Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
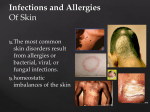
Zoya Minasyan, RN, MSN-Edu A localized injury to the skin and/or underlying tissue due to pressure with or without shear/friction Most common sites ▪ Sacrum ▪ Heels Advanced age Anemia Contractures Diabetes mellitus Elevated body temperature Immobility Impaired circulation Incontinence Low diastolic blood pressure (<60 mm Hg) Mental deterioration Neurologic disorders Obesity Pain Prolonged surgery Vascular disease •Ulcers are graded or staged according to deepest level of tissue damage • A pressure ulcer may also present as a blood-filled blister. • Stable (dry, adherent, intact) eschar on the heels serves as “the body’s natural (biologic) cover” and should not be removed. Intact skin with non-blanchable redness Possible indicators—Skin temperature, tissue consistency, pain May appear with red, blue, or purple hues in darker skin tones Partial-thickness loss of dermis Shallow open ulcer with red pink wound bed Presents as an intact or ruptured serum-filled blister Full-thickness skin loss involving damage or necrosis of subcutaneous tissue that may extend down to, but not through, underlying fascia Presents as a deep crater with possible undermining of adjacent tissue Depth of ulcer varies by anatomic location. Full-thickness loss can extend to muscle, bone, or supporting structures. Bone, tendon, or muscle may be visible or palpable. Undermining and tunneling may also occur. Signs of infection Leukocytosis Fever Increased ulcer size, odor, or drainage Necrotic tissue PainMost common complications Recurrence Cellulitis (is a inflammation of connective tissue with severe inflammation of dermal and subcutaneous layers of the skin) Chronic infection Osteomyelitis (an infection of the bone or bone marrow) Assess pressure ulcer risk on admission and at periodic intervals based on care setting and patient’s condition. Use risk assessment tools such as the Braden scale for systematic skin inspection. Look for areas of skin darker (purplish, brownish, bluish) than surrounding skin. Use natural or halogen light for accurate assessment (fluorescent light casts a blue color that can skew results). Assess skin temperature using your hand. An ulceration may feel warm initially, then become cooler. Touch the skin to feel its consistency. Boggy or edematous tissue may indicate a stage I pressure ulcer. Ask about pain or an itchy sensation. Overall goals No deterioration Reduce contributing factors Not develop an infection Healing and no recurrence Prevention is the best treatment. Identify risk factors and implement prevention strategies. Remove excessive moisture. Avoid massage over bony prominences. Turn every 1 or 2 hours (with care to avoid shearing). Use lift sheets. Position with pillows or elbow and heel protectors. Use specialty beds. Cleanse skin if incontinence occurs. Use pads or briefs that are absorbent. Caloric intake elevated to 30 to 35 cal/kg/day or 1.25 to 1.50 g protein/kg/day Supplements, enteral, or parenteral feedings may be necessary. Document and describe size, stage, location, exudate, infection, pain, and tissue appearance. Keep ulcer bed moist. Cleanse with nontoxic solutions. Debride. Use adhesive membrane, ointment, or wound dressing. Verify good nutrition. Teach self-care and signs of breakdown. Initiate specialty services. Skin grafts Microscopic view of the skin in longitudinal section. Structures Epidermis Dermis Subcutaneous tissue Irregular pigmentation and keratoses occur on sun-damaged skin on forehead. Normal Physical Assessment of Integumentary System. Subjective Data Important health information ▪ Past health history ▪ Medications ▪ Surgery or other treatments Functional health patterns ▪ ▪ ▪ ▪ ▪ ▪ ▪ ▪ ▪ ▪ ▪ Health perception–health management pattern Nutritional-metabolic pattern Elimination pattern Activity-exercise pattern Sleep-rest pattern Cognitive-perceptual pattern Self-perception–self-concept pattern Role-relationship pattern Sexuality-reproductive pattern Coping–stress tolerance pattern Value-belief pattern Objective Data: Physical examination-Inspection, Palpation Intertrigo. Rash in body folds with Candida infection. Vitiligo. Total loss of pigment in the affected area. Naevus of Ota. Flat gray to blue pigmentation in the upper trigeminal area, which is more common in dark-skinned individuals. Traction alopecia. Hair loss in scalp due to prolonged tension from hair rollers and braiding and straightening combs. Basal cell carcinoma. Rolled, well-defined border and central erosion. Squamous cell carcinoma of the finger. Breslow measurement of tumor thickness. A, Thin (0.08° mm) superficial spreading melanoma good prognosis. B, Thick nodular melanoma with lymph node involvement, poor prognosis. Dysplastic nevus. Irregular border and color. Herpes zoster (shingles) on the anterior chest, confined to one dermatome. Plantar wart. A, Keratotic lesion. B, After excision. Candidiasis in interdigital cleft. Occurs in workers whose constantly wet hands are not dried often. Tinea unguium (onychomycosis). Fungal infection of toenails. Crumbly, discolored, and thickened nails. Scabies infestation on hand. Psoriasis. Characteristic inflammation and scaling. Acne vulgaris. Papules and pustules. Seborrheic keratoses. Deeply pigmented, rough and warty surface. Fig. 24-17. Curettage. The superficial growth is removed by a gentle scoping technique. Collaborative Therapy, continued Drug therapy ▪ Antibiotics ▪ Corticosteroids ▪ Antihistamines ▪ Topical fluorouracil ▪ Immunomodulators Diagnostic and Surgical Therapy Skin scraping Electrodesiccation and electrocoagulation Curettage Radiation therapy Laser technology Cryosurgery Punch biopsy. A, Removal of skin for diagnostic purposes. B, Specimen obtained. A, Removal of melanoma by Mohs, surgery. B, Following plastic surgery using a skin flap to repair defect. Ambulatory and Home Care Wet dressings Baths Topical medications Control of pruritus Prevention of spread Face-lift. A, Preoperative. B, Postoperative. Elective Surgery Laser surgery Face lift Liposuction