Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
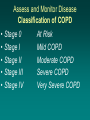
بسم هللا الرحمن الرحیم COPD Dr.Cheraghvandi Chronic Obstructive Pulmonary Disease (COPD): definition • GOLD (Global Initiative on Chronic Obstructive Lung Disease) definition: COPD is a progressive but preventable chronic disease most frequently caused by smoking COPD is characterized by: - a progressive airflow limitation, which is not fully reversible - a rapid decline in lung function - a local and systemic inflammatory process not responsive to corticosteroids Close to the Beltway but a World Apart COPD • Chronic obstructive pulmonary disease is a slowly progressive disease that is characterized by a gradual loss of lung function • COPD includes chronic bronchitis, chronic obstructive bronchitis, or emphysema, or combinations of these conditions Asthma • Asthma is a chronic inflammatory pulmonary disorder that is characterized by reversible obstruction of the airways Chronic Bronchitis • Inflammation of the main airway passages (bronchi) to the lungs, which results in the production of excess mucous, a reduction in the amount of airflow in and out of the lungs, and shortness of breath Chronic bronchitis • • • • Increase in the number of mucous cells Large amount of sputum Diffusion normal Hypercarbia due to deceased alveolar ventilation Emphysema • A respiratory disease characterized by breathlessness brought on by the enlargement, or overinflation of, the air sacs (alveoli) in the lungs Emphysema • What is it? • Destruction of alveolar walls-- below the bronchioles • Decreases surface area • Decreases area available for exchange • Increase resistance to pulmonary blood flow Emphysema cont... • • • • • • • Can lead to pulmonary hypertension Cor pulmonale = right heart failure Lungs can not recoil and air is trapped Residual lung capacity increases PO2 decreases over time Increased RBC Polycythemia-- high hematocrit Emphysema cont... • • • • • • • PCO2 increased Hypoxic drive Causes Complications of disease Pneumonia URI Dysrhythmias cancer Emphysema cont... • • • • Home drugs Bronchodilators Steroids Later-- oxygen Emphysema cont.. • • • • • • Assessment Weight loss-- thin Dyspnea esp on exertion Cough only in AM Barrel chest Tachypnea Emphysema cont.. • • • • Pink puffers Enlarged accessory muscles Clubbing of fingers Pursed lips-- prolonged expiration-- active now • Wheezing or rhonchi may or may not be present Chronic bronchitis • • • • • Assessment Overweight Blue bloaters Rhonchi RHF-- JVD, pedal edema Epidemiology • 20.3 million Americans report having asthma • 5,000 deaths annually from asthma • 12.1 million Americans reported being diagnosed with COPD • 119,000 deaths annually from COPD • COPD is the 4th leading cause of death in the U.S. Wayne McLaren…Former Marlboro Man Age 30…a robust young man Age 51…riding into the sunset % Change in Age Adjusted Death Rate US 1965-1998…gotta die of something US Leading Causes of Death 2001 The Real Story Etiology • Cause of asthma is unknown but many factors play a part: – Genetic factors: Asthma tends to run in the family – Environmental factors: pollen, dust, mold, tobacco smoke – Occupational exposure: chemicals and gases • Smoking is the leading cause of COPD followed by occupational exposures Clinical Features of Asthmatic Patients • General: intermittent wheezing, coughing, and breathlessness • During an attack: decreased peak flow, tachypnea, use of accessory muscles to breathe, hyperinflation or barrel chest, and prolonged inspiration Clinical Features of COPD Patients • Mild COPD: no abnormal signs, smokers cough, little or no breathlessness • Moderate COPD: breathlessness with/without wheezing, cough with/without sputum • Severe COPD: breathlessness on any exertion/at rest, wheeze and cough prominent, lung inflation usual, cyanosis, peripheral edema, and polycythemia in advanced disease Diagnosis • Spirometry – Breathing test which measures the amount and rate at which air can pass through the airways • Bronchodilator Reversibility Testing – Relaxing tightened muscles around the airways and opening up airways quickly to ease breathing • Other pulmonary function testing – Diffusion capacity • Chest X-ray • Arterial Blood Gas – Shows oxygen level in blood Medical Management of Asthmatic Patient • Limit exposure triggering agents • Medications such as: inhaled corticosteroids, inhaled beta2 adrenergic agonist, and cromolyn sodium Medical Management of COPD Patient • Smoking cessation and elimination of environmental pollutants • Palliative measure such as regular exercise, good nutrition, flu and pneumonia vaccines • Bronchodilators, corticosteroids, anticholinergics, and NSAIDs Dental Management of COPD Patient • • • • • • • Review history for concurrent heart disease Avoid treatment if upper respiratory tract infection is present Treat in upright position Avoid rubber dam in severe cases Use pulse oximetry (if pulse ox <91%, use low flow 2-3L/min) Avoid Nitrous oxide/oxygen in severe cases Avoid barbiturates, narcotics, antihistamines, and anticholinergics • If patient is on steroid regimen, supplement as needed • Drug interactions with COPD medication Other Sad Facts • Direct Cost 2002- 18 Billion • Indirect Costs- 14 Billion • In US 47 million still smoke – 28% males – 23% females • WHO: 1 billion smokers worldwide…to increase to 1.6 billion 2025. Increasing in lower income areas Objectives of COPD Management • Prevent Progression • Relieve symptoms • Improve exercise tolerance and general health status • Prevent and treat exacerbations and complications • Minimize treatment side effects Pathophysiology Simplified Bad Genes Breathe Noxious Crap COPD THE Guideline • Global Initiative for Chronic Obstructive Lung Disease (GOLD), World Health Organization (WHO), National Heart, Lung and Blood Institute (NHLBI) 4 Keys to Management • Assess and Monitor Disease • Reduce Risk Factors • Manage Stable COPD – Education – Med management – Non med management • Treat exacerbations Assess and Monitor Disease Classification of COPD • • • • • Stage 0 Stage I Stage II Stage III Stage IV At Risk Mild COPD Moderate COPD Severe COPD Very Severe COPD Stage 0 At Risk • Normal spirometry • +/- Chronic symptoms (cough, sputum, production) Stage I Mild COPD • FEV1/FVC <70% • FEV1 >80% predicted • With or without chronic symptoms (cough, sputum production) Stage II Moderate COPD • FEV1/FVC <70% • 50% <FEV1 <80% predicted • With or without chronic symptoms (cough, sputum production) Stage III Severe COPD • FEV1/FVC <70% • 30% <FEV1 <50% predicted • With or without chronic symptoms (cough, sputum production) Stage IV Very Severe COPD • FEV1/FVC <70% • FEV1 <30% predicted or FEV1 <50% predicted plus chronic respiratory failure GOLD Guideline in Japan Assess: Who Has Early Stages And Who Do You Test? • Test patients with: – chronic cough and sputum – exposure to risk factors – even if no dyspnea • Early Stage: – airflow limitation that is not fully reversible – with or without the presence of symptoms Assess for COPD: A Common Story • Cough – intermittent or daily – present throughout day- seldom only nocturnal • Sputum – Any pattern of chronic sputum production • Dyspnea – Progressive and Persistent – "increased effort to breathe" "heaviness" "air hunger" or "gasping" – Worse on exercise – Worse during respiratory infections • Exposure to risk factors – Tobacco smoke – Occupational dusts and chemicals – Smoke from home cooking and heating fuels Assess: Spirometry to Diagnose FEV1/FVC <70% and a postbronchodilator FEV1 <80% predicted confirms the presence of airflow limitation that is not fully reversible. Must have access to spirometry Assess: Medical History in Those With Established Disease • Exacerbations or hospitalizations? • Comorbidities that contribute to restriction of activity • Appropriateness of current medical treatments • Impact of disease on patient's life – limitation of activity – missed work and economic impact – effect on family routines – depression or anxiety • Social and family support • Possibilities for reducing risk factors, esp smoking Assess: Physical Examination • Rarely diagnostic in COPD • Physical signs of airflow limitation – rarely present until significant impairment of lung function – low sensitivity and specificity Assess: Measure Airflow Limitation • Patients with COPD typically show a decrease in both FEV1 and FVC • Postbronchodilator FEV1 <80% predicted + FEV1/FVC <70% confirms the presence of airflow limitation that is not fully reversible • FEV1/FVC <70% is an early sign of airflow limitation in patients whose FEV1 remains normal (>80% predicted). Assess: Additional Investigations > Stage II: Moderate COPD • Bronchodilator reversibility testing – – – – rule out asthma establish best attainable lung function gauge a patient's prognosis guide treatment decisions • Chest x-ray – seldom diagnostic unless obvious bullous disease – valuable in excluding alternative diagnoses – CT not routinely recommended Assess: Additional Investigations > Stage II: Moderate COPD • Arterial blood gas measurement – In advanced COPD: FEV1 <40% predicted or signs suggestive of respiratory failure or right heart failure – central cyanosis, ankle swelling, JVD – Respiratory failure • PaO2 < 60 mm Hg +/- PaCO2 >50 mm Hg • Alpha-1 antitrypsin deficiency screening – COPD at a young age – strong family history of the disease Differential Diagnosis • A major differential diagnosis is asthma • In some patients with chronic asthma, a clear distinction from COPD is not possible • In these cases, current management is similar to that of asthma • Other potential diagnoses are usually easier to distinguish from COPD COPD • • • • • Onset in mid-life Symptoms slowly progressive Long smoking history Dyspnea during exercise Largely irreversible airflow limitation Asthma • • • • Onset early in life (often childhood) Symptoms vary from day to day Symptoms at night/early morning Allergy, rhinitis, and/or eczema also present • Family history of asthma • Largely reversible airflow limitation Congestive Heart Failure • Fine basilar crackles on auscultation • Chest x-ray shows dilated heart, pulmonary edema • PFTs indicate restriction- not obstruction • BNP can help Other Diff Dx to Consider • Bronchiectasis – Large volumes of purulent sputum – bacterial infection – CXR/CT shows bronchial dilation, bronchial wall thickening • TB – History with the usual suspects • BOO and BOOP – nonsmokers – environmental exposures – CT on expiration shows hypodense areas Monitoring: This is a progressive disease • Lung function worsens over time- even with best care • Monitor symptoms and objective measures of airflow limitation to determine when to adjust therapy • Spirometry should be performed if there is a substantial increase in symptoms or a complication • ABG should be considered in all patients with an FEV1 <40% predicted or clinical signs of respiratory failure or right heart failure (JVD/edema) Reduce Risk Factors Reduce Risk Factors: Key Points • Reducting exposure to tobacco smoke, occupational dusts, and chemicals, and indoor and outdoor air pollutants • Smoking cessation is the single most effective -- and cost-effective -- intervention to reduce the risk of developing COPD and stop its progression (Evidence A) Reduce Risk Factors: Key Points • Brief tobacco dependence treatment is effective (Evidence A) • Every tobacco user should be offered at this treatment at every visit • Three types of counseling are especially effective: practical counseling, social support as part of treatment, and social support arranged outside of treatment (Evidence A) Reduce Risk Factors: Key Points • There are effective pharmacotherapies for tobacco dependence (Evidence A) • Add meds to counseling if necessary • Progression of many occupationally induced respiratory disorders can be reduced or controlled by reducing inhaled particles and gases (Evidence B) Maybe This Would be Better Than Drugs Manage Stable COPD Key Points 1 • Stepwise increase in treatment based on disease severity • Health education can play a role in improving skills, ability to cope with illness, and health status. It is effective in accomplishing certain goals, including smoking cessation (Evidence A). • None of the existing medications for COPD affects long-term decline in lung function that is the hallmark of this disease (Evidence A) • Pharmacotherapy for COPD is used to decrease symptoms and/or complications Therapy by Stage- Pretty Simple Manage Stable COPD Key Points 2 • Bronchodilators central to symptom management (Evidence A) • PRN or regular basis to reduce symptoms • Use beta2-agonist, anticholinergic, theophylline, or a combination of one or more of these drugs (Evidence A) • Regular treatment with LABs is slightly more effective and convenient than with SABs, but more expensive (Evidence A) • TECHNIQUE IS KEY • MDI BETTER THAN NEB IF USED CORRECTLY Manage Stable COPD Key Points 3 • Add inhaled steroids to bronchodilators for symptomatic COPD patients with an FEV1 <50% predicted (Stage III: Severe COPD and Stage IV Very Severe COPD) and repeated exacerbations (Evidence A) • Avoid chronic treatment with systemic steroids - unfavorable benefit-to-risk ratio (Evidence A Manage Stable COPD Key Points 3 • The long-term O2 with chronic respiratory failure increases survival (Evidence A) • Improves exercise tolerance • If hypercapnic titrate SpO2 to 88-90% • Walk your clinic patients if RA SpO2 OK Manage Stable COPD Key Points 4 • All COPD patients benefit from exercise training program • Improves both exercise tolerance and symptoms of dyspnea and fatigue (Evidence A) Medications Bronchodilators Beta2-agonists • Short-acting – Fenoterol – Salbutamol (albuterol) – Terbutaline • Long-acting – Formoterol – Salmeterol Bronchodilators Anticholinergics • Mode of Action – Cholinergic tone is only reversible component of COPD – Normal airway have small degree of vagal cholinergic tone • Short-acting – Ipratropium bromide – Oxitropium bromide • Long-acting – Tiotropium BronchodilatorsCombos and Methylxanthines • Combination beta2-agonists plus anticholinergic in one inhaler – Fenoterol/Ipratropium – Salbutamol/Ipratropium • Methylxanthines – Aminophylline (slow release preparations) – Theophylline (slow release preparations) – RARELY OF SIGNIFICNAT BENEFIT – LEVEL 8-12 mcg/ml Other Med Adjuncts? • Influenza vaccines significantly reduce serious illness and death (Evidence A) • Pneumococcal vaccine –OK to use but data lacking (Evidence B) • Antibiotics: other than treating infectious exacerbations- not recommended (Evidence A) • Mucolytic Agents: a few patients with viscous sputum may benefit but the widespread use cannot be recommended (Evidence D) • Antitussives: Cough, a troublesome symptom in COPD, has a protective role. Regular use of antitussives contraindicated (Evidence D) • Narcotics: The use of PO and IV opioids effective for dyspnea in advanced disease Therapy by Stage- Pretty Simple • “Make everything as simple as possible, but not one bit simpler” Einstein Manage Exacerbations • Do you admit? You and your patient decide….little guidance in the literature Manage Exacerbations 1 • Infection of tracheobronchial tree and air pollution are most common causes • Cause of about 1/3 of severe exacerbations cannot be identified Manage Exacerbations 2 (Evidence A) treatment Inhaled bronchodilators (beta2-agonists and/or anticholinergics) Systemic, preferably oral, glucocorticosteroids (Evidence B) Antibiotic treatment if signs of airway infection increased volume/change of color of sputum fever O2 of course….but caution with retainers Little evidence for Methyxanthines Manage Exacerbations 3 Noninvasive intermittent positive pressure ventilation (NIPPV) improves blood gases and pH, reduces in-hospital mortality, decreases the need for invasive mechanical ventilation and intubation, and decreases the length of hospital stay (Evidence A) BIPAP is Best! • Set FiO2, inspiratory (IPAP) and expiratory (EPAP) • Difference between IPAP and EPAP augments tidal volume and improves minute ventilation • CO2 gets blown off Best References • Stoller J. Acute Exacerbations of COPD, NEJM Mar 28, 2002 • Sutherland E. Management of COPD, NEJM June 24, 2004 • GOLD (Global Initiative for Chronic Obstructive Lung Disease) Executive Summary www.goldcopd.org • New….TORCH NEJM Feb 22, 2007 Questions? COPD - Pathogenesis Tobacco Smoke Host factors Chronic Inflammation* Anti-oxidants Anti-proteinases Oxidative Stress Proteinases Repair Mechanisms Emphysema Chronic Bronchitis *CD8+ T-lymphocytes Macrophages Neutrophils IL-8 and TNF COPD Therapy Prolong Life Smoking Cessation Oxygen Reduce exacerbations Pulmonary Rehabilitation • LVRS (selected patients) • Lung Transplantation • • • • Symptomatic • MDI Therapy – SA beta-2 agonists – LA beta-2 agonists – SA and LA Anticholinergics • Theophylline • Corticosteroids (inhaled or oral) • Combination Preparations – SABA and anticholinergic – LABA and corticosteroids Management of COPD Stage 0: At Risk Characteristics Treatment • Risk factors •Chronic symptoms - cough - sputum • No spirometric abnormalities Recommended •Adjust risk factors •Immunizations Management of COPD Stage I: Mild COPD Characteristics Treatment • FEV1/FVC < 70 % • FEV1 > 80 % predicted • With or without symptoms Recommended • Short-acting bronchodilator as needed Management of COPD Stage II: Moderate COPD Characteristics Treatment •FEV1/FVC < 70% •50% < FEV1< 80% predicted •With or without symptoms Recommended •Treatment with one or more long-acting bronchodilators •Rehabilitation Management of COPD Stage III: Severe COPD Characteristics Treatment •FEV1/FVC < 70% •30% < FEV1 < 50% predicted •With or without symptoms Recommended •Treatment with one or more long-acting bronchodilators •Rehabilitation •Inhaled glucocorticosteroids if repeated exacerbations (>3/year) Management of COPD Stage IV: Very Severe COPD Characteristics Treatment •FEV1/FVC < 70% •FEV1 < 30% predicted or presence of respiratory failure or right heart failure Recommended •Treatment with one or more long-acting bronchodilators •Inhaled glucocorticosteroids if repeated exacerbations (>3/year) •Treatment of complications •Rehabilitation •Long-term oxygen therapy if respiratory failure •Consider surgical options Bronchodilator Therapy Some General Principles • Inhaled therapy (with spacer) preferred • Long-acting preparations more convenient • Combined preparations improve effectiveness and decrease risk of side effects – Ipratroprium-albuterol – Fluticasone-salmeterol – Budesonide-formoterol • MDI almost always as effective as nebulizers (in equal doses) Effectiveness of BronchodilatorTherapy? • FEV1 does not always correlate with symptoms – Concept of “dynamic hyperinflation” in COPD • Quality of life issues are important – Chronic fatigue – Depression – Physical immobility – Dyspnea COPD - Surgical Options • Giant Bullous Disease – Consider bullectomy if see normal lung compression • Lung Volume Reduction Surgery* – FEV1 (<20% pred) plus diffuse emphysema or Dlco<20% pred = high risk of surgical death – Upper lobe emphysema and low exercise capacity = decreased mortality, increased exercise and QOL • Lung Transplantation – FEV1<25% predicted, younger patient – 3-5 year mortality 55% *NETT Research Group. N Eng J Med 348:2059, 2003 COPD Exacerbation Definition Elements • Worsening dyspnea • Increased sputum purulence • Increase in sputum volume Severity • Severe - all 3 elements • Moderate - 2 elements • Mild - 1 element plus: Modified from Anthonisen et al. Ann Int Med 106:196, 1987 • URI in past 5 days • Fever without apparent cause • Increased wheezing or cough • Increase (+20%) COPD Exacerbation Pathophysiology - Current Hypothesis Chronic Inflammation Viral Infection Unknown 20% 25% Bacterial Infection 50% Acute Inflammation Exacerbation Air Pollution 5% Therapy of COPD Exacerbation Guidelines Variable Diagnostic ACCP-ACP CXR for admissions GOLD CXR, EKG, ABG, sputum culture, lytes, cbc Bronchodila Ipratroprium, add B2 tors agonist. No methylxanthine B2 agonist, add ipratroprium. Yes methylxanthine Delivery system None preferred Not discussed Antibiotics Yes, in selected (severe). Duration Ann Int Med 134:595, 2001 unclear Yes, with purulence, Rx local sensitivities http:/www.goldcopd.com COPD Exacerbation Effects on Lung Function Decline Infrequent Frequent • 109 pts (mean FEV1 = 1.0 L over 4 years • Frequent exacerbators: – faster decline in PEFR and FEV1 – more chronic symptoms (dyspnea, wheeze) – no differences in PaO2 or PaCO2 Conclusion: Frequent exacerbations accelerate decline in lung function Donaldson et al. Thorax 57:847, 2002 Therapy of COPD Exacerbation Guidelines Variabl ACCP-ACP e GOLD Steroids Yes, for up to two weeks Yes, oral or IV for 10-14 days Oxygen Yes Yes - target PaO2 60 torr or Sat of 90% with ABG check Chest PT No Maybe - for atelectasis or sputum control Mucokinet No ics Ann Int Med 134:595, 2001 Not discussed http:/www.goldcopd.com Therapy of COPD Exacerbation Guidelines Variable Mechanical Ventilation ACCP-ACP GOLD Yes - use NIPPV in Yes if ≥2 of: severe Severe dyspnea, exacerbation access. muscle or paradox, pH <7.35 and PCO2 >45, RR>25 LMWH, fluids, diet Other Ann Int Med 134:595, 2001 http:/www.goldcopd.com COPD Therapy - New Horizons • Newer anti-inflammatory agents – Matrix metalloproteinase inhibitors – Specific phosphodiesterase (PDE4) inhibitors • Cilomilast • Rofumilast • Piklanilast • Anabolic steroids • Repair agents – Retinoic acid • Long-acting anti-muscarinic agents – tiotropium Tiotropium Specific M1 and M3 Muscarinic Blockade • 470 patients - stable COPD • 3 month, randomized, double blind, once daily tiotropium vs. placebo Conclusions: Increased FEV1 and FVC No tachyphylaxis Decreased rescue albuterol Decreased wheezing, SOB Dry mouthCasaburi in 9.3% et al. CHEST 118:1294, 2000 Tiatroprium Specific M1 and M3 Muscarinic Blockade • 1207 patients, double blind, randomized trial, • qd tiotropium vs. bid salmeterol vs. placebo Conclusions: Tiotropium Fewer exacerbations Increased time to first exacerbation Fewer admissions Increased QOL Brusasco et al. Thorax 58:399:2003 Lung Volumes in Obstructive Disease TLC Volume Room to Breathe TLC FRC Room to Breathe FRC RV RV Normal COPD