Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Alterations in Fluid,
Electrolyte and Acid-Base
Balance in Children
Dr. Nataliya Haliyash, MD, BSN
Institute of Nursing, TSMU
Pediatric Differences
• ECF/ICF ratio varies with age
• Neonates and infants have
proportionately larger ECF volume
• Infants: high daily fluid requirement
with little fluid reserve; this makes the
infant vulnerable to dehydration.
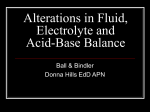
FIGURE 23–2
The newborn and infant have a high percentage of body weight
comprised of water, especially extracellular fluid, which is lost from the body easily. Note the
small stomach size which limits ability to rehydrate quickly.
Jane W. Ball and Ruth C. Bindler
Child Health Nursing: Partnering with Children & Families
© 2006 by Pearson Education, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Fluid Loss; Infants and <2yr.
• excretion is via the urine, feces, lungs and
skin
• have greater daily fluid loss than older child
• more dependent upon adequate intake
• greater about of skin surface (BSA),
therefore greater insensible loss.
• respiratory and metabolic rates are higher
• therefore, dehydrate more rapidly
Mechanism to Restore balance
• kidney: conserves water, regulates
electrolyte excretion
• <2yr kidneys immature
• less able to conserve or excrete water and
solutes effectively
• greater risk for acid/base imbalances
• Will use the SG norm: 1.005-1.015
Fluid Volume Imbalances
• Dehydration: loss of ECF fluid and sodium.
• Caused by: vomiting, diarrhea, hemorrhage, burns, NG
suctioning and drainage loss, adrenal insufficiency.
• Manifested by wt loss, poor skin turgor, dry mucous
memb., VS changes, sunken fontanel
• Dehydration that is not corrected will lead to hypovolemic
shock and death.
• Fluid overload: excess ECF fluid and excess
interstitial fluid volume with edema.
• Causes: fluid overload, CHF.
• Manifested by wt.gain, puffy face and extremities,
enlarged liver.
Clinical Manifestations of
Dehydration
Depend on the degree of dehydration.
• Weight loss
• Rapid-thready pulse
• Hypotension
• Decreased peripheral circulation
• Decreased urinary output
• Increased specific gravity
• decreased skin turgor
• dry mucous membranes
• absence of tears
• a sunken fontanel in infants.
Nursing Considerations
• How can the nurse determine if the
child is mildly dehydrated vs moderately
dehydrated?
Mild Dehydration: by history.
• hard to detect because the child may be alert,
have moist mucous membranes and normal
skin turgor.
• Wt loss may be up to 5% of body weight.
• The infant might be irritable; the older child
might be thirsty
• vital signs will probably be normal
• Capillary refill will most likely be normal
• Urine output may be normal or sl less
Moderate Dehydration
• dry mucous membranes; delayed cap refill
>2 sec; Wt loss 6-9% of body weight
• irritable, lethargic, unable to play, restless
• decreased urinary output: <1ml/kg/hr; dark
urine with SG > 1.015 (in child >2yr)
• Sunken fontanel
• HR increased, BP decreased. Postural vital
signs
Severe Dehydration
• wt loss > 10% body weight
• lethargic/comatose
• rapid weak pulse with BP low or
undetectable; RR variable and labored.
• dry mucous membranes/parched;
sunken fontanel
• decr or absent urinary output.
• Cap refill >4sec
Types of Dehydration and Sodium
Loss
• Sodium may be:
• Low
• High
• Or normal
Isotonic Dehydration or
Isonatremic Dehydration
• Loss of sodium and water are in proportion
• Most of fluid lost is from extracellular
component
• Serum sodium is normal (130-150mEq/L)
Harriet Lane Handbook, 2000.
• Most practitioners consider below 135 and above
148 a more conservative parameter (138-148)
• Most common form of dehydration in young
children from vomiting and diarrhea.
Hypotonic or Hyponatremic
Dehydration
• Greater loss of sodium than water
• Serum sodium below normal
• Compensatory shift of fluids from
extracellular to intracellular makes
extracellular dehydration worse.
• Caused by severe and prolonged vomiting
and diarrhea, burns, renal disease. Also by
treatment of dehydration with IV fluids
without electrolytes.
Hypertonic or Hypernatremic
Dehydration
• Greater loss of water than sodium
• Serum sodium is elevated
• Compensatory shift from intracellular to
extracellular which masks the severity
of water loss (dehydration) delaying
signs and symptoms until condition is
quite serious.
• Caused by concentrated IV fluids or
tube feedings.
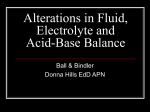
Clinical Manifestations Associated
with Degree of Dehydration
Dehydrated child
• Before…
and after treatment
Nursing Diagnoses
• Nursing diagnoses appropriate for a child with
dehydration may include:
1. Deficient fluid volume related to excessive fluid
volume loss or inadequate fluid intake.
2. Risk for injury (fall) related to orthostatic
(postural) hypotension.
3 . Deficient knowledge (caregiver) related to lack of
exposure to information about
preventing/detecting dehydration.
Outcome Identification
1. The child will receive sufficient fluids to replace
losses.
2. The child will exhibit signs of adequate hydration.
3. The child will not fall or sustain other injuries
while hypotensive or lethargic.
4. Caregivers will demonstrate understanding of
conditions that can lead to dehydration and of the
early signs and symptoms.
Planning/Implementation
• Nursing interventions include:
• assessment of daily weight, vital signs, and maintenance of
accurate intake and output records.
• Blood may be drawn to assess electrolytes, BUN and
Creatinine levels
• administration of oral or IV fluids.
• Injury due to falls can be prevented by making sure that the
side rails of the bed are raised, assessing level of
consciousness, and monitoring the serum sodium level.
• An elevation in serum sodium will cause the brain cells to
dehydrate and result in a loss of consciousness if not
corrected quickly.
Diarrhea
•is increase in the number of stools
and/or a decrease in their consistency
as a result of malabsorption or
alterations of water and electrolyte
transport by the alimentary tract.
•Diarrhea may be acute or chronic.
Grades of diarrhea
• Mild diarrhea – 4 to 7 loose stools each day as a
rule without other evidence of illness
• Moderate diarrhea – 8 to 15 loose or watery
stooles daily with elevated temperature,
vomiting, irritability, mild dehydration
• Severe diarrhea – numerous (>15) to
continuous stools, evident signs of moderate to
severe dehydration, drawn, flaccid expression,
high pitched cry, irritable or lethargic or even
comatose.
Acute gastroenteritis
•is characterized by the passage of ≥3 loose
or watery stools in an 24 hour period, or the
passage of one or more bloody stools, with
or without vomiting, nausea, fever, and
abdominal pain.
•Acute gastroenteritis usually refers to as an
illness lasting no longer than 10-14 days.
Etiology of acute diarrhea
Viral agents
Human rotavirus
Small round viruses:
Norwalk
Taunton
Snow Mountain
Astrovirus
Wollan
Enteric adenoviruses
Coronaviruses
Bacterial pathogens
Escherichia coli
Campylobacter
Salmonella
Shigella
Vibrio cholera
Yersinia enterocolitica
Clostridium difficile
Parasitic pathogens
Protozoa:
Giardia lamblia
Cryptosporidium
Entamoeba histolytica
Balantidium coli
Helmintic pathogens
Nematodes:
Ancylostoma duodenale
Strongyloides stercoralis
Necator americanus
Trichuris trichiura
Trematodes:
Schistosoma
Cestodes:
Taenia solium
Taenia saginata
Diphyllobothrium latum
Pathogenesis of Acute
Diarrhea
•
•
Diarrhea results when the net intestinal fecal
loss of fluid and salt exceeds the absorbed
amount.
There are 5 pathogenic forms of diarrhea:
1.
2.
3.
4.
5.
Toxigenic diarrhea
Osmotic diarrhea
Secretory diarrhea
Invasive diarrhea
Motility disorders
Toxigenic diarrhea
• Toxins from bacteria, like enterotoxigenic E.coli or
Vibrio cholerae, bind to specific receptors:
labile toxin (LT) raises the level of cyclic guanosine
monophosphate (cGMP) in the intestinal mucosa,
stable toxin (ST) increases the adenasine 3׳:5׳-cyclic
monophosphate (cAMP)
• This leads to blocking the absorption of Na and Clˉ
ions into the villous enterocytes.
• LT induce the secretion of Clˉ and HCO3ˉ ions by
crypt cells.
Osmotic diarrhea
• Characterized by a positive osmotic gap
of the stool
• Clinically, osmotic diarrhea is
distinguished by the fact that the
diarrhea diminishes when the patient
fasts or stops eating the poorly ingested
solute.
Differential diagnosis of
osmotic and secretory diarrhea
Stools
Osmotic diarrhea
Secretory diarrhea
Electrolytes
Na<70 mEq/l
Na>70 mEq/l
Osmolality
>(Na + K)2
=(Na + K)2
pH
<5
>6
Reducing
substances
Positive
Negative
Volume
< 200 ml/day
> 200 ml/day
Secretory diarrhea
• There is no positive osmotic gap and the stool
osmolality is equal to the ionic constituents:
(Na + K)2 = stool osmolality
• Food ingestion does not usually affect the stool
volume
• The stool is watery without blood or pus and is
characterized by very high volume and ion
output
Invasive diarrhea
• Is caused by direct mucosal damage by
the invasive organism
• It is similar to colitis and is usually
associated with blood and mucous.
Motility disorders
• Hypermotility can cause diarrhea by
reduction of contact time between
intestinal mucosa and its contents,
despite normal absorption function of
the cell
• Hypomotility can be primary, as in
idiopathic intestinal pseudo-obstruction
syndrome, or secondary to neuronal
disorders.
Clinical characteristics of infectious
gastroenteritis in dependence on
enteropathologic cause.
Organism
Rotavirus
Incubation
period:2-3 d.
Norwalk-like
viruses
Inc.period:
1-2 days
Characteristics
Abrupt onset
Fever (≥ 38°C) for
48 hh
Associated upper
resp.tract infection
Fever
Loss of appetite
Nausea/vomiting
Abdominal pain
Malaise
Comments
Incidence higher in
cool weather
6- to 24-month-old
infants are more
vulnerable
Source of infection:
drinking water, food
Affects all ages
Self-limited
Pathogenic
Escherichia coli
Incubation
period: highly
variable
Salmonella
groups
(nontyphoidae)
– gramnegative, nonencapsulated,
nonsporulating
Incubation
period: 6 hh-21
day
Diarrhea with moistgreen, watery stool with
mucus; becomes explosive
Vomiting may be present
from onset
Abdominal distension
Fever, intoxication
Rapid onset
Variable symptoms – mild
to severe
Nausea, vomiting, and
colicky abdominal pain
followed by diarrhea,
occasionally with blood and
mucus
Infants may be afebrile
and nontoxic
•Incidence
higher
in summer
•Usually
interpersonal
transmission, but
may transmit via
inanimate objects
•Highest incidence
in children
younger than 9
years, especially
infants
•Transmission –
via contaminated
food and drink,
more commonly
poultry and eggs
Shigella groups – Onset usually abrupt
Fever (to 40.5°C) and
gram-negative,
cramping abdominal pain
nonmotile,
initially
anaerobic bacilli
Febrile convulsions in 10 %
Incubation
cases
period: 1-7 days Headache, neck rigidity,
Vibrio cholerae
groups
Inc.period: 1-3
days
delirium
Sudden onset of profuse,
watery diarrhea without
cramping, tenesmus, or anal
irritation
Stools are intermittemt at
first, then almost continuous
Stools are whitish, almost
clear, with flecks of mucus –
“rice water stools”
Transmitted
directly or
indirectly
from infected
persons
Rare in
infants
Mortality is
high
Transmitted
via
contaminated
food or water
Food poisoning:
Staphylococcus
Nausea,vomiting
Incub.period:
4-6 hours
Botulism
Clostridium
botulinum
Incub.period:
12 hr – 3 days
•Transfered via
contaminated food –
Severe abdominal
inadequately cooked:
cramps
custards, mayonnaise,
Profuse diarrhea
cream-filled desserts
Shock may occur in
•Self-limited (24-72
severe cases
hours)
May be a mild fever
•Exellent prognosis
Nausea,vomiting
Transfered via
contaminated food
Diarrhea
Variable severity – mild
CNS symptoms
symptoms to rapidly
with curare-like
fatal within a few hours
effect
Antitoxin administration
Dry mouth,
dysphagia
Diagnosis
• Diagnosis is based on:
• the history, physical exam, and laboratory studies
focused on evaluating the child's hydration status
and identifying the causative agent.
• The history should include the following data:
•
•
•
•
•
Recent exposure to infectious agents
Travel history
Exposure to contaminated food and water supplies
Exposure to turtles
Attendance at a day-care center
If no systemic manifestations are
present:
• Diagnostic laboratory tests are not
indicated.
• Stool cultures should be performed for:
• children with a fever lasting more than 24
hours,
• blood or mucus in the stool,
• a family or household member with similar
symptoms,
• or a positive stool white blood cell stain.
Treatment
The main treatment aims are:
• To prevent dehydration – restoration
and maintenance of adequate hydration
and electrolyte balance.
• Nutritional support, adequate to prevent
protracted diarrhea and malnutrition.
What about antimicrobial
therapy?
• In about 30 % of patients no specific agent can
be found
• Most of the isolated pathogenic organisms are viral
• The majority of the bacterial pathogens are selflimited
• In some cases, antimicrobial therapy prolongs the
infection duration
• Antibiotic therapy has no effect on fluid transport
nor on nutritional support
When should antibiotics be
used?
•
•
•
•
In young infants
In immunocompromised patients
When a systemic bacteremia is suspected.
In case of specific persisting infection
caused by Yersinia, Campylobacter, and
Giardia
Rehydration
• In the majority of cases of acute diarrhea with
mild or moderate dehydration, this aim can be
achieved with oral rehydration solutions (ORS)
• 1-3 tsp of ORS every 10-15min to start (even if vomits
some)
• 50ml/Kg/Hr is the goal for rehydration.
• Severe dehydration requires immediate admission
to hospital and intravenous replacement of fluid
and electrolytes.
The rationale for the use of
ORS
1. During diarrhea, the normal
mechanism for water and sodium
absorption is impaired, so, the
replacement of water or saline fluids
alone will only lead to more diarrhea.
2. The sodium-glucose-coupled transport
generally remains intact. This
mechanism stimulates water transport
by solvent drag.
The basic components of ORS
• Glucose
• Electrolytes
in an isotonic solution.
In the World Health Organization formula
the glucose concentration is 2 %.
WHO recommendations for a
sodium concentration
• 90 mEq/l, essentially for treatment of cholera
• 30-60 mEq/l for countries, where cholera is
not a concern and the stool sodium
concentration in diarrheal illness is much
lower
• 30-40 mmol/l for neonates up to 2 mo
whose kidneys have less capacity to excrete
excess amounts of fluid and salt
Rehydration Fluids
• The World Health Organization recommends the
following electrolyte concentrations for rehydration
fluids:
•
•
•
•
•
20 g glucose/L,
90 mEq sodium/L,
80 mEq chloride/L,
20 mEq potassium/L,
and 30 mEq bicarbonate/L.
• Encourage caregivers to look at product labels and
make sure that the rehydration fluid they are
choosing has the above electrolyte concentrations.
Composition of oral electrolyte
solutions (in mEq/l)
Na+
K+
Clˉ
Other anion
CHO(%)
WHO solution
90
20
80
30
2
Gastrolyte
90
20
80
30
2
Pedialyte
45
20
35
30
2.5
Rehydralyte
75
20
65
30
2.5
infalyte
50
20
40
30
2
Composition of
“clear liquid” solutions
Na+
K+
CHO(%)
Pepsi Cola
1-2
0.1
10.9
Coca Cola
1-2
0.1
10
Root beer
6
0.6
10.6
Super-ORS
• Recent studies demonstrate the advantage of
short glucose polymers as the carbohydrate
source in ORS
• Traditionally it is widely used rice water + 3-5 %
sugar syrup.
• Or carrot decoction: 500 g of cleansed carrot boil
in 1 l of water during 1 hour, then mash it to
homogenous mass and add boiled water up to 1 l.
Boil for 10 min. Add 3 tsf of lemon juice. Give 1-2
teaspoon every 5-10 min up to 400 ml/day.
Why are drinks high in glucose
avoided during rehydration?
• Simple sugars increases the osmotic
effect in the intestine by pulling water
into the colon, thereby increasing
diarrhea and subsequent
fluid/electrolyte loss
• Drinks high in glucose: apple juice,
sodas, jello water.
Recommended foods during
rehydration progression:
• In this question opinions differ: “bowel
rest” versus “early feeding” is still
controversial.
• Generally, formula feeding should be
introduced gradually by starting with
dilute mixtures.
• In practice, refeeding can start gradually after 24
hr of only fluid intake, i.e.,”bowel rest”.
• An exception is made for nursing infants, who
should continue their regular feeding.
• Children already on solid foods are easier to
handle. Food with a high content of disaccharides
and monosaccharides (fruits, sweets) should be
withheld in the convalescent period.
• Foods with starch carbohydrates (cereal, rice,
noodles, bananas, potatoes, carrot, cooked fruits &
vegetables), soups, yogurt should be encouraged.
• It is important to give often small food-intakes (up
to 8-10 times per day)
IV Therapy
• Used for severe dehydration or in the child
who will not/cannot tolerate ORS
• Half 24hr maintenance plus replacement
given within first 6-8hr (in ER) to rapidly
expand the intravascular space. Usually a
normal saline bolus.
• slower IV rate for the remainder of the first
24hrs
• nurse records IV vol infused hourly
Rehydration and IV solution
• Why is the child initially rehydrated with
a normal saline bolus and not an IV
solution with potassium?
• Potassium is only added to an IV after
the patient has voided to avoid
hyperkalemia in a child with little or no
urinary output
Adding Potassium to Intravenous
Solutions
• Be sure that the child is able to void (1 -2 ml/kg/hr) before
adding potassium to the IV.
• Children who are dehydrated are oliguric and can become
anuric. An anuric child will not be able to excrete electrolytes
that are in the IV solution; therefore, if potassium is added to
the IV, it would result in an elevated serum potassium. An
elevated serum potassium can cause cardiac irritability and
ventricular fibrillation.
• Always check the dose and dosage calculations prior to
giving. Never give more than 40 mEq/L at a rate not to
exceed 1 mEq/kg/hr.
• After adding potassium to an IV bag, shake it to make sure
the potassium is equally distributed.
• Never give potassium by IV push.
Which of the following IV
solutions replaces Sodium?
•
•
•
•
D5 W
Lactated Ringers
Normal Saline
D5 ½ NS
• Answer: All but D5 W
Calculation of intravenous fluid
needs: maintenance
• For the 1st 10 Kg, replace at 100ml/Kg
• for the second 10 Kg, replace at
50ml/Kg
• for >20kg, replace at 20ml/Kg
Example of Maintenance Fluid
Calculation
• Your patient is a 10 yr old weighing 35 Kg.
You want to determine this patient’s 24hr
maintenance fluid needs:
• for the first 10 Kg give 100ml/Kg = 1000ml
• for the second 10 Kg:
50ml/Kg = 500ml
• for the remaining 15 Kg (35-20Kg) , replace
at 20 ml/Kg:
20 15 = 300ml
• 1000 + 500 + 300= 1800 ml/day.
How much fluid should this patient
get per hour?
• 1800 ml / 24 hrs = 75 ml/hr.
• Therefore, if the patient was NPO and not
taking in fluids from any other source, the IV
should be running at 75ml/hr.
• If there is a deficit that also needs to be
replaced, the IV rate may be slightly higher for
a defined period of time.
• If the patient is receiving fluids from other
sources, these need to be accounted as well
Practice Problems for Calculating
24hr Fluid Maintenance and the hourly
IV rate for:
• A 9 yr old patient who weighs 20 Kg.
• A 6 mo old baby who weighs 8 Kg
• An 24mo old toddler who weighs 18 Kg
• A 3 yr old preschooler who weighs 28 Kg
• An 18 yr old who weighs 50 Kg
Answers for 24hr Fluid Calc.
•
•
•
•
•
•
9yr old wt 20 Kg = 1500 ml/day
6mo old wt 8Kg= 800 ml/day
36mo old wt 18 Kg= 1400 ml/day
3yr old wt 28Kg=1660 ml/day
18yr old wt 50Kg= 2100 ml/day
Adult > 50Kg= 2-3 L/day
Fluid Overload:Edema
• capillary blood flow: inflammation, infection
• venous congestion: ECF excess, R sided heart
failure, muscle paralysis.
• albumin excess: Nephrotic Syndrome
• albumin synthesis: Kwashiorkor, liver cirrhosis
• capillary permeability: inflam/ burns
• blocked lymphatic drainage: tumors/surg.
Clinical Assessment /
Management of Edema
• assess dependent limbs if ambu or sacrum if lying
• ascites; periorbital edema; rings too tight
• pitting edema for degree of swelling
• daily wt and strictly In and Out
• elevation/change position Q2hr/ protect skin against
breakdown
• distraction to deal with discomfort and limitations of
edema.
Electrolyte Imbalances
• Electrolytes usually gained and lost in
relatively equal amounts to maintain
balance
• Imbalance caused by:
• Abnormal route of loss (vomiting/diarrhea)
can disturb electrolyte balance
• Disproportionate IV supplementation
• Disease states: renal dis.
Hypernatremia
• Excess serum sodium in relation to water
• Causes:
•
•
•
•
•
•
•
Too concentrated infant formula
Not enough water intake
Clinical manif.: thirst, lethargy, confusion
Seizures occur when rapid or is severe.
SG concentrated 1.020-1.030
Lab test: serum sodium
Treatment: hypotonic IV solution
Hyponatremia
• Excess water in relation to serum sodium
• Most common sodium imbalance in
children
• Causes:
• Infants vulnerable to water intoxication:dilute
form, excess pool water, poorly developed
thirst mech so cont to drink and can’t excrete
excess water.
Hyponatremia (cont)
• Clinical manif: decreased level of
consciousness d/t swelling of brain cells.
• Anorexia, headache, muscle weakness,
decreased DTR’s, lethargy, confusion or coma.
• Seizures occur when rapid or severe.
• SG dilute: 1.000-1.0005
• Lab tests: serum sodium
• Treatment: hypertonic solution.
Hyperkalemia
• Excess serum potassium
• Causes:
• excess K intake from IV overload, blood
transfusion, rapid cell death (hemolytic
crisis, large tumor destruction from chemo
rx, massive trauma, metabolic acidosis
from prolonged diarrhea and in DM when
insulin levels are low
• Insulin drives K back into the cells
• decreased K loss from Renal insufficiency
Hyperkalemia (cont)
• Clinical manif: all are related to muscle dysfunction:
hyperactivitiy of GI smooth muscle: intestinal cramping and
diarrhea.
• Weak skeletal muscles
• Lethargy
• Cardiac arrhythmias (tachycardia, prolonged QRS, peaked T
waves: also AV block and VTach).
• Lab test: serum potassium
• Treatment: correct underlying condition (take K out of the IV)
• dialysis (peritoneal or hemo), Kayexalate (po or enema), K
wasting diuretics, IV calcium, bicarbonate, insulin and glucose.
• Low potassium diet.
Hypokalemia
• Decreased serum potassium
• Causes: diarrhea and vomiting, ingestion of
large amts black licorice, diuretics, osmotic
diuresis (glucose in urine as in DM), NPO
without K replacement in IV, NG Sx, bulimia,
insulin.
• Also in nephrotic syndrome, cirrhosis, Cushing
Syndrome, CHF (to be covered elsewhere)
Hypokalemia (cont)
• Clinical manif: muscle dysfunction
• Slowed GI smooth muscle resulting in
abdominal distention, constipation and
paralytic ileus
• Skeletal muscles are weak; may effect
respiratory muscles
• Cardiac arrhythmias: hypokalemia potentiates
Digitoxin Toxicity.
• Lab test: serum potassium
• Treatment: oral and/or IV potassium, diet rich
in K.
Hypercalcemia
• Excess calcium
• Needs vit D for efficient absorption; most of Ca
is stored in the bones.
• Causes: bone tumors that cause bone
destruction, chemo rx release Ca from the
bones; immobilization causes loss from the
bones (usually excreted) but if kidneys can’t
clear it, hypercalcemia results, increased intake
(milk-alkali syndrome).
Hypercalcemia (cont)
• Clinical manif: Ca imbalances alter
neuromuscular irritability with non-specific
symptoms
• Constipation, anorexia, N/V, fatigue, skeletal
muscle weakness, confusion, lethargy.
• Renal calculi, cardiac arrhythmias
• HyperCa increases Na and K excretion leading to
polyuria and polydipsia.
• Rx: serum Ca, Ionized Ca, fluids, Lasix, steroids,
dialysis.
Hypocalcemia
• Decreased serum calcium
• Causes: decreased intake of Ca and/or Vit D
(adolescents are vulnerable d/t fad diets and the
deficit cannot be made up later, increasing risk
for osteoporosis).
• Limited exposure to sunlight, premature infants and
dark skinned people at increased risk to inadeq. Vit D
and therefore decreased Ca absorption.
• Parathyroid dysfunction, multiple transfusion (Citrate
binds Calcium), steatorrhea (as in pancreatitis and
Cystic Fibrosis) binds Calcium in the stool.
Chvostek’s Sx: tap the skin lightly in front of the
Hypocalcemia
(cont)
ear (over the facial nerve), if the corner of the
mouth draws up, d/t muscular contraction =
+Chvostek’s Sx.
Trousseau’s Sx: + if carpal spasm after BP cuff
Manif:acute
situation related to
inflated ~ 3min.
• Clinical
increased muscular excitability: tetany.
+Chvostek’s Sx, + Trousseau’s Sx.
• In children: Twitching, cramping, tingling
around the mouth or fingers, carpal/pedal
spasms.
• In infants: tremors, muscle twitches, brief
tonic-clonic seizures, CHF.
• Laryngospasm, seizures and cardiac
arrhythmias in severe situations.
Hypocalcemia (cont 2)
• In children and adolescents, chronic
hypocalcemia more common, manif. By
spontaneous fractures.
Lab tests: serum Ca; bone density study
Rx: oral and/or IV Ca, Ca rich diet
Hypermagnesemia
• Excess in Mg.
• Imbalances characterized by neuromuscular
irritability
• Causes: impaired renal function, Mag
Sulfate given perinatally to treat eclampsia,
increased use of laxatives, enemas,
antacids, IV fluid additives.
Hypermagnesemia (cont)
• Clinical Manif: decreased muscle
irritability, hypotension, bradycardia,
drowsiness, lethargy, weak or absent
DTR’s.
• Rx: increase fluids, diuretics, dialysis.
Hypomagnesemia
• Decreased serum Mg.
• Stored in cells and bones
• Causes: prolonged NPO without
replacement, chronic malnutrition,
chronic diarrhea, short bowel syndrome,
malabsorption syndromes, steatorrhea,
multiple transfusions, prolonged NG Sx,
some medications.
Hypomagnesemia (cont)
• Clinical manif: increased neuromuscular
excitability (tetany). Hyperactive
reflexes, skeletal muscle cramps,
twitching, tremors, cardiac arrhythmias,
seizures.
• Lab: serum Mg along with Ca and K.
• Rx: po/IV Magnesium admin and
treating underlying cause of imbalance.
Critical Thinking: Clinical Evaluation
of Fluid and Electrolyte Imbalance
• How can you evaluate children
appropriately for fluid and electrolyte
imbalance without thinking through the
clinical manifestations of every possible
disorder, one after the other?
Answer to Critical Thinking:
3 paragraphs of text that review this concept and pull the content
together with clinical application:
•
1) risk factor assessment
•
2) exam several body systems: cardiovascular, respiratory,
neurological
•
3) look for factors that alter intake, retention, and loss of fluids
and electrolytes
•
4) consider growth and development to realize problems most
common to the age group.
•
5) clinical assessment: wt, fluid balance, vascular volume (BP,
HR), interstitial volume (edema?), mentation, DTR’s, muscle
irritability, GI function, cardiac rhythm, assess electrolyte levels.
Fluid and Electrolyte
Worksheet
• Use the fluid and electrolyte worksheet
to help review some of the major
concepts of fluid and electrolyte
imbalance.
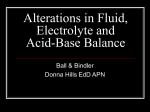
pH
- Is the acidity or alkalinity of a solution.
- From French pouvoir hydrogène ("hydrogen power“)
- pH is the Hydrogen ion concentration [H+] of a
solution.
- It is a measure of the solution's acidity.
• pH is defined as the negative logarithm of the concentration
of H+ ions:
pH = -log10[H+]
• The greater the concentration of H+, the more
acidic a solution is.
• The lower the concentration of H+, the more
basic or alkaline a solution becomes.
Neutral
7
1
Acidic
14
Alkaline
H+
HCO3-
Neutral
Acidic
Alkaline
Acid Base Balance
• normal arterial blood pH: 7.35-7.43 (in
general)
• Acidosis < 7.35 : too much acid
• Alkalotic > 7.43 : too little acid
• pCO2 reflects carbonic acid status:
• 40 mmHg (+- 5)
• HCO3- reflects metabolic acid status:
• 24 mmol/l (+- 4)
Respiratory Acidosis
•
•
•
•
caused by decr respir effort
build up of CO2 in the blood
pH decr or normal; pCO2 incr.
Symptoms manifested: confusion,
lethargy, HA, incr ICP, coma,
tachycardia, arrhythmias
Management of Respiratory
Acidosis
•
•
•
•
Incr ventilatory rate
give O2
intubate
adm NaHCO3
Clinical Conditions that cause
Respir Acidosis
• conditions associated with decreased
respiratory drive, impaired gas
exchange/air trapping, ie:
• head trauma, general anesthesia, drug
overdose, brain tumor, sleep apnea,
mechanical under ventilation, asthma,
croup/epiglottitis, CF, atelectasis, MD,
pneumothorax.
Respiratory Alkalosis
•
•
•
•
caused by hyperventilation
CO2 is being blown off
pH incr : pCo2 decr
Symptoms: dizziness, confusion,
neuromuscular irritability, paresthesias
in extremities and circumoral, muscle
cramping, carpal or pedal spasms.
Management of Resp. Alkalosis
• First determine if oxygenation is adequate, if
not, you don’t want to slow the RR.
• Determine the cause and correct it:
• Causes of hypervent: hypoxemia, anxiety, pain,
fever, ASA toxicity, meningitis/encephalitis,
Gram - sepsis, mechanical overventilation.
• Ipecac is no longer recommended for treatment
of ingestions.
Metabolic Acidosis
•
•
•
•
•
caused by a loss of bicarbonate (HCO3)
therefore, is an incr of acids in the blood
pH decr or moving towards normal
pCo2 decr ; HCO3 decr
Symptoms: Kussmaul respirations = incr rate
and depth as compensation (hyperventilation /
acetone breath), confusion, hypotension, tissue
hypoxia, cardiac arrhythmias, pulmonary
edema.
Management of Metabolic Acidosis
• Identify and treat underlying cause
• In severe case may give IV NaHCO3 to incr
pH, or insulin/glucose.
• Causes of MA for gain of acid: ingestion of
ASA, antifreeze, oliguria, RF, HAL, DKA,
starvation or ETOH KA, lactic acidosis (tissue
hypoxia).
• Loss of HCO3: maple syrup urine disease,
diarrhea, RF.
Metabolic Alkalosis
• caused by loss of H+ or HCO3 retention
• HCO3 incr with probable incr in pH, incr
pCO2.
• Symptoms:weak, dizzy, muscle cramps,
twitching, tremors, slow shallow resp.,
disorientation, seizures.
Management of Metabolic
Alkalosis
• correct underlying cause; facilitate renal
excretion of HCO3.
• admin NS, K+ if hypokalemic, replace loss
of fluids, prec for Sz, monitor I and O and
electrolytes
• Causes: prolonged vomiting, ingestion of lg
quantities of bicarb, antacids, loss of NG
fluids, hypokalemia from prolonged diuretic
use, multiple blood transfusion with citrate.
ABG Basic (Uncompensated)
Analysis
• Resp Acidosis: low pH and high PaCO2
• Resp Alkalosis: incr pH and low PaCO2
• Metab Acidosis: low pH and nl PaCo2;
decr HCO3
• Metab Alkalosis: high pH; nl PaCO2 ;
high HCO3
ABG Analysis with
Compensation
• Resp Acidosis: HCO3 will incr, pH will
approach nl; PaCO2 will still be increased
• Resp Alkalosis: HCO3 will decr, pH will
approach nl; PaCO2 will still be decreased
• Metab Acidosis: PaCO2 will decr, pH will
approach nl; HCO3 will still be decreased
• Metab Alkalosis: PaCO2 will incr, pH will
approach nl; HCO3 will still be increased
Examples of ABG:
• pH 7.35-7.43 PaCO2 35-45 HCO3 20-28
=Norm
• pH 7.33
PaCO2 52
HCO3 26
• pH 7.48
PaCO2 32
HCO3 24
• pH 7.28
PaCO2 37
HCO3 18
• pH 7. 45
PaCO2 38
HCO3 32
That’s all, folks!