Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
ABUSE & IMAGING
PEDS & GERIATRICS
SOME IMAGES MAY BE DISTURBING
YOU HAVE A LEGAL RESPONSIBILITY
TO REPORT POSSIBLE ABUSE
CHILD ABUSE
• MULTIPLE INJURIES
• COVERS MORE THAN 1 PLANE
• DEFENSIVE WOUNDS
• BE ALERT
• Most abused and neglected children never come to the
attention of government authorities.
• This is particularly true for neglected and sexually
abused children, who may have no physical signs of
harm.
• In the case of sexual abuse, secrecy and intense
feelings of shame may prevent children, and adults
aware of the abuse, from seeking help.
• Therefore, official government statistics do not indicate
actual rates of child abuse.
• Government statistics are based on cases that were
• (a) reported to social service agencies,
• (b) investigated by child protection workers
• (c) had sufficient evidence to determine that a legal
definition of "abuse" or "neglect" was met.
• Failure to report suspected abuse is against the law and harms
children
• Every state has laws that require healthcare workers and others to
report suspected child abuse to a law enforcement agency or child
protective services.
• When circumstances suggest a reasonable suspicion that a child
could be a victim of abuse, a report is required.
• It is not the job of the "mandatory reporter" to investigate the facts in
these cases. The law simply directs them to file a report with a law
enforcement agency or child protective services whenever facts
might suggest a reasonable suspicion of abuse. Mandatory
reporters are not permitted to pick and choose which cases they will
report based on their personal opinion. Those who may feel that
there is nothing wrong with adult-child sex cannot simply pretend
child rape is merely consensual sex. By law, an underage girl cannot
consent to sex. Nor does the law allow a mandatory reporter to
decide whether or not a report should be filed based on the
statements of the child, because cover stories are often concocted
to cover up cases of abuse.
Child neglect, also called
psychological abuse
• , is a form of child abuse. It occurs when
someone intentionally does not provide the child
of the necessities of life, or does so with reckless
disregard for the child's well being. Such
necessities include food and water for healthy
growth, shelter, clothing, and medical care. They
child may also lack a safe environment, and
adult emotional support. The abuser may ignore,
insult, or threaten the child with violence.
• Some authorities consider witnessing violence
or severe abuse between parents or adults
another form of psychological abuse.
Symptoms of psychological abuse
may include
• Difficulties in school
• Eating disorders, resulting in weight
loss or poor weight gain
• Emotional issues such as low self
esteem, depression, and anxiety
• Rebellious behavior
• Sleep disorders
• Vague physical complaints
Battered child syndrome;
Physical abuse - children
• The physical signs of child abuse used to be
called battered child syndrome. This syndrome
referred to multiple fractures in different states of
healing. The fractures occurred at different times
in children too young to have received the
fractures as a result of an accident.
• The definition of child abuse has since
expanded significantly. Physical child abuse or
non-accidental child trauma refers not only to
multiple fractures at different ages, but it also
includes numerous other signs of injury.
• Physical abuse tends to occur at moments of greatest stress, when
someone strikes out in anger at the child. Many of those who
commit physical abuse have been abused themselves as children.
As a result, they often do not realize that abuse is not appropriate
discipline. Those who commit physical abuse also frequently have
poor impulse control, which prevents them from thinking about what
happens as a result of their actions.
• Because adults are so much stronger and bigger than children, an
abused child can be severely injured or killed by accident. For
example, shaking an infant, especially if the head hits something,
even against a soft object like a mattress or pillow, can cause
bleeding over the brain (subdural hematoma). This can cause
permanent brain damage or death. (See shaken baby syndrome.)
SHAKEN BABY SYNDROME
• is a severe form of head injury caused by the baby's brain
rebounding inside of the baby's skull when shaken.
• In this injury there is bruising of the brain, swelling, pressure, and
bleeding (intracerebral hemorrhage).
• This can easily lead to permanent, severe brain damage or death. If
a child has this injury there are usually no outward physical signs of
trauma, but there may be a change in the child's behavior such as
irritability, lethargy, pale or bluish skin, vomiting, and convulsions.
SHAKEN BABY SYNDROME
• The tight grasp around the chest that
accompanies this shaking may also
cause rib fractures (these are also
highly specific for abuse). These rib
fractures may be incidentally found on
chest X-rays performed for other
reasons, such as to evaluate for
pneumonia.
• Finally, the shaken infant syndrome may also
include throwing the baby down or into a
hard surface, like a wall or table.
• This will cause swelling at the point of
impact and, if the head is the point of impact,
may add to brain damage by causing local
bleeding and swelling in and on the brain
and scalp.
• This impact injury often accompanies
shaking; this may be refered to as "the
shaken-impact syndrome."
Rate of child abuse is fairly high.
• The most common form is neglect.
• Child abuse accounts for at least 1,400
deaths in children each year.
• The major risk factors for someone to
abuse another person include:
• Poverty
• Lack of education
• Being a single parent
• Alcoholism
• Other drug abuse
Symptoms of physical abuse
•
• Adult may bring an injured child to an emergency room
with a strange explanation of the cause of the injury. The
child's injury may not be recent.
• Symptoms include:
• Broken bones that are unusual and unexplained
• Bruise marks shaped like hands, fingers, or objects
(such as a belt)
• Bruises in areas where normal childhood activities
would not usually result in bruising
• Burn (scalding) marks, seen when a child is placed
in hot water as a punishment -- particularly "glove"
or "sock" burn patterns
• Burns from an electric stove, radiator, heater or
other hot objects, usually seen on the child's hands,
arms or buttocks
Symptoms of physical abuse
• Cigarette burns on exposed areas or the genitals
• Black eyes in an infant or a similar, unexplained
injury in a child
• Human bite marks
• Lash marks
• Choke marks around neck
• Circular marks around wrists or ankles (indicating
twisting or tying up)
• Separated sutures
• Bulging fontanelle
• Evidence of unexplained abdominal injury (such as
bruised or ruptured intestines due to punching)
• Unexplained unconsciousness in infant
Typical injuries in abused children include:
• Bleeding in the back of the eye, seen
with shaken baby syndrome or a direct
blow to the head
• Internal damage, such as bleeding or
rupture of an organ from blunt trauma
• Any fracture in an infant too young to
walk or crawl
• Evidence of fractures at the tip of long
bones or spiral-type fractures that
result from twisting
• Fractured ribs, especially in the back
Typical injuries in abused children include:
• Evidence of skull fracture (multiple
fractures of different ages may be
present)
• Subdural hematoma (collection of
blood in the brain) without plausible
explanation
• Multiple bruises that occured at
different times -- especially in unusual
areas of the body or in patterns that
suggest choking, twisting, or severe
beating with objects or hands
• Other unusual skin damage, including
burns or burn scars
The following tests can reveal
physical injuries
• Bone x-ray -- a skeletal survey is done
whenever physical abuse is suspected. All
the child's bones, including the skull, are xrayed to look for unseen fractures or old,
healing fractures.
• MRI or CT scan of the head or abdomen are
done if there is a skull fracture, bleeding in
the eye, unexplained vomiting, severe
bruising of the face, skull or abdomen, or
unexplained neurological symptoms,
headaches, or loss of consciousness.
There are several types of bone
fracture, including:
• Oblique - a fracture which goes at an
angle to the axis
• Comminuted - a fracture of many
relatively small fragments
• Spiral - a fracture which runs around
the axis of the bone
• Compound - a fracture (also called
open) which breaks the skin
• Physical abuse of a child can lead to severe
brain damage, disfigurement, blindness,
crippling, and death. Abused individuals may
carry emotional scars for a lifetime.
• Children can be removed permanently from the
parents' custody if the parents are the
perpetrators and the cause is sufficient to
warrant termination of parental rights. However,
this experience itself can result in significant
psychological problems due to feelings of
rejection, or if the placement does not result in a
strong, long-term attachment to new caregivers.
• Recognize the warning signs of
potential abuse.
• For example, a caregiver may:
• Previously abused a child
• Fail to maintain the child's proper hygiene or
care
• Appear to lack love or concern
• Have alcohol or drug problems
• Have emotional problems or mental illness
• Was abused as a child
• Has high stress factors, including poverty
All states require that you report
any known or suspected child
abuse.
Call the police and Child
Protection Services
Sexual abuse - children
• Child sexual abuse is the deliberate
exposure of minor children to sexual
activity.
• This means a child is forced or talked into
sex or sexual activities by another person.
Such abuse includes touching (fondling),
sexual intercourse, oral sex, pornography,
and other sexual activity.
Sexual abuse - children
• With the exception of sexual abuse among
family members (incestuous relationships), child
sexual abuse was not clearly described until the
late 1970s.
• The problem is far more common than had been
thought. Indeed, the medical literature up
through the mid-1970s contained articles about
children and sexually transmitted diseases, such
as gonorrhea.
• However, there was no discussion of how the
children caught such disease. There was great
reluctance in society to deal with this issue, but
after 30 years of examination worldwide, child
sexual abuse is now considered a serious issue.
Causes, incidence, and risk factors
•
It is difficult to determine how common
child sexual abuse is. It is often more
secret than physical abuse. Children are
often scared to tell someone about the
event. According to the American
Academy of Child and Adolescent
Psychiatry, it is reported up to 80,000
times a year, but the actual number of
unreported events is probably much
higher.
Causes, incidence, and risk factors
• Abusers are usually men.
• They usually know the person they are
abusing.
• This is the case in 80 to 90% of cases.
• Because the abuser violates the trust of
the younger person, it makes the sexual
abuse even more psychologically
devastating.
Causes, incidence, and risk factors
• Child sexual abuse occurs in all social and
economic classes of people, but it has the
same type of risk factors as physical child
abuse, including poverty, disordered
families, and abuse of alcohol and street
drugs.
• Abusers often have a history of physical or
sexual abuse themselves.
• A small group of repeated abusers suffer
from the psychiatric disorder pedophilia, in
which the preferred sexual contact is with
children.
Symptoms of child abuse are similar to
those seen in depression or severe
anxiety and nervousness.
•
•
•
•
They can include:
Repeated headaches
Stomach aches (vague complaints)
Bowel disorders, such as soiling oneself
(encopresis)
• Eating disorders, such as anorexia
nervosa
Symptoms of child abuse are similar to
those seen in depression or severe
anxiety and nervousness.
• Sleep problems
• Genital or rectal symptoms, such as pain
during a bowel movement or urination,
or vaginal itch or discharge
• Children may withdrawal from normal
activities, have excessive fears, do poorly in
school, and display disruptive behaviors
such as using alcohol and street drugs or
engaging in high-risk sexual behaviors.
Signs and tests
• If you suspect a child has been sexually abused, the
child should be examined as soon as possible by a
trained healthcare professional.
• A doctor's exam should not be delayed for any
reason. Many signs of injury related to sexual abuse are
temporary. Ideally, the exam should occur within 72
hours of the event or discovery. A complete physical
exam must always be performed, so that the examiner
can look for any signs of physical and sexual abuse. The
two forms of abuse may co-exist.
• Affected areas may include the mouth, throat, penis,
anus, and vagina, including the hymen. There are some
normal variations to this structure, but it can be affected
by abuse.
Signs and tests
• blood tests to check for sexually transmitted
diseases, such as syphilis and HIV, and
pregnancy in females. These tests can help
determine treatment.
• Photographs of injuries may help establish what
happened.
• Most pediatricians, many family medicine
doctors, and most emergency room (ER) doctors
have training in examining cases involving
sexual abuse.
• VCUG may be ordered for recurrent UTI’s
due to possible sexual abuse
Treatment
• All children who have been sexually abused or
traumatized in any way should receive mental health
counseling.
• Suspicion of child sexual abuse must be reported to child
protective services and the police. Medical professionals,
teachers, and child care professionals are required by
law to make a report.
• TELL YOUR SUPERVISOR
• Once a case is reported, child protection agencies and
the police must investigate. If the allegation is
considered true, the child must be protected from further
abuse. Placement with a non-abusing parent, another
relative, or a foster home may result.
• In physical abuse cases, the goal of child protection
agencies is to educate an abusing caretaker and attempt
to re-join the family together, if safe
• 3,500 Number of deaths due to
child abuse and neglect in 27
developed nations worldwide.
The United States, Mexico, and
Portugal have death rates 10 to
15 times higher than many of the
other countries.
• 40-47 Percent of sexual assaults
perpetrated against girls age 15
or younger worldwide.
76 Percent of United States child
abuse fatalities that were in
children aged 4 years or
younger.
More than 1/3
Number of U.S. child abuse
fatalities that were associated
with neglect, or in other words,
the denial of a child’s basic need
for food, warmth, clothing, and
medical care.
• 2.9 million
Number of reports of child abuse and neglect
received by U.S. Child Protective Services from
concerned teachers, policemen, social workers,
day care workers, friends and neighbors (2003).
That’s 39 referrals for every 1,000 children.
79 % of U.S. child abuse or neglect deaths
where one or both parents were involved. Much
of the time, the parent is young, without a high
school diploma, living in poverty, depressed, and
has experienced violence in his or her own life.
Injuries Worrisome for Child
Physical Abuse
• Skin and Soft Tissue Injury
• bruises on face, lips, mouth, torso, back, buttocks, thighs
– especially if in various stages of healing
– degree of bruising is greater than expected for the activity level of
the child
• bilateral black eyes ("raccoon eyes")
• patterned bruise (of inflicting instrument such as belt buckle,
hairbrush, or hand)
• human bite marks
• cigarette burns, especially on palms, soles of feet, back,
buttocks
• immersion burns
• patterned burns (curling iron, clothes iron, stove burner)
• rope burns
Skeletal Injuries
• fractures of ribs, ends of long bones
(near growth plates),
• spine
• multiple fractures
• fractures of differing ages
• any fracture inconsistent with the
developmental capabilities of the child
Head Injuries
• bleeding into/onto brain (subdural
hemorrhage)
• brain swelling (cerebral edema)
• multiple skull fractures ("eggshell"
fracture)
Abdominal Injuries
• small bowel injury (duodenal or jejunal
hematoma, bowel laceration)
• pancreatitis or pancreatic injury
• injury to liver, spleen, adrenal glands
Signs of Neglect
•
•
•
•
•
•
•
•
•
lack of appropriate hygiene
inappropriate dress
bald spots
severe diaper rash
failure to thrive
lack of immunizations
lack of dental care
lack of supervision
abandonment
Parental Behavior Patterns Seen
in Abuse
•
•
•
•
lack of concern or detachment about injury
lack of response to child in pain
overly concerned about trivial injuries
has unrealistic expectations of the child (to
be behaviorally more mature)
• parents themselves may exhibit or have a
history of:
– drug or alcohol addiction
– psychosis
• lack of trust in health professionals
Radiographic skeletal survey in all
children less than 2 yrs suspected of
abuse.
• The abuse skeletal survey consists of individual
frontal X-rays of the following body parts:
•
•
•
•
•
•
•
•
•
•
chest
skull (also lateral)
upper arms (humeri)
forearms
hands
pelvis
upper legs (femurs)
lower legs (tibia/fibula)
ankles (also lateral views)
feet
• In children 12 months or younger, also perform:
• lateral thoracolumbar spine film
NOTE: Expert attention to technique and detail
is necessary for quality radiographs that show
some of the very subtle injuries of abuse.
• These are the radiographs that will go
to court - it is imperative that they be
well-performed.
It is recommended that these films be
obtained:
• with mammography or high-detail
extremity film (exquisite detail)
Expert attention to technique and detail
is necessary for quality radiographs
• during regular duty hours (not in the
middle of the night by the on-call
technologist)
• and submitted to a pediatric radiologist
for interpretation
• NOTE: some of the injuries of abuse
heal very quickly (in less than 2 weeks),
so it is imperative that the evaluation of
the possibly abused child be
accomplished as promptly as possible
Abuse imaging
• Head CT scan: Perform on all suspected
abuse victims 1 year of age or younger.
• Nuclear Medicine Bone Scan. Usually not
necessary. Perform this if:
– there are equivocal findings on the skeletal
survey
– there is a high clinical suspicion of skeletal injury
but the skeletal survey is normal
• Brain MRI scan: Perform if the susupected or
confirmed abuse is older (weeks to months
or even years), to look for evidence of
chronic blood collections (chronic subdural
hematoma) and brain damage.
The Child Abuse Homicide
• Abuse should be considered when any child
dies unexpectedly.
The following should be performed on all
unexplained childhood deaths:
• forensic autopsy
• radiographic skeletal survey, preferably at a
hospital (try to have this done BEFORE the
body is taken to the morgue or medical
examiner's office)
• A full radiographic evaluation should be
considered an integral part of a complete
autopsy on a young child!
CASE STUDIES OF
PEDIATRIC ABUSE
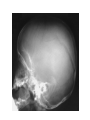
Ped injury – corner fx
• This 2 month old baby girl was brought into the local ER with
scalp swelling
• Patterns of skull fracture that suggest child abuse are multiple
('eggshell') fractures (as in this case)
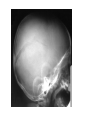
• 1 year old child
brought in by
ambulance
comatose.
• This child was
violently shaken,
causing severe
brain injury,
evidenced by
diffuse cerebral
edema.
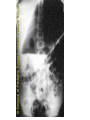
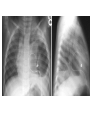
4 month old with cough,
chest X-ray request says
"rule out pneumonia."
Posterior rib fracture of the
left 7th rib
This fracture is less than 14
days old as there is no visible
callus.
This is a case of child abuse incidentally found on
CXR because of the detection of the rib fracture,
which was unrelated to the child's presenting
complaint
Healing right posterior 5th-7th and 9th rib fractures, as well as multiple
healing right lateral rib fractures
3 MO OLD – BROUGHT IN FOR ABD PAIN AND VOMITING
CORNER OR BUCKLE FX
• 4 month old
baby with brain
injury
suspicious for
child abuse.
Skeletal survey
performed to
evaluate for
other injuries
of abuse.
There is a
corner fracture
of the distal
femur
• This corner fracture (also known as a metaphyseal or
bucket handle fracture) is highly specific for abuse
• The metaphyseal lesion in abused infants
• It occurs when a child is violently shaken, or other forms
of torsional stress and shear are applied to a limb (such
as severe twisting or wrenching of the limb).
• When this occurs from shaking, the shaking causes the
arms and legs to flail violently, and shear forces
(whiplash forces) are exerted on the distal ends of long
bones.
• Fractures occur through the most immature (weakest)
part of the growing bone, which is immediately adjacent
to the metaphyses or growth plate.
• This fracture shears off a disc of bone at the end of the
shaft; this fracture fragment may resemble a "corner" of
bone or a bucket handle depending on the orientation of
the fracture site to the X-ray film.
• Notice how subtle this fracture is - Visualizing these
fractures is very dependent on high detail radiography.
• 3 mo deceased sibling of a child who is found
to have rib and metaphyseal injuries indicative
of abuse.
• Cause of death of the abused infants sibling
listed by coroner's office as "bacterial
peritonitis" from an unknown cause; death
ruled "natural"
• Body exhumed for reevaluation when younger
sibling presented with abuse injuries.
• This is a specimen radiograph of the
dissected limb of the exhumed body
• A forensic autopsy does not evaluate the
limbs well (especially the metaphyses), and
therefore metaphyseal fractures will often be
missed.
• In this case, the child did die of bacterial
peritonitis from an abuse-related traumatic
bowel perforation.
Post Mortem
Of tibia
11 month old female with possible right-sided posterior rib fractures
at recent skeletal survey.
Bone scan shows focal increased uptake along multiple posterior
right ribs , the left humeral shaft & both humeral heads
Therefore, plain X-rays of the skeleton (in the areas of abnormality
identified at bone scan) are almost always still needed to evaluate for the
exact nature of the abnormality.
Use of bone scans for when there is an equivocal finding or there is high
clinical suspicion but the plain X-rays are normal. Bone scans will detect
those difficult to see posterior rib fractures, as in this case.
• 3 month old child with
vertebral abnormality
noted on chest X-ray.
• Compression injury to the
body of L1. Notice the
angulation of L1 relative to
T12 above it and the defect in
the anterior superior margin of
the body of L1
Injuries to the
thoracolumbar junction
• are relatively common in abuse, especially in
shaken infant syndrome.
• Shaking by holding the infant around the chest
makes the thoracolumbar junction a fulcrum.
• Violent shaking can thus create strong
compression forces on vertebral bodies at this
area of the spine (very much like the "lapbelt"
injuries in motor vehicle accidents).
• Compression fractures can occur, and there can
even be rupture of intervertebral ligaments and
disc herniations, too.
•
3 1/2 year old with 4
day history persistent
vomiting after eating
and abdominal pain.
• Upper GI shows a
mass in the wall of the
descending
duodenum
• This is consistent with
a duodenal
hematoma.
duodenal hematoma
• It is a relatively common injury in abuse and is
typically seen in older children who are punched or
kicked in the abdomen (intentionally or accidentally).
• It is an unusual injury in very young children (less
than 2 years old).
• Of note, abdominal injury, such as this duodenal
hematoma, is the leading cause of morbidity and
mortality in the older abused child.
• Because abdominal injuries are usually seen in older
children, who are often quite active, identifying the
injury as abuse-related is more difficult.
• Correlation with history and other evidence of abuse
suggest the diagnosis.
• This 6-week old male was well until two days
prior to presenting to the ED when his left thigh
suddenly became swollen.
• His mother, who cares for him both day and
night, states that there is no history of trauma.
She denies any rough play, shaking, or any
chance of trauma, such as rolling off the bed or
the couch.
• Further questioning reveals that sometimes the
infant's father, paternal grandmother, paternal
grandfather, and paternal aunt, all living in the
same household, also care for the infant.
• There is also a one-year old female sibling a 2year old female cousin, and great grandparents
all living in the same house, who sometimes play
with the infant.
• Both mother and father are 18 years of age
• This radiograph shows
an obvious oblique
fracture of the proximal
shaft of the left femur,
with superior and
anterior displacement of
the distal fracture
fragment
• Because of the strong
suspicion of intentional
trauma (child abuse),
the infant is hospitalized
and a skeletal survey is
done
• The upper extremity radiograph
(left image) reveals an old fracture
of the right proximal radius. There
is some periosteal elevation
surrounding the fracture indicating
that the fracture did not occur
recently. The lower extremity
radiograph (right image) reveals a
healing fracture of the right tibia
with periosteal reaction along the
entire shaft of the right tibia. The
fracture line itself is not easily
identified.
• The vertebral
body of T12
appears much
flatter than the
other thoracic
vertebra. T10
and L2 may
also be slightly
flattened.
Because of the
difficulty in
diagnosing
these as
vertebral body
compression
fractures, a
bone scan is
done for
correlation.
•
•
•
•
This bone scan confirms the long bone fractures.
There is an obvious hot spot
right radius. left femur and right tibia
also the occiput suggesting a fracture or a
subperiosteal contusion.
• There are no obvious vertebral hot spots
suggesting that the flattened vertebral bodies
may not represent fractures
• After being fitted with an orthopedic harness,
child protective services placed the infant in a
foster home.
• The young children living in the household were
also removed and placed in foster homes.
The upper extremity
radiograph (left image) reveals
an old fracture of the right
proximal radius
The lower extremity
radiograph (right image)
reveals a healing fracture of
the right tibia with periosteal
reaction along the entire shaft
of the right tibia.
The fracture line itself is not
easily identified.
• 6-week old male was well until two days
prior to presenting to the ED when his
left thigh suddenly became swollen.
• There is also a one-year old female
sibling a 2-year old female cousin, and
great grandparents all living in the same
house, who sometimes play with the
infant.
• Both mother and father are 18 years of
age.
This radiograph shows an
obvious oblique fracture of
the proximal shaft of the left
femur
Because of the strong
suspicion of intentional
trauma (child abuse), the
infant is hospitalized and a
skeletal survey is done.
The following positive
radiographs are shown:
7 WEEK OLD
Wheezing and
respiratory
distress are a
common
presentation of
CHF in infants.
Tachypnea alone
may be the
earliest sign.
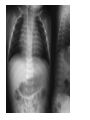
• Chest radiograph
showing different
stages of healing
posterior rib
fractures (arrows).
SIGNS OF ABUSE
• Physical abuse most often is a pattern of
repeated behavior, with bruises and welts being
the most frequent evidence of such.
• Typical sites for inflicted bruises include the neck
(choke marks), upper lip and frenulum (forceful
feeding), ear lobe (pinch or slap marks), cheeks
(slap marks), buttocks and lower back
(paddling), the genital area and inner thighs.
• Human bite marks leave concentric bruises that
contain individual teeth marks. If the point-topoint distance between the canines (eye teeth)
is greater than 3.0 cm, the injury was inflicted by
someone with permanent teeth.
• Dating bruises is also important, and multiple
colors suggest multiple times of injury.
• Child abuse is a common cause of burns.
• Scald or immersion burns are the most common,
bearing the characteristic glove or stocking
pattern that is observed on physical
examination.
• With a water temperature of 130- 145 degrees
or greater
• Contact burns from a hot metal object or
cigarette are another type of burn seen with
child abuse.
• Head injuries are the most common cause
of death from child abuse
• Abdominal injury is the second most
common cause of death among battered
children. Ruptures of the spleen, liver or
bowel caused by a punch or kick can
result in the above with no visible bruises
or marks on the abdomen in over half the
cases.
• Rupture of the bladder may also occur.
• multiple fractures at multiple sites and in various
stages of healing should be considered abused
until proven otherwise
• Epiphyseal-metaphyseal injury is virtually
diagnostic of physical abuse in an infant, since
an infant cannot generate enough force to
fracture a bone at the epiphysis.
• Fractures secondary to abuse are more
commonly seen in children less than 3 years of
age.
• Conversely, less than 10% of children over 5
years of age who are abused sustain fractures.
• In general, a complete skeletal survey should be
done on all children less than 2 years of age
who are possible abuse victims.
FRACTURES
• A spiral or oblique fracture of long bones is
produced by a twisting mechanism.
• Whether accidental or non-accidental, a large
amount of force is required to produce a fracture
of the femur.
• A direct blow causing a transverse fracture can
also be seen with major violence.
• Young children who are not ambulatory cannot
produce enough force to fracture their femur. A
history of getting his/her leg "caught in the crib"
should be viewed with suspicion.
FRACTURES
• Rib fractures are highly suggestive of
abuse in infants and young children.
• Squeezing usually produces fractures of
the posterolateral aspects of the ribs.
• Shaking or choking a child has been
shown to produce fractures anteriorly in
the first or second ribs.
• Rib fractures secondary to trauma that is
NOT child abuse tend to occur in the
middle or anterior part of the rib cage.
FRACTURES
• Spinal fractures are infrequently seen in
child abuse cases. The mechanism is
usually one of compression, as a child is
forcibly seated into a chair or onto a
tabletop.
• There are several radiologic signs suggestive of abuse.
• These include healing fractures, multiple fractures,
fractures of unusual locations, and metaphyseal
fractures.
• The typical radiographic appearances have been
described as: a) "corner fractures", b) "bucket handle"
fractures, and c) subperiosteal hematoma with new bone
formation.
• Other radiographic findings suggestive of abuse include
posterior rib fractures, spinous process fractures, sternal
fractures, complex skull fractures, and diaphyseal spiral
and oblique fractures.
• Fractures showing different stages of healing are almost
signs of abuse.
• Any fracture which already shows signs of healing
suggests that the fracture is at least ten days old.
Review- signs of abuse
Just because a child has bruises does not mean that
he or she is abused. The most important thing is to
look for is a pattern of abuse.
Here are some of the signs to look for:
Physical Abuse
• Injuries to eyes or both sides of the head or body
(accidental injuries typically only affect one side of
the body);
• Frequently appearing injuries such as bruises, cuts
and/or burns. These may appear as grab marks,
human bite marks, cigarette burns.
• Destructive, aggressive or disruptive behavior.
• Fear of going home.
Review- signs of abuse
Sexual Abuse
• Symptoms of sexually transmitted diseases
• Injury to genital area
• Difficulty and/or pain when sitting or walking
• Sexually suggestive, inappropriate behavior
or verbalization
• Sexual victimization of other children
Review- signs of abuse
Maltreatment
• Obvious malnourishment, listlessness or
fatigue
• Stealing or begging for food
• Poor personal hygiene, torn and/or dirty
clothes
• Need for glasses, dental care or other
medical attention
• Frequent absence from or tardiness to
school
• Child inappropriately left unattended or
without supervision
1 YO IN ER
NO FEVER
RIBS FX SEEN
NO HX OF TRAUMA
CHILD ABUSE
& ELDER ABUSE
• Healthcare workers are responsible for
their patients’ safety. This would include
treating the patients according
• to their own age level. Treating their
patients within their age development will
assist the healthcare worker to
• deliver proper care.
ELDER ABUSE
• Each person is moving through the life cycle at all
times from birth to death.
• The patient’s life cycle stage can generally be
identified by physical attributes, psychosocial
tasks, common fears or stressors.
• As healthcare workers, you can deliver
appropriate care to each patient by identifying the
life cycle the patient
• is currently in and modify the delivery of your
treatment to be more effective and best treat the
patient.
• Abuse is any intentional or unintentional hurt of a
person. Elder abuse is any intentional or
unintentional hurt of a person who is
approximately 60 years of age or older.
ELDER ABUSE
• Abuse can be Domestic (in their home) or
Institutional (in a facility).
• Healthcare abusers can be doctors, nurses,
hospitals, caregivers, unlicensed “professionals”,
and
• nonprofessional healthcare providers. Abusers
may be family members, visitors or intruders.
• Never assume why someone may abuse an
elder.
• Report all instances of abuse to your immediate
on-site supervisor and your staffing specialist.
• Be able to report specific information about the
incident.
SIGNS & SYMPTOMS
OF ELDER ABUSE
• Warning Signs
• are frequent arguments between elder and caregiver or
changes in personality or behavior of
elder.
• If you suspect elderly abuse, but aren't sure, look for
clusters of the following physical and behavioral signs
PHYSICAL ABUSE
• Unexplained bruises, pressure marks, black
eyes, welts, lacerations, cuts, or burns
•
Bone fractures
• Sprains or dislocations
• Bite marks or restraint marks
• Broken glasses
• Underutilization of medication or overdose
– (via lab findings)
• Elder is not left alone with visitors
• Elder reports physical abuse
EMOTIONAL ABUSE
•
•
•
•
•
•
•
•
•
•
•
•
•
Upset or agitated
Withdrawn, depression or
non-communication
Sucking, biting or rocking
(usually with dementia)
Caregiver belittling or
controlling elder
Desertion at an institution
(hospital, nursing home, etc
or public locations)
Physical or chemical
restraints
Elder reports emotional abuse
ELDER NEGLECT
•
•
•
•
•
•
•
•
•
•
•
Dehydration, malnutrition,
or hunger
Physical weakness
Hazardous or unsafe living
conditions
Unsanitary & unclean living
Clothing unsuitable for
weather
Poor hygiene, foul body or
household odor
Lack of medical aids
SEXUAL ABUSE
•
•
•
•
•
Bruises around breasts or genitals
Unexplained VD or infections
Unexplained vaginal or anal bleeding
Torn, stained or bloody underclothing
Elder reports sexual abuse
HEALTHCARE ABUSE
• Duplicate billings for services
• Pill counts are under or over the number
the patient was prescribed
• Lack of inadequate medical care even
though bills are paid
ABUSERS
• Most abuse occurs in the home, and usually by
a family member. Most commonly the
perpetrators of elderly abuse are
• spouses or partners of elders. Next most
frequent abusers are the adult children of elders.
• Abusers can be men or women. Men ages thirtysix to fifty are the most common perpetrators.
In nursing homes & other long-term care
facilities, abusers may be employees,
visitors, or intruders.
• Anyone associated with an elder may abuse
them: friends, relatives, doctors, lawyers,
bankers, accountants, clergy,caregivers, or
strangers.
Taking care of the elderly, whether at
home or in an institution, can be
very stressful.
• The incidence of depression isvery high
among caregivers.
• Caregivers habitually lack exercise and
outdoor time, have inadequate nutrition,
and need more sleep.
• Many people with dementia have trouble
sleeping so caregivers are kept up caring
for them.
• Caregivers have a high level of anxiety.
• HOW TO REPORT ELDER ABUSE
• If an elder is in danger:
• Notify your on-site supervisor