most cases, cancer develops later AVAILABLE PANELS: -- Breast7 -- BreastIOvarianIUterine26 -- Colorectal20 -- EndocrineIParagangliomaPheochromocytoma17 in life in people without a significant Identifying a disease-causing family history of the disease. For these (pathogenic) change in any of the patients, the cancer is often thought to genes included in each panel provides -- Neuro17 be “sporadic” or to have developed by potentially actionable results, including chance over time. However, for a subset treatment and/or risk reduction. -- Pancreatic14 of patients, this is not the case. Rather, Additionally, this information allows these individuals develop cancer that is for the targeted genetic screening termed “hereditary” or is the result of of at-risk family members. a genetic change present since birth. Often, physicians and genetic counselors can use information from the patient’s personal and family history to determine if there is an increased likelihood that an individual’s cancer is hereditary. Factors that result in an increased likelihood of hereditary cancer include: • The type of cancer is rare. • Cancer presents at an early age. • Multiple family members have the same or related cancers. • Multiple cancers are present in the same person. Current literature suggests that both sequencing-based changes (changes at the DNA base pair level) and copy number changes (deletions or duplication within the gene of interest) have been identified in patients with hereditary cancers. Thus, to ensure comprehensive assessment of the genes of interest, each of our hereditary cancer panels includes two testing components: -- Renal19 A complete list of genes and testing indications for each of our panels, as well as logistical information (test request forms, specimen requirements, turnaround times), is available on our laboratory website. Additionally, if you or your team would like to learn more about how these panels would benefit your patients, please contact the laboratory to speak with a genetic counselor or director. sequencing analysis and high resolution deletion/duplication analysis. 1 “Lifetime Risk of Developing or Dying From Cancer,” October 1, 2014. http://www.cancer.org/cancer/cancerbasics/lifetime-probability-of-developing-or-dying-from-cancer Newsletter | 3 “Chromosome analysis is the foundation of our laboratory. Our team is dedicated to providing accurate and timely cytogenetic studies across all oncologic specimen types.” Chromosome Analysis: Clinical Utility Stands the Test of Time Chromosome Analysis (conventional cytogenetics) has been used by laboratories for decades for the identification of diagnostic and prognostic genetic markers in oncologic specimens, including bone marrow aspirates, peripheral blood specimens, lymph node biopsies, solid tumor tissues, and other body fluids. Chromosome analysis is also frequently referred to as G-banding because of the technique used to differentially stain (“band”) chromosomes for improved characterization. In the laboratory, our team analyzes the metaphase chromosomes Chris Higgins, BS, CG(ASCP)CM Cytogenetics Supervisor from cells of interest and organizes them into a karyotype that accompanies the final report (see image below). Chromosome analysis has many advantages. This technique is a whole genome approach, characterizing both numerical and structural abnormalities throughout all chromosomes. Unlike 48,XY,+8,t(9;22),i(17),+der(22) BONE MARROW KARYOTYPE more focused laboratory techniques such as fluorescence in situ hybridization (FISH), a specific aberration of interest does not need to be identified prior to analysis. Thus, chromosome analysis allows for the identification of hallmark abnormalities associated with a given diagnosis (e.g., a translocation between the long arms of chromosomes 11 and 14 in mantle cell lymphoma) as well as genetic abnormalities not anticipated based on the testing indication alone. Like a patient’s response to therapy. However, this technique ► ► other assays, chromosome analysis is useful in monitoring provides additional information about disease progression and treatment-related secondary malignancies that might not be ► apparent with a targeted genetic study (e.g., FISH alone). Of note, chromosome analysis is limited in its resolution as compared to most other genetic tests. Thus, for many indications, we recommend performing concurrent chromosome ► ► analysis and targeted FISH for the identification of clinicallyrelevant genetic changes. Our laboratory directors are eager to discuss our current oncology test menu and our recommended testing strategies with you at any time. In G-banded karyotype from a bone marrow aspirate showing three copies (trisomy) of chromosome 8, a translocation between chromosomes 9 and 22 t(9;22)(q34;q11.2) resulting in the presence of the Philadelphia chromosome, and an isochromosome 17 resulting in loss of the tumor suppressor gene TP53. This karyotype demonstrates the hallmark cytogenetic change observed in chronic myelogenous leukemia [t(9;22)], as well as common secondary abnormalities associated with this disease [+8, i(17), and +der(22)]. Newsletter | 4 addition, logistical information, including specimen requirements, turnaround times, and shipping details, is available on our laboratory website or by contacting our laboratory team. Decades of Committment The Human Genetics CYTOGENETICS SECTION FISH SECTION ADMINISTRATION Laboratory Supervisor: Laboratory Supervisor: Associate Directors: Christine Higgins, BS, CG(ASCP)CM 34 Pamela Althof, MS, CG(ASCP)CM 14 Bhavana Dave, PhD, FACMG 19 tremendous loss with the Culture Techs: Technologists: passing of Dr. Sanger, and Fen-Fen Lin, BS 19 Michele Wiggins, BA, CG(ASCP)CM 17 Laboratory Managers: Patricia Cattano, BA 18 Tom Hempel, BS, CG(ASCP)CM 14 Renée Fordyce Boyer, MS, CG(ASCP)CM 39 Yvette Rush, BS 13 Chestnut Livermore, BS, CG(ASCP)CM 11 Michelle Hess, MS, CG(ASCP)CM 35 Laboratory suffered a we will greatly miss his 40 years of experience our team of 66 members foundation that Warren MICROARRAY SECTION Technologists: Dianna Zaleski, BS, CG(ASCP)CM 28 proudly stands on the Administrative Associate: CONSTITUTIONAL STUDIES and leadership. However, Diane Pickering, MS, CG(ASCP)CM 26 LABORATORY SUPPORT Kirby Anderson, BS, CG(ASCP) 27 Technologists: Customer Support: Ivan Kanev Stoyanov, DVM, PhD, CG(ASCP)CM 15 Denae Golden, BS, CG(ASCP)CM 12 Francisca Rebolloso, BA, CG(ASCP)CM 35 Jadd Stevens, BA, BS, CG(ASCP)CMMBCM10 Billing Representative: Siri Huston, BA, CG(ASCP)CM 28 CM Abigail Haggerty, MS, CG(ASCP)CM 10 Lori Myers 25 MOLECULAR SECTION Technologists: Laboratory Supervisor: cumulative 828 years of Jana Brueggemann, BA, CG(ASCP)CM 18 Marilu Nelson, MS, CG(ASCP)CMMBCM 26 Jeff Pinnt, BS, CG(ASCP)CM 17 experience at UNMC. Melissa Nipper, BS, CG(ASCP) 14 Technologists: In addition, we would Amaris Zephyr Van Dyke, BS, CG(ASCP)12 like to recogize the 36 Kimberly Tyrey 20 Laboratory Supervisor: ONCOLOGY STUDIES built, bringing with us a Jennifer Sanmann, PhD, MB(ASCP)CMCGCM 10 CM Kimberly Wiechman, MS, CG(ASCP)CM 12 Kelli Novak, BS, CG(ASCP)10 Julie Carstens, MS, CG(ASCP)CMMBCM 29 Janet Williamson, BS, MLT, CG(ASCP)CMMBCM 11 Programer / Analyst: Rebecca Gilbert 20 Marketing Specialist: Nicole Hackendahl, BS 13 Office Associate: Kelly Crotty 12 Laboratory Assistant: Bunnita Washington, CMA 12 employees who each have 10 or more years of dedicated service. Panel Includes More Genes, Increasing Diagnostic Utility Our laboratory launched an expanded Autism / Intellectual Disability / Multiple Anomalies Panel in November 2014. The expansion of this panel from 86 genes to 117 genes allows for inclusion of several new non-syndromic autism genes (e.g., CHD8 ), as well as the addition of several genes associated with known genetic syndromes. The newly added genes broaden the scope of our panel to include Coffin-Siris, Greig cephalopolysyndactyly, Joubert, Pallister-Hall, Simpson-Golabi-Behmel, Sotoslike, and X-linked creatine deficiency syndromes. For the complete list of genes and disorders included in this panel, please visit our laboratory website. Newsletter | 5 The genetic changes that result in disease come in several different forms, including sequence-based mutations (changes in the DNA at the base-pair level) and intragenic deletions/duplication (copies number changes within the gene of interest). However, due to the current limitations of technology, both pieces of clinically-relevant information (sequencing and deletion/duplication) cannot be obtained from a single assay. Thus, the comprehensive panel option on our laboratory’s test request form includes both sequence analysis and high resolution deletion/duplication analysis of all 117 genes. Either test (sequencing or deletion/duplication) can be ordered separately on the test request form as well. We are pleased to offer this expanded panel at the same price and within the same reporting parameters as the previous, smaller version. Please contact any of the laboratory genetic counselors or directors if you have questions about how this expanded panel may benefit your patients. Human Genetics Laboratory 985440 Nebraska Medical Center Omaha, NE 68198-5440 402.559.5070 unmc.edu/geneticslab In this issue 1 Remembering Warren Sanger, Our Leader Dr. Warren Sanger, beloved director of our Human Genetics Laboratory, has passed away. Although this void is vast, we proudly promise to continue his legacy of dedicated patient care and personalized service. 3 Hereditary Cancer Testing Seven tissue-specific gene panels now available. 4 Chromosome Analysis for Oncology Historical technique remains clinically useful for diagnosis and prognosis. UNMC Human Genetics Laboratory Newsletter | 2015 vol 1 WILL YOU ATTEND THE 2015 ANNUAL ACMG MEETING? Visit booth 831 to meet our team! M A R C H 2 5 -2 7