Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
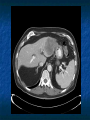
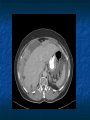
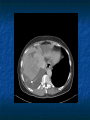
Cancer Pain Management 101 Sarah Beth Harrington, MD Internal Medicine Noon Conference November 30, 2007 Objectives 1. 2. 3. 4. Review primary causes of cancer-related pain. Recognize effects of pain on cancer patients. Understand basic concepts of pharmacologic management techniques with opioids and non-opioids. Discuss non-pharmacologic techniques in cancer pain management. Causes of Cancer-Related Pain Tumor / Mass effect Post-chemotherapy Post-radiation Post-surgical Somatic Pain Tumor / Mass effect Musculoskeletal Dull, sharp, localized Visceral Pain infiltration, compression, extension, or stretching of the thoracic, abdominal, or pelvic viscera pressure, deep, squeezing not well-localized referred Neuropathic Pain CA compressing or infiltrating nerves/nerve roots/blood supply to nerve Nerve damage from treatments Shooting, sharp, burning, “pins & needles” Cranial neuropathies Post-herpetic neuropathies Brachial plexus neuropathies Post-radiation Neuropathic Pain Chemotherapy-induced neuropathies Cisplatin, Oxaliplatin Paclitaxil, Thalidomide Vincristine, Vinblastine Surgical Neuropathies Phantom limb pain Post-mastectomy syndrome Post-thoracotomy syndrome Summary Causes Descriptors Tumor size may not correlate with pain intensity Physiological effects of Pain Increased catabolic demands: poor wound healing, weakness, muscle breakdown Decreased limb movement: increased risk of DVT/PE Respiratory effects: shallow breathing, tachypnea, cough suppression increasing risk of pneumonia and atelectasis Increased sodium and water retention (renal) Decreased gastrointestinal mobility Tachycardia and elevated blood pressure Psychological effects of Pain Negative emotions: anxiety, depression Sleep deprivation Existential suffering Immunological effects of Pain Decrease natural killer cell counts Effects on other lymphocytes not yet defined What Does Pain Mean to Patients? Poor prognosis or impending death Decreased autonomy Particularly when pain worsens Impaired physical and social function Decreased enjoyment and quality of life Challenges to dignity Threat of increased physical suffering Principles of Assessment Ask Dispel myths/ misunderstandings Believe the patient Assess and REASSESS Use methods appropriate to cognitive status and context Assess intensity, relief, mood, and side effects Include the family Patient Pain History Site(s) of pain/radiation? Quality? Severity of pain? Onset / duration What aggravates or relieves pain? Impact on sleep, mood, activity? Effectiveness of medication? Pharmacologic Management WHO Ladder Non-opioid therapy / Co-analgesics Opioids WHO Ladder Non-Opioids NSAIDS Acetaminophen Topicals Lidocaine, Capsaicin Practice Points: Mild pain “ceiling” effect Start at lowest effective dose Review pt’s underlying medical illnesses Adjuvants Antidepressants TCAs for neuropathic pain Anticonvulsants Corticosteroids Neuroleptics Alpha2 – agonists Benzodiazepines Antispasmodics Muscle relaxants NMDA-blockers Systemic local anesthetics Adjuvants Bone pain Bisphosphonates Calcitonin Pain from malignant bowel obstruction Steroids Octreotide Anticholinergics Practice Points: Choose adjuvant carefully (risk:benefit) Start low and titrate gradually Avoid initiating several adjuvants concurrently Opioids Step 2 opioids Step 3 opioids Codeine, Oxycodone, tramadol, hydrocodone Oxycodone, morphine, dilaudid, fentanyl, methadone AVOID: meperidine, agonists/antagonists, combo agents, propoxyphene Opioids Practice Points: If pain constant/chronic – use long-acting opioids with short-acting for breakthrough Breakthrough dose - 10-20% of total daily dose Assess pt’s clinical and financial situation before prescribing Mr. Smith 58 yo AAM with chronic bone pain from met. prostate CA. Prescribed Percocet (5/325) in the ER 2 weeks ago and is now in your clinic for f/u. Pain is well controlled, but tends to recur ~1 hr before the next dose. He takes 2 Percocets q4hrs around the clock, even at night. Mr. Smith 10mg oxycodone 6 times/day = 60mg oxycodone in 24 hrs Equivalent SR oxycodone= Oxycontin 30mg q12h Rescue dose – 10% (60mg) = 6 mg 20% (60mg) = 12mg ANSWER: Oxycontin 30mg q12h with Oxycodone 5-10mg q4h prn Changing opioids Intolerable side effects, method of delivery, cost Practice points Incomplete cross-tolerance with different opioids Start new opioid at ½-⅔ of equianalgesic dose Ms. B 50 yo breast CA survivor with chronic neuropathic pain from her mastectomy. She currently is well-controlled on a 75 mcg/hr fentanyl patch. She lost her job and can no longer afford the patch. You want to switch her to MS Contin with MS IR for breakthrough. What dose? Ms. B 75 mcg/hr fentanyl patch 75 mg po morphine/day 25 mcg/hr fentanyl patch ⅔ (225 mg) ≈ 150 mg morphine/day 75 mg MS Contin q12h Breakthrough - 10% 150 = 15 mg 20% 150 = 30 mg MS Contin 75 mg q12h with 15-30mg MS IR prn 225 mg po morphine/day Parenteral Opioids 1mg IV morphine = 3 mg po morphine 1mg IV dilaudid = 4-5 po dilaudid Rapid escalation, assess pt’s pain needs (PCA), fast-acting PCA tips How to order – IV PCA dose q6 min, basal, bolus q1hr prn If pt on a long-acting opioid – can continue po or convert all to IV basal (DO NOT STOP) REASSESS, REASSESS, REASSESS Double PCA and bolus dose if pain score worse or >50% original SQ option – morphine & dilaudid – higher concentration; PCA dose q15 min Opioid adverse effects Common Uncommon Constipation Dry mouth Nausea / vomiting Sedation Sweats Bad dreams / hallucinations Dysphoria / delirium Myoclonus / seizures Pruritus / urticaria Respiratory depression Urinary retention Radiation / Nuclear Medicine Radiation – curative treatment, adjuvant, palliative Bone metastases – pain response rate 3560%, duration 12-24 wks Strontium-89 Non-Pharmacologic Management Acupuncture Yoga Guided imagery Cold/heat Massage Vibration TENS units Exercise programs Hypnosis Counseling Music Pet therapy Cancer Pain Emergencies (a.k.a. things you can’t miss) Cord Compression Withdrawal Bone Mets/Impending Fractures WHO Ladder What about the 20%!? Have the opioids been titrated aggressively? Is the pain neuropathic? Has a true pain assessment been accomplished? Have you examined the patient? Is the patient receiving their medication? Is the medication schedule and route appropriate? Modified WHO Analgesic Ladder Quality of Life Invasive treatments Proposed 4th Step Opioid Delivery Pain persisting or increasing Step 3 Opioid for moderate to severe pain ±Nonopioid ±Adjuvant Pain persisting or increasing The WHO Ladder Step 2 Opioid for mild to moderate pain ±Nonopioid ±Adjuvant Pain persisting or increasing Step 1 ±Nonopioid ±Adjuvant Pain Deer, et al., 1999 Cancer pain management 201 Interventions Blocks Epidural Intrathecal pain pumps Lidocaine infusion Ketamine Sedation Interventions Palliative surgery Nerve Blocks Kyphoplasty/Vertebroplasty Epidural Intrathecal pain pumps Celiac Plexus Block Celiac Plexus Block Kyphoplasty/Vertebroplasty Kyphoplasty/Vertebroplasty Intrathecal Pain Pumps Intrathecal Pain Pumps Conclusion Cancer pain can be from the cancer itself, or from cancer-related treatments Can be somatic, visceral, or neuropathic Negative effects of cancer-related pain can effect QOL, mortality Ask the patient about pain and REASSESS! Conclusion Choose non-opioid / adjuvants carefully paying close attention to side effect profile Use WHO ladder guidelines when titrating pain medications Use long-acting opioids for chronic cancer pain Recognize “4th step” in WHO ladder and utilize your multidisciplinary resources Palliative Care Service N4N – 6-1295 Fellows: Dr. Paresh Patel, Dr. Keith Swetz NPs – Pat Coyne and Bart Bobb Questions?