Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
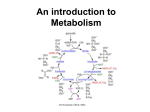
DIAGNOSIS AND TREATMENT OF BONE DISEASE IN RENAL FAILURE Dr.Shahram Sajjadieh Nephrologist The management of progression of CKD is aimed at addressing a multiplicity of factors known to be associated with progression. DIAGNOSIS AND TREATMENT OF BONE DISEASE IN RENAL FAILURE Dr.Shahram Sajjadieh Nephrologist CKD Metabolic Bone Disease All stages of chronic kidney disease (CKD) are associated with increased mortality; patients who require dialysis have a particularly poor prognosis. Without the benefits of a kidney transplant, 5-year survival for patients aged ~60 years who are on dialysis is only just better than 5-year survival for sufferers of ovarian carcinoma (46% versus 44%, respectively) and much worse than the 5-year survival for patients with breast or colon cancer Changes in bone mineral metabolism and alterations in calcium and phosphate homeostasis occur early in the course of CKD and progress as kidney function declines These changes are grouped under the umbrella term Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) which includes renal osteodystrophy and extraskeletal (vascular) calcification related to abnormalities of bone mineral metabolism Pathogenesis Kidney failure disrupts systemic calcium and phosphate homeostasis and affects the bone, GIT and parathyroid glands. In kidney failure there is decreased renal excretion of phosphate and diminished production of calcitriol (1,25-dihydroxyvitamin D) Calitriol increases serum calcium levels The increased phosphate and reduced calcium, feedback and lead to secondary hyperparathyroidism, metabolic bone disease, soft tissue calcifications and other metabolic abnormalities PO4 Ca GFR 1,25 DHCC Calcitriol PTH Although bone disease and abnormal PTH are a major feature, CVD and excess calcification (extra-skeletal) are important causes of morbidity and mortality Normal Bone Remodelling Cycle Resorption osteoclasts Quiescence Formation osteoblasts matrix Mineralisation Hyperparathyroidism Increase PTH is hallmark of secondary hyperparathyroidism The major factors leading to it’s increase are; Decreased production of Vit D3 (calcitriol) Decreased serum calcium Increased serum phosphorous Role of PTH Responsible for maintaining serum calcium in a narrow range (8.5-10.3) Does this by; 1. acting directly on the distal tubule of the kidney to increase calcium reabsorption – – Increases calcitriol production (D3) D3 increases GIT absorption of Ca and Phos and promotes osteoclast formation. 2. Acting on bone to increase calcium and phosphate efflux The net effect of PTH is to create positive calcium balance necessary to maintain homeostasis. To balance out the increased phos from skeletal effects, and GIT effects of calcitriol, PTH acts secondarily to increase renal phos excretion By decreasing activity of sodium phosphate co-transporter in prox renal tubule. Uremic Secondary Hyperparathyroidism Cause PO4 retention Low 1,25 Vit D synthesis Effects (late) Proximal weakness, Bone pain Alk Phos, bone erosions Rx Diet, PO4 binders Calcitriol, PTHx (usually for 3o) hyperPTH in CKD In CKD is a progressive disorder. Involves both increased secretion PTH & hyperplasia Can occur once eGFR < 60 PTH levels increase progressively as renal function declines and by CKD stage 5(<15) most pt’s expected to have this. Usually the 1st sign and occurs before lab tests pick up phosphatemia, ↓ Vit D3 and ↓ calcium Presumably as PTH is maintaining homeostasis. Unless treated, progresses and frequency of parathyroidectomy proportional to yrs on dialysis Classification of Bone Disease in CKD The circulating level of PTH is primary determinant of bone turnover in CKD Type of bone disease depends upon Age of pt Duration of kidney failure Severity of hyperPTH Type of dialysis PTH & Vit D receptors, as well as calcium sensors are present on osteoblasts Types of Renal Bone Disease Traditionally classified according to degree of abnormal bone turnover High Turnover (osteitis fibrosa) Hyperparathyroidism Low turnover Adynamic - Osteomalacia Beta 2 MG amyloidosis Osteoporosis Post-menopausal - Post-transplant High turn over bone disease Due to excess PTH Increased bone turnover activity (greater number of osteoclasts and osteoblasts) and defective mineralization. Associated with bone pain and increased risk of fractures. Severe symptomatic disease is currently uncommon with modern therapy. Mixed uremic bone disease Mixture of high turn over bone disease and osteomalacia Osteomalacia Formally linked to aluminium toxicity From aluminium based phosphate binders From contamination of water in diasylate solutions Adynamic bone disease Characterized by low osteoblastic activity and bone formation rates Seen in up to 40% HD and 50% PD May be due to excess suppression of the parathyroid gland with therapies, particularly calcium-containing phosphate binders and vitamin D analogues. Typically maintain a low serum intact PTH concentration, which is frequently accompanied by an elevated serum calcium level. Felt to represent a state of relative hypoparathyroidism Clinical manifestations of bone disease Most with CKD and mildly elevated PTH are asymptomatic When present classified as either 1. Musculoskeletal 2. Extra-skeletal Musculoskeletal Fractures, tendon rupture and bone pain from metabolic bone disease, muscular pain and weakness. Most clinically significant is hip fracture, seen in CKD 5 (and is associated with increase risk of death) In dialysis pts there is already a 4.4 x increase risk of hip fracture. Extra-skeletal Important to recognise disordered bone and mineral metabolism is a systemic disorder affecting soft tissues, particularly vessels, heart valves and skin. CVD accounts for around half of all deaths of dialysis patients. Coronary artery and vascular calcifications occur frequently in CKD 5 (and increase each year on dialysis) Types of calcification 1. Focal calcification associated with lipid laden atherosclerotic plaques • Increases fragility and risk of plaque rupture 2. Diffuse calcification • • • not in atherosclerotic plaques and occurs in media of vessels Called “Monckeberg’s sclerosis” Increases blood vessel stiffness and reduces vascular compliance ○ ○ ○ Results in widened pulse pressure Increased afterload LVH • Contributing to CVD morbidity Types of calcification Calciphylaxis or calcemic uremic arteriopathy Seen primarily in CKD 5 Occurs in 1-4% of dialysis patients Presents with extensive calcification of the skin, muscles and SC tissues. ○ Extensive medial calcification of small arteries, arterioles, capillaries and venules. ○ Clinically they may have skin nodules, skin firmness, eschars, livedo reticularis and painful hyperesthesia of the skin. ○ May lead to non healing ulcers and gangrene calciphylaxis A, Confluent calf plaques • (borders shown with arrows). Parts of the skin are erythematous, which is easily confused with simple cellulitis. B, Gross ulceration in the same patient 3 months later. The black eschar has been surgically débrided. C, Calciphylactic plaques, a few of which are beginning to ulcerate. (Photographs courtesy of Dr. Adrian Fine. Up To Date) Angulated black eschar with surrounding livedo. Note the bullous change at the inferior edge of the eschar. (courtesy Up To Date) Diagnosis of CKD bone disease Blood PTH ○ Random circulating PTH (1/2 life 2-4 mins) ○ Excreted renally so present for longer in RF Calcium Phosphate Bone biopsy no longer frequently performed Imaging In general not indicated PTH levels Normal (Pathwest) 0.7 – 7.0 pmol/L In CKD there is end-organ resistance Hence, recommended levels are 2 – 3 x normal. Treatment of CKD bone disease Directed towards normalizing serum calcium, phosphate and PTH, while minimizing the risks associated with Rx Treatment of CKD bone disease Various Rx for secondary hyperPTH and hyperphosphataemia include; 1. Dietary phosphorous restriction 2. Calcium and non-Ca phosphate binders 3. Calcitriol or other Vit D analogues 4. Calcimimetics 5. Parathyroidectomy Phosphorus (oxidized form is phosphate) 80% in the bone Food products include; nuts, beer, chocolate, coca-cola Normal level 0.8 – 1.5mmol/L (Pathwest) Passes into glomerular filtrate and 90% reabsorbed Reabsorption decreased by PTH and by calcitonin and increased if PTH is absent Low levels if hyperparathyroidism with excessive losses in urine High levels in hypoparathyroidism or renal failure Phosphate binders Calcium-based phosphate binders Calcium carbonate (Cal-Sup/Caltrate) Only Cal-Sup i PBS/S100 Varies, eg. 1 BD, 1-4 TDS Must be chewed with food to maximize binding of ingested phosphorous. Phosphate binders Non-calcium phos binder Sevelamer Often used in conjunction with Cal-sup Used when phos still high despite max Cal- Sup (2 TDS) More costly Phosphate binders Aluminium-containing phos binders Alu-tabs/aluminium hydroxide Most effective, but ceaesd use when sevelamer and cinacalcet available. Systemic absorption with subsequent neurological, hematological and bone toxicity. Calcitriol 1,25-(OH)2 Vitamin D3 or other analogues bind to receptor on PT tissue and suppress PTH production Calcimimetics Calcium receptor-sensing agonists Act on PT gland and increase sensitivity of receptor to calcium Cinacalcet (Sensipar) Significant decrease PTH, w/o Ca or phos Avoids calcification Parathyroidectomy Last option Considered when other methods fail to ↓ PTH Either total or sub-total Used to re-implant in forearm. We recommend measuring serum levels of calcium, phosphate, PTH, and alkaline phosphatase activity at least once in adults with GFR <45 mL/min/1.73 m2 in order to determine baseline values and inform prediction equations if used As kidney function declines abnormalities of serum calcium, phosphate and circulating hormones related to CKD-MBD progress. These include parathyroid hormone (PTH), 25hydroxyvitamin D (25(OH)D), 1,25-dihydroxyvitamin D (1,25(OH)2D), and other vitamin D metabolites, fibroblast growth factor-23 (FGF-23), and growth hormone. At the tissue level there is down regulation of vitamin D receptors and resistance to the actions of PTH. abnormalities of calcium and phosphate appear to occur relatively later in the course of CKD, than do abnormalities in values of 1,25 (OH) and 25 (OH) Vitamin D and PTH. Thus, the recommendation is to evaluate these parameters in relatively early stages of CKD, In dialysis patients the highest risks for mortality have been reported with combinations of high serum phosphate and calcium together with either high PTH or low PTH compared with the combination of high PTH with normal serum calcium and phosphate We suggest not to perform bone mineral density testing routinely in those with eGFR <60 mL/min/1.73 m2, as information may be misleading or unhelpful. bone densitometry does not reliably predict fracture risk in patients with GFR <60 mL/min/1.73 m2,neither does it predict the type of renal osteodystrophy. Thus, BMD measurements do not provide the information usually sought from such testing In people with GFR <60 mL/min/1.73 m2, we suggest maintaining serum phosphate concentrations in the normal range In people with GFR <60 mL/min/1.73 m2, the optimal PTH level is not known. We suggest that people with levels of intact PTH (iPTH) above the upper normal limit of the assay are first evaluated for hyperphosphatemia, hypocalcemia, and vitamin D deficiency Higher serum phosphate concentrations are associated with mortality and experimental data suggests that serum phosphate concentration is directly related to bone disease, vascular calcification and cardiovascular disease. earlier phosphate control may help reduce the early clinical consequences of CKD-MBD the risk of death increased 18% for every 1mg/dL increase in serum phosphate concentration There was no association seen with either PTH or serum calcium and all cause mortality Each 1 mg/dL increase in serum phosphate concentration was associated with a 21% ,33% .,25% ,and 62% greater prevalence of coronary artery, thoracic, aortic valve, and mitral valve calcification, Sources of dietary phosphate are proteinrich foods, including dairy products, meat, and fish as well as legumes, nuts, chocolates and inorganic phosphate additives such as are found in carbonated drinks. There are a number of agents available for phosphate binding In the absence of hypercalcemia there is no indication to prescribe phosphate-binders less cost effective than calcium-based agents. Current data are insufficient to make recommendations about target levels of serum calcium or PTH concentrations in people with CKD We suggest to not routinely prescribe vitamin D supplements, in the absence of documented deficiency, to suppress elevated PTH concentrations in people with CKD not on dialysis In the absence of deficiency treatment with vitamin D and related compounds has not been shown to improve either mortality or cardiovascular outcomes. Of particular note a higher urinary albumin creatinine ratio was associated with lower levels of 1,25(OH)2D at GFR values of <60 mL/min/1.73 m2. We suggest not to prescribe bisphosphonate treatment in people with GFR <30 mL/min/1.73 m2 their safety and efficacy below GFRs of 30 mL/min have not been well validated and intravenous bisphosphonates have been implicated in nephrotoxicity, especially when rapidly infused History Secondary hyperparathyroidism Patients with secondary hyperparathyroidism usually present with a history of underlying disease such as renal or intestinal conditions. Symptoms are musculoskeletal in nature, including bone pain, muscle weakness, and previous fracture. Physical Exam. Secondary hyperparathyroidism Skeletal deformity Decreased muscle tone Bone pain on palpation Short stature Medical Care For secondary hyperparathyroidism that occurs with chronic renal failure, parenteral administration of calcitriol is helpful; however, this manner of administration is feasible only for those patients receiving hemodialysis. For those individuals receiving therapy with peritoneal dialysis, oral administration of calcitriol is the only alternative. This route of administration may not be as effective as the intravenous route; however, some preliminary clinical trials have been conducted for calcimimetics in this condition, as well as in primary hyperparathyroidism. Early results are encouraging. Medical Care For other forms of secondary hyperparathyroidism, such as that resulting from chronic cholestatic liver disease, no standard treatment guidelines exist. Therefore, treatment should be aimed at ameliorating the underlying condition and supplying sufficient dietary calcium, phosphorus, vitamin D, and magnesium. This ensures that hyperparathyroidism is not exacerbated by nutritional insufficiency. over the past four decades it has been suggested that the accumulation of various ‘uremic toxins’ contribute to this increased mortality. urea parathyroid hormone (PTH) β2-microglobulin homocysteine leptin advanced glycation end products, asymmetric dimethylarginine and advanced oxidation protein products. phosphate Pathophysiology of hyperphosphatemia A normal diet contains ~1,500 mg per day of phosphate. However, modern practices of food processing frequently include the addition of sodium polyphosphates, and have appreciably increased this daily intake. Depending on individual food choices, phosphate intake can be increased by as much as 1,000 mg per day by increasing the percentage of processed foods in the diet. Pathophysiology... Serum levels of phosphate do not generally rise in patients with stage 3 CKD, as a result of compensatory reduction in tubular resorption mediated by increased serum levels of PTH, fibroblast growth factor 23 (FGF23) and phosphate itself. In patients with stage 4 and 5 CKD, the dietary intake of phosphate exceeds the excretion of phosphate (Figure 1), and serum levels of phosphate begin to rise to the point that hyperphosphatemia is usual in patients with advanced CKD. Pathophysiology... As intestinal phosphate absorption is linearly related to intake over the range 4–30 mg/kg per day the main determinants of absorption are the amount of phosphate present in the diet, its bioavailability and the presence or absence of natural dietary phosphate binders. Pathophysiology... Standard dialysis plus dietary restriction of phosphate are moderately effective control measures, but are unable to normalize serum levels in the majority of patients Consequently, oral phosphate-binding agents are generally required to bind phosphate in the gut lumen and thereby reduce its absorption. the only dialysis modality shown to normalize, or even deplete, serum levels of phosphate is DAILY, NOCTURNAL HOME HEMODIALYSIS, which is only practical for a small percentage of patients who are physically and psychologically able. Phosphate transport Following renal filtration, the majority of phosphate in the serum is reabsorbed across the kidney proximal tubule epithelium. Several humoral factors impinge on these transport systems to differing degrees to modulate the amount of phosphate that is reabsorbed. For example, FGF23 inhibits reabsorption of renal phosphate and decreases the synthesis of 1,25-dihydroxyvitamin D3. Clinical impact of hyperphosphatemia a statistical association between serum levels of phosphate and allcause (but not cardiovascular) mortality. the degree of hyperphosphatemia is statistically associated with vascular calcification, and vascular calcification is in turn associated with mortality. control of hyperphosphatemia in patients with stage 3–5D CKD is now regarded as a high priority and most patients on dialysis are eventually prescribed phosphate binders Pharmacology of oral phosphate binders All currently available oral phosphate binders work in a similar way—binding phosphate in the gastrointestinal tract, either by forming an insoluble complex or by binding it into a resin. In both cases less phosphate is available to be absorbed and more passes through the gastrointestinal tract to be excreted in the feces than when no phosphate binder is administered Aluminum salts these binders are highly effective but associated with cognitive disturbances, osteomalacia and anemia. Aluminum successfully reduces serum levels of phosphate via two mechanisms. First, aluminum ions in the gut form aluminum phosphate precipitates that are insoluble and cannot be absorbed. Second, aluminum hydroxide is able to form coordination compounds with phosphate ions and thus ‘trap and mask’ phosphate ions in the blood. No safe dose of aluminum has been identified. Aluminum salts an important tool in the treatment of hyperphosphatemia in most developing countries used as short-term ‘salvage’ therapy to achieve acute control of high levels of phosphate in most Western countries. sometimes used in patients whose prognosis is felt to be so short, because of other comorbidities a low dose of aluminum (2 g daily) probably does not cause toxicity in patients with a reduced life expectancy (such as patients aged >75 years receiving dialysis) Calcium and magnesium salts Binders that have a calcium or magnesium base bind phosphate ionically and are effective and inexpensive. Calcium carbonate and calcium acetate are the most widely used, but their administration results in hypercalcemia in up to 50% of patients, especially when coadministered with vitamin D analogues. Calcium and magnesium salts Calcium carbonate has a fairly long disintegration time and is not a particularly effective binder at low pH values because hydrogen ions compete with calcium for phosphate. Calcium carbonate dissociates best in an acid milieu and therefore a noteworthy problem with calcium carbonate is the opposing effects of pH on solubility and on the calcium–phosphate reaction—acidity is best for solubility, but alkalinity is best for binding. its performance as a phosphate binder can be inhibited by other medications such as gastric proton pump inhibitors. Calcium and magnesium salts Other binders that contain calcium but are much less widely used include calcium alginate (25% elemental calcium)and calcium lactate (12% elemental calcium). Calcium ketoglutarate is also reported to have phosphate-binding properties, without inducing notable hypercalcemia. Lanthanum carbonate Lanthanum carbonate retains binding activity across the full range of pH 1–7, but binds phosphate optimally at pH 3–5 Thus, lanthanum carbonate is able to bind phosphate efficiently in the low pH environment of the stomach, as well as at the higher pH values found in the duodenum and jejunum. Unlike calcium carbonate, lanthanum carbonate is highly insoluble and therefore has a low potential for accumulation, with only 0.001% of an oral dose being absorbed in the gastrointestinal tract, compared with 0.1% for aluminum. As expected for a minimally absorbed drug, the majority of an oral dose of lanthanum carbonate is excreted in the feces lanthanum does not seem to cross the blood–brain barrier and therefore the potential for neurological adverse events is extremely low. Sevelamer hydrochloride and carbonate Sevelamer (molecular weight 1016 Da) is a cationic hydrogel that is hydrophilic but insoluble in water Peak binding occurs in vitro in the physiological pH range (~pH 7) and is appreciably affected by changes in gastric acidity. sevelamer hydrochloride binds bile acids and reduces serum levels of LDL cholesterol at the expense of previously bound phosphate ions, which are released. Sevelamer hydrochloride, therefore, might also bind lipophilic drugs, such as immunosuppressants and the fat-soluble vitamins D, E and K. Reduced levels of 25-hydroxyvitamin D have been reported in a 12-month study in healthy volunteers. Sevelamer hydrochloride and carbonate evelamSer had little effect on ciclosporin levels, but further studies looking at the metabolites of ciclosporin demonstrated that the area under the curve and peak concentration of one of the metabolites, were significantly reduced by approximately 30% and 25%, respectively, 4 days after commencing sevelamer treatment. concomitant administration of sevelamer hydrochloride and mycophenolate mofetil reduced the immunosuppressant’s area under the curve by 25% even after a single dose. Sevelamer hydrochloride and carbonate Sevelamer carbonate has a similar structure to sevelamer hydrochloride. Both are marketed as 800 mg tablets, but a powdered form of sevelamer carbonate is also available in many countries in foil packets containing 800 mg or 2,400 mg. Apart from the absence of induction of metabolic acidosis, sevelamer carbonate seems to be equivalent to sevelamer hydrochloride in terms of efficacy and tolerability. Efficacy of oral phosphate binders traditionally efficacy has been judged simply by the criterion of serum levels of phosphate. with phosphate binders was independently associated with decreased mortality compared with no treatment, but the results were independent of baseline and follow-up serum levels of phosphate lack of correlation with serum levels of phosphate, might be attributable to an effect on circulating levels of FGF23 Efficacy of oral phosphate binders all phosphate binders decreased serum levels of phosphate compared with placebo. calcium salts were superior to sevelamer for reduction of serum levels of phosphate. Compared with calcium salts, however, sevelamer and lanthanum carbonate were associated with considerably reduced rates of hypercalcemia, which might result in decreased vascular calcification. increased PTH suppression by treatment with calcium salts compared with sevelamer Patient preference for phosphate binders Phosphate binders have to be taken with food, and their interference with an individual’s lifestyle and social habits is known to affect treatment concordance. all phosphate binders are of similar efficacy, and none is ideal. the choice of binder will depend to some extent on the prescriber’s and the patient’s individual habits and behavior as well as their expectations, beliefs and preferences. Safety and tolerability Gastrointestinal adverse events and tablet burden are the main tolerability issues that are common to all currently available oral phosphate binders. no statistically significant difference in the risk of gastrointestinal adverse events with calcium acetate compared with calcium carbonate, or with lanthanum carbonate compared with placebo or calcium carbonate. However, sevelamer was associated with an increased risk of gastrointestinal adverse events compared with calcium salts Calcium salts calcium overload might contribute to vascular calcification in patients with advanced CKD or on dialysis continues to accumulate. The KDIGO Clinical Practice Guidelines recommend restricting the dose of calcium-based phosphate binders in patients on dialysis in the presence of persistent or recurrent hypercalcemia, and in patients with arterial calcification and/or adynamic bone disease and/or if serum levels of PTH are persistently low, but the extent to which doses should be restricted is not specified. Magnesium salts Magnesium-containing phosphate binders are associated with raised serum levels of magnesium and diarrhea. A combination of calcium acetate and magnesium carbonate is available under the trade name OsvaRen®. OsvaRen® was equivalent to sevelamer in lowering serum levels of phosphate.A small increase in total serum calcium and no change in ionized calcium were reported. OsvaRen® was associated with an asymptomatic increase in serum levels of magnesium, but had a good tolerability profile. Lanthanum carbonate Avoidance of hypercalcemia is the major advantage cited for use of both lanthanum and sevelamer trace deposition of lanthanum occurred in some tissues, particularly in the liver, and tissue levels seemed to be increased under uremic conditions. a satisfactory long-term safety profile, with no evidence of harmful adverse events. Subsequent studies have demonstrated the absence of adverse effects on liver function, bone and the central nervous system. Sevelamer hydrochloride and carbonate the most important of its is association with metabolic acidosis. sevelamer’s amine content causing a dietary acid overload, and also the withdrawal of other phosphate-binding agents, which are often alkalinizing agents such as carbonates and acetates. Apart from the absence of induction of metabolic acidosis, sevelamer carbonate seems to be equivalent to sevelamer hydrochloride in terms of safety and tolerability. Sevelamer hydrochloride and carbonate Isolated cases of fecal impaction, ileus, bowel obstruction and perforation have been reported with sevelamer, possibly attributable to the large increase in the size of the tablet as the sevelamer molecules hydrate in the gastrointestinal tract Sevelamer binds various other molecules apart from phosphate, including folic acid (which results in a rise in levels of homocysteine) and vitamin D. In vitro, sevelamer binds vitamins C and K as well as copper and zinc. Alternatives to current phosphate binders Nicotinamide:inhibit sodium-dependent phosphate cotransport activity in the rat small intestine. The nicotinamide had no effect on serum levels of calcium, and resulted in a possibly beneficial rise in serum levels of HDL cholesterol plus a fall in levels of LDL cholesterol. Gastrointestinal adverse events will probably limit the dosage of nicotinamide to between 1 g per day and 2 g per day, and doses above 3 g per day are associated with hepatoxicity. Thanks for your attention






























































































![Poster ECE`14 PsedohipoPTH [Modo de compatibilidad]](http://s1.studyres.com/store/data/007957322_1-13955f29e92676d795b568b8e6827da6-150x150.png)