Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
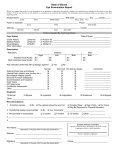
Chapter 2 Understanding Medical Documents Importance Medical Reports 1 The transcribed medical report is a legal medical document that communicates the patient’s health status. Medical records provide documented evidence of a patient’s medical treatment to insurance companies, for federal and state regulatory requirements. Importance Medical Reports 2 Medical records are vital records for your employer’s accounting department. Medical reports dictated in office practice, hospital, and inpatient facilities have similarities and differences. Medical Reports in Inpatient history and physical examination operative report consultation discharge summary * These records are referred to as the “big four” Medical Reports in Outpatient Consultation letters Chart notes History & physical examination reports Diagnostic imaging reports Procedure reports Information for identification Each report must include: Patient’s legal name Date of birth File number (ex. Social Security No.) Formatting Signature Lines Method 1. The physician’s or dictator’s name is followed by the initials of the transcriptionist on the third or fourth line below the last entry line. Method 2. The physician’s or dictator’s initials are followed by the initials of the transcriptionist, the date of dictation, and date of transcription. METHOD 1 Potter T. Bucky, MD Potter T. Bucky, MD/cd METHOD 2 Potter T. Bucky, MD Potter T. Bucky, MD/cd ptb:XX D: 11/20/xx (date the report was dictated) T: 11/21/xx (date the report was transcribed) Outpatient Medical Documents Chart Note (Progress Note or Follow-up Note) Dictated by a physician after talking, examining, or meeting with the patient. Chart Note 1 The chart note contains: Precise description of the patient’s major presenting problem (chief complaint) Physical findings Physician’s plan of treatment. Chart Note 2 It may also include: Results of laboratory test Results of x-ray test The Look of Chart Notes FORMAT Margins = 0.5 inches Single spacing No blank lines separating the topics * In this textbook you will format the chart notes and other medical documents in block style using 1-inch margins, single spacing, blank lines separating the topics which are capitalized. Pointers Be sure that the patient’s name is spelled correctly. The document is dated with the month, day and year of the visit. Statistical Data Format on Chart Notes 1 Statistical data for the first page: Patient Name: Doe, Jane Date of Birth: December 21, 1952 Examination Date: April 1, 20xx Statistical Data Format on Chart Notes 2 Statistical data for continuation pages: Patient Name: Doe, Jane Date of Birth: December 21, 1952 Page 2 Chart Notes Using the SOAP Format A common chart note format is the SOAP method. Subjective S: Subjective findings that are typically associated with what prompted the patient to seek medical care. A patient will describe feelings and symptoms to the physician. Example: My head and throat hurt and I have been throwing up all day. Objective O : Objective findings are measurable findings discovered by the physician or by the results of diagnostic studies or laboratory tests. Example: Temperature is 103.2ºF, and throat culture is positive. Assessment A : Assessment is the physician’s diagnosis or diagnoses of the patient;s disease or condition, based on subjective and objective findings. Example: Strep throat. Plan P : Plan is the treatment plan developed by the physician relative to the findings of the subjective and objective assessment of the patient. Example: Amoxicillin 250 mg t.i.d. X 10 days. Chart Notes Using the History and Physical (H&P) Format H&P Format 1 Format 1 History of present illness (abbreviated HPI) Past medical history (abbreviated PMH) Physical exam (abbreviated PX, PE, or CPX) Impression (abbreviated IMP) Plan (abbreviated RX) H&P Format Format 2 Chief complaint (abbreviated CC) Past medical history Physical exam Laboratory X-ray Diagnosis (abbreviated DX) Treatment (abbreviated TX) 2 History and Physical Examination Reports The dictation style of history and physical examination reports contains recurrent phrases and terms. It also contains more negative than positive statements. Characteristics of H&P and Chart Notes Tendency to condense and abbreviate Short and cryptic Clipped sentences which lack subject or verb Clipped Sentence Structure CHEST : Clear to percussion and auscultation. Heart regular rate and rhythm. ABDOMEN : Flat, soft, nontender, nondistended, normoactive bowel sounds. RECTAL : No masses. Guaiac negative. Clipped Sentence Structure This means: The chest was clear to percussion and auscultation. The heart rate and rhythm were regular. The abdomen was soft, nontender, was not distended, and had normal bowel sounds. The rectal exam was negative in that no masses were found, and the guaiac test found no occult blood in the feces. Formatting Statistical Data on History & Physical Examination Reports Statistical Data on H&P First Page: Patient Name: Doe, Jane File Number: 00912 Date of Birth: December 21, 1952 Examination Date: April 1, 20xx Physician: Potter T. Bucky Statistical Data on H&P Continuation page: Patient Name: Doe, Jane File Number: 00912 Date of Birth: December 21, 1952 Examination Date: April 1, 20xx Physician: Potter T. Bucky Page 2 Topics Included in the “History” Heading of a History and Physical Examination Report Pointers The H&P report is divided into two headings: “History” and “Physical” Topic headings are formatted in all capital letters. H&P Exam Report Topics HISTORY Chief complaint is the specific reason for which the patient sought medical care, stated in the most concise terms or sometimes quoted in the patient;s own words. History History of present illness contains all historical information that was given by the patient concerning the illness. This information includes all relevant symptoms and their duration and any remedies that have been attempted. Past Medical History Includes information about previous illness, injuries, surgeries, and chronic conditions a patient may have had, along with any allergies to medications. This topic may also include immunizations. Allergies Is a list of the patient’s allergies. Allergies are keyed in either all capitals, boldfaced, or underlined to call attention to their importance. The format varies by facility. Medications may be included in this section or under a separate heading. Medications Is a list of medications that the patient is currently taking. Sometimes this information is not listed as a separate topic but included under “Past Medical History” or “Allergies”. Family History Consists of information about any hereditary or familial diseases. Social History Is included if the physician believes this information is pertinent to the patient’s treatment plan. This topic may include lifestyle habits such as smoking, and drinking, as well as the patient’s occupation, hobbies, family structure, and living arrangements. Review of Systems (ROS) Includes a brief review of any relevant information about each major body system. Depending on the patient’s problem, this topic can be very comprehensive and divided into subtopics such as HEENT, cardiovascular, respiratory, gastrointestinal, genitourinary, gynecologic, neuropsychiatric, and Continuation… musculoskeletal, or it may be combined into one paragraph or simply be a brief statement such as “noncontributory” when all systems are negative. Topics included in the “Physical Examination” Heading of a H&P Examination Report Physical Examination report The “Physical Examination” heading of the report is exactly what its name implies. The physician completes a physical examination of the patient, and the findings are transcribed under the pertinent topic. The major topics for the physical examination of the report include the following: General section The general section discusses the appearance of the patient such as pallor, gait, mood, and personal hygiene. It also includes a statement of the patient’s vital signs (blood pressure, temperature, pulse, and respiration). HEENT Is an abbreviation for the head, eyes, ears, nose and throat. Neck The neck is palpated for enlargement of the lymph nodes or thyroid gland, assessment of the carotid pulses, and distention of the jugular veins. Chest The chest also includes the thorax, breasts, and axilla areas. Lungs The lungs are evaluated by auscultation, during which the physician listens with a stethoscope to air moving in and out of the lungs. Diseases or injury can produce abnormal changes in the quality and volume or loud ness in breath sounds. The physician also may perform the percussion (tapping) maneuver. Heart The heart is evaluated with a stethoscope for any abnormal sounds, such as murmurs or bruits (sound or murmur heard in auscultation), clicks (brief, sharp sounds, especially any of the short, dry clicking heart sounds during systole), rubs (sounds cause by rubbing together of two serous surfaces), thrills (vibrations), and gallops (disordered heart rhythm). Abdomen The abdomen is assessed by auscultation, in which the physician listens for any abnormal bowel sounds, and percussion, in which the physician palpates the abdomen for tenderness, guarding, and masses. Pelvic The pelvic region or genitalia are examined. Women may undergo a bimanual pelvic exam and Papnicolaou (Pap) smear. Rectal The rectal exam involves a digital evaluation of the rectum for deformity or masses. The physician also may comment on the results of a guaiac test (for occult blood) or colonoscopy (fiberoptic instrument) in this topic of the report. Men may undergo a digital rectal examination of the prostate. Digital palpation is a useful method for detection of early prostatic carcinoma. Exremities The extremities are examined for developmental or traumatic deformities, muscle wasting, and stiffness. The bones, joints, and muscles of all extremities are evaluated. Neurological The neurological examination is a systematic evaluation of the nervous system, including mental status, functioning of the cranial nerves and reflexes, and sensory and neuromuscular function. The Babinski reflex and deep tendon reflexes (DTRs) are usually checked. Laboratory Data Include laboratory test results, such as complete blood count (CBC), white blood cell count (WBC), and urinalysis (UA). Impression Is the physician’s diagnosis or diagnoses of the patient’s clinical condition or disease based on the findings of the physical examination and diagnostic tests. Plan of Treatment Is developed by the physician based on the findings of the physical examination and diagnostic tests. Diagnostic Imaging Reports and Letters Diagnostic Imaging Reports Diagnostic imaging reports include: Clinical radiology (x-ray) Ultrasonography (US) or sonography Computerized tomography (CT) Nuclear medicine (NM) Magnetic Resonance imaging (MRI) Each area is classified as a separate imaging modality because each uses a different type of energy and recording device to image the body. A compute is involved in the imaging process of almost all differing modalities. Hence the image can be displayed on a video monitor and then digitally stored or printed on traditional x-ray film. All modalities except diagnostic x-ray have crosssectional image recording capabilities. Diagnostic X-rays Diagnostic x-rays use low levels of radiation to record images of the body on x-ray film. Newer methods sometimes allow the image to be digitized and stored in a computer. Ultrasound Ultrasound or sonography uses highfrequency sound waves to image the body. It is unique in that it does not expose patients to ionizing radiation and therefore is the modality of choice to evaluate maternal or fetal anatomy in pregnant women. Nuclear Medicine In nuclear medicine the energy source is a radioactive isotope that is injected into the patient’s body, and then specialized computers and cameras record and store the image. Computerized Tomography Uses a combination of radiation and computerized imaging techniques to record and display an individual’s anatomy. It is sometimes referred to as CAT scan (computerized axial tomography). This term is technically incorrect because today’s CT scanners can image the body in more than just the axial plane. Magnetic Resonance Imaging Is a very sophisticated machine that uses a magnetic field and radiofrequency waves to generate an image. It does not use ionizing radiation and often produces sharper soft-tissue images than other modalities.