Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
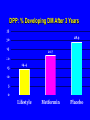
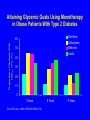
DIABETES MANAGEMENT 2006: INTEGRATING NEW MEDICINES AND NEW DEVICES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus in the US: Health Impact of the Disease 6th leading cause of death Renal failure* Blindness* Amputation* Life expectancy -5 to 10 yr Diabetes Cardiovascular disease 2x to 4x Nerve damage in 60% to 70% of patients *Diabetes is the no. 1 cause of renal failure, new blindness, and nontraumatic amputations Diabetes Mellitus: U.S. Impact DIABETES 16.7 Million (8.3%) IFG 12.3 Million (6.3%) ~1 Million Type 1 ~16 Million Type 2 2/3 Diagnosed 1/3 Undiagnosed (4.9 Million) TOTAL: 29 Million (14.4%) Screening for Diabetes ADA: >45, especially if BMI >25. <45 if overweight and have risk factor for DM (inactive, FH, high risk ethnicity, baby >9 lb, HTN, low HDL or high TG, PCOS, vascular disease). Screen with FPG or 2-h OGTT Diabetes Care, 2006 USPSTF: Insufficient evidence to recommend for or against. However, recommend screening in adults with hypertension and lipid disorders Ann Intern Med, 2003 Diagnosis of Diabetes Two measures of any of the following: Random glucose: 200 mg/dl with symptoms (poly’s, weight loss) Fasting glucose: 126 mg/dl 2-hr glucose: 200 mg/dl during OGTT Diabetes Care 2006 HbA1C for Screening ? • HbA1c 2SD above mean has sensitivity of 66 % and specificity of 98 % and compares favorably to FPG • Different nondiabetic reference ranges due to different glycated hemoglobin fractions • Precision and accuracy may not be sufficient in all labs • Affected by hemoglobinopathies, anemia, transfusions, uremia, pregnancy Diagnosis of Pre-Diabetes Two measures of any of the following: Fasting glucose 100 - 125 mg/dl 2-hr glucose 140 - 199 mg/dl during OGTT % developing Diabetes DPP: % Developing DM After 3 Years 35 28.9 30 25 21.7 20 15 14.4 10 5 0 Lifestyle Metformin Placebo Prevention of Type 2 DM: RCTs Trial Description Results (RR) Da Qing1 Diet &/or exercise 31 to 46% Finnish Prevention Study (FPS)2 Intensive lifestyle 58 % Diabetes Prevention Program (DPP)3 Meformin Lifestyle 31 % 58 % STOP- NIDDM4 Acarbose 25 % TRIPOD5 Troglitazone 55 % Recommendations for Adults Glycemic Control A1C: <7.0 Preprandial: 90-130 mg/dl Postprandial: <180 mg/dl Blood Pressure: <130/80 mmHg Lipids LDL: <100 mg/dl TG: <150 mg/dl HDL: >40 mg/dl ADA Diabetes Care 2006 Treatment of Type 2 Diabetes Step 1: Step 2: Step 3: Step 4: Step 5: Step 6: Lifestyle Changes Oral Monotherapy Combination Oral Therapy Oral Therapy plus Insulin Insulin Alone Insulin plus Thiazolidinedione/Metformin Target metabolic values need to be individualized Attaining Glycemic Goals Using Monotherapy in Obese Patients With Type 2 Diabetes Diet Alone Sulfonylurea Metformin Insulin Proportion of Patients With HbA1c <7% (%) 60 50 40 30 20 10 0 3 Years Turner RC et al. JAMA. 1999;281:2005-2012. 6 Years 9 Years Treatment of Type 2 Diabetes Acarbose/ Miglitol Delay digestion of carbohydrates SFUs/Insulin Metformin Decrease Hepatic Glucose Output Improved Glycemic Control Increase Insulin Secretion Decrease insulin Thiazolidinediones resistance Generic Oral Hypoglycemic Slide Change from Drug A to B, C, or D Add Drug A to B, or B to A HgA1c Add Drug C Add Drug D Time Adding Instead of Switching Continue glyburide Switch to metformin Change in Mean HbA1c (%) 1 Glyburide+ metformin +0.2% 0 * –1 –0.4% * * * –1.7% –2 –3 0 9 13 17 21 Treatment (wk) 25 29 DeFronzo, et al. N Engl J Med. 1995;333:541-549, 5-2 Oral Agent “Failure” Why does this occur? Changing HbA1c goals Compliance, side effects Wrong diagnosis (LADA--latent autoimmune diabetes in adults 10%) Stress, diabetogenic medications Natural progression of the disease Natural History of Type 2 Diabetes Obesity Glucose (mg/dL) IFG* Diabetes 350 300 250 200 150 100 50 Uncontrolled hyperglycemia Post-meal Glucose Fasting Glucose 250 200 Relative 150 Function 100 (%) 50 0 Insulin Resistance Insulin Level` Beta-cell failure -10 *IFG = impaired fasting glucose -5 0 5 10 Years of Diabetes 15 20 25 30 Natural History of Type 2 Diabetes Thiazolidinedione - Biguanide Lifestyle Glucose (mg/dL) Relative Function (%) 350 300 250 200 150 100 50 250 200 150 100 50 0 Insulin SU Post-meal Glucose Fasting Glucose Insulin Resistance Insulin Level Beta-cell failure -10 -5 0 5 10 15 Years of Diabetes 20 25 30 Insulin Plus Oral Agents Introduction of insulin – Bedtime – Intermediate/Long-acting insulins • NPH, UL, glargine • 10 units – Self-monitoring of blood glucose (hypoglycemia education) Insulin plus other oral agent combinations (maintain effect on insulin sensitivity) When to go to > 1 shot per day HgA1c >7 Glucose in AM at goal but g lucose before dinner >140 Options Add premeal lispro/aspart Add bid premixed insulin – 70/30, 75/25 Questions Continue metformin ? Sulfonylurea, ? Thiazolidinedione Function of Insulin in Regimens Meal coverage (carbohydrates) Basal insulin Correction of high blood sugar More Options Insulins – Insulin Lispro (Humalog®) ‘96 – Insulin Aspart (Novolog®) 9/00 – Humalog ® Mix 75/25 1/00 – Insulin Glargine (Lantus®) 4/00 – Novolog ® Mix 70/30 5/02 – Insulin Glulisine (Apidra®) 4/04 – Insulin Detemir (Levemir®) 6/05 – Insulin delivery devices and glucose meters Insulin Pharmacokinetics Type of Insulin Short-acting Regular Lispro/Aspart/ Glulisine Onset Peak ½-1hr 2-4hr <15 min 1-2 hr Duration Appearance 6-8hr 3-5hr clear clear Intermediate-acting NPH/Lente* 1-2hr 6-10hr 12+hr cloudy Long-acting Ultralente* Detemir Glargine 4-6hr 1 hr 1.5hr 18hr flat flat cloudy clear clear 24+hr 12-24hr 24hr On July 6, 2005 Lilly announced Lente and Ultralente will no longer be available in 2006. Short-acting Insulin Analogues: Lispro and Aspart Plasma Insulin (pmol/L) 400 Lispro 350 300 250 200 150 100 50 0 0 glulisine Regular Human 30 Meal SC injection 60 90 120 150 180 210 240 Time (min) Plasma Insulin (pmol/L) Plasma Insulin Profiles 500 Aspart 450 400 350 300 250 200 150 Regular 100 Human 50 0 0 50 100 150 200 Time (min) 250 300 Meal SC injection Heinemann, et al. Diabet Med. 1996;13:625-629; Mudaliar, et al. Diabetes Care. 1999;22:1501-1506. 6-28 Rapid-Acting Insulins Advantages Disadvantages • Flexibility--given immediately before or after meals • Caution with adequate CHO intake (if < than predicted, susceptible to hypoglycemia • Postprandial control-better match with glucose peak • Cost/insurance coverage • Limited duration so less overlap with subsequent injections Activity Profile in Type 1 Diabetes Glucose Utilization Rate (mg/kg/min) Lepore et al. Diabetes 1999;48(suppl 1):A97. Abst 416; Study 1015 (Hourly Mean Values) 6 5 Insulin Glargine 4 3 2 1 0 0 10 Time (h) after sc injection 20 30 = End of observation period Type 2 Diabetes: Unanswered Questions When should insulin be started? What insulin should you use in Type 2? What insulin regimen is best? Which, if any, oral agents should be continued? Insulin tactics Minimize weight gain – metformin Minimize risk of hypoglycemia – insulin analogs, optimize self management skills Minimize insulin resistance – thiazolidinediones and metformin Use oral agents to limit number of injections More Options Incretin mimetics Exenatide (Byetta ®) 4/05 Amylinomimetics (amylin analog) Pramlintide (Symlin ®) 3/05 Incretins in Type 2 DM Gut hormones released postprandially Oral glucose elicits greater insulin response than IV glucose; “incretin effect” accounts for 50-70% of insulin response to oral glucose 2 main gut incretins – Glucose-dependent insulinotropic polypeptide (GIP) • Released by K cells in duodenum – Glucagon-like peptide-1 (GLP-1) • Released by L cells in small intestines • Levels are diminished in type 2 DM post-meal Incretins in Type 2 DM (cont) Rapidly degraded by dipeptidyl peptidase IV (DPP-IV) • GLP-1 analogs; “incretin mimetics” – Liraglutide (free fatty acid added to bind to albumin; injected daily) – Exenatide • DPP-IV inhibitors (oral) Actions of GLP-1 Insulin secretion (Insulinotropic effects) – – – – – – Potentiates glucose-induced insulin secretion Enhances all steps of insulin biosynthesis Upregulates insulin gene expression Upregulates genes needed for beta-cell function ( Stimulates beta cell proliferation Promotes differentiation of beta cells from progenitor cells Inhibits glucagon secretion (Glucostatic effect) Slows gastric emptying Inhibits appetite and food intake Exenatide (Byetta) Synthetic Exendin-4, or exenatide Exendin-4 originally isolated from Gila monster’s (Heloderma suspectum) saliva; lizard in Arizona Analog of GLP-1 – 39 amino acid peptide – >50% overlap with human GLP-1 Resistant to DPP-IV degradation Similar binding affinity at GLP-1 receptors Exenatide (Byetta) Indications: adults with type 2 DM who are taking metformin, sulfonylurea or combination Peak concentration post injection achieved in 2.1 hr (injected SQ twice daily within 60 minutes of meal) Metabolized primarily by kidneys Not recommended in Clcr <30 ml/min OK in hepatic impairment Exenatide: BG Effects Lowers post-prandial BG – Restores first-phase insulin response – Slows gastric emptying – Lowers post-prandial glucagon ( hepatic glucose output) – food intake Lowers A1C Clinical Data: Exenatide 3 large, 30 week clinical trials (randomized, doubleblind, placebo-controlled) in patients with type 2 DM • On SFU: Buse et al. Diabetes Care. 2004;27:2628-35 • On SFU & metformin: Kendall DM et al. Diabetes Care. 2005;28:1083-91. • On metformin: DeFronzo RA et al. Diabetes Care. 2005;28:1092-1100 Placebo BID 5 mcg exenatide BID 10 mcg exenatide BID ITT 483 480 483 Age (y) 55 55 55 BMI 34 33 34 A1C 8.5 8.4 8.5 8 8 7 Duration of DM A1C (%) Effect (change from baseline) Placebo BID 5 mcg exenatide BID 10 mcg exenatide BID MET 0.1 -0.4 -0.8 SFU 0.1 -0.5 -0.9 MET+SFU 0.2 -0.6 -0.8 Changes in A1C from baseline vs placebo statistically significant Effect on FBG less pronounced: 6-9 mg/dl (5 mcg dose); 10 mg/dl (10 mcg dose) PPG 60% (5 mcg dose) & 90% (10 mcg dose) Weight (change from baseline) & Hypoglycemia Placebo BID 5 mcg exenatide BID 10 mcg exenatide BID Weight (kg) -1.4 -3.1 -4.2 Hypoglycemia (%) MET SFU MET + SFU 5.3 3.3 1.26 4.5 14.4 19.2 5.3 35.7 27.8 Open-label extension study to 90 weeks: persistence in weight loss and A1C Exenatide Dosing Start 5 mcg SQ BID before morning and evening meal When added to SFU, lower dose of SFU After 1 month, can increase to 10 mcg SQ BID Available in prefilled pen Must be continuously stored refrigerated at 36-46°F For oral medications dependent on threshold concentrations or rapid onset, take them 1 hour before Side Effects GI – Nausea (44% vs 18% with placebo); incidence lessens over time; 3% dropout rate due to nausea – Vomiting (13% vs 4%) – Diarrhea (13% vs 6%) Headache (9% vs 6%) Hypoglycemia (see previous slide) New Options for Insulin Delivery Durable Insulin Pens Use replaceable insulin cartridge Use dial mechanism for dose NovoPen® 3 – Maximum dosage: 70 units – 1 unit increment – metal material NovoPen ® Junior – Maximum dosage: 35 units – ½ unit increment BD™ Pen and Pen Mini – 1.5 cc cartridge – Maximum dosage: 30 or 15 units Innovo® & InDuo™ InDuo: Integrates two daily activities combined into one device – Blood glucose monitoring (OneTouch® Ultra® meter) and Insulin Delivery Device (Innovo) – Supports an acceptance and understanding of the link between SMBG and insulin therapy – Device serves as a constant reminder to test whenever the patient injects Memory function stores the time elapsed & amount of last insulin dose Uses 3 cc cartridge Maximum dosage: 70 units; 1 unit increments OptiClik FDA approved 8/04 Reusable pen for Lantus & Apidra 1-unit increments; takes only BD pen needles Supplied to physicians; not available in pharmacies www.opticlik.com Disposable/Prefilled Insulin Pens Hold 3 cc insulin Discard when finished Use dial mechanism for dose; need to prime (“air shot”) Novolin® InnoLet® – Clock-like dial (egg timer-like) with large scale numbers; audible clicks – large grip and ergonomic shape that allows alternative grips, easy-to-push large button and support shoulder – Maximum dose: 50 units – 1 unit increments Regular, NPH and 70/30 insulin only Disposable/Prefilled Insulin Pens, cont. Novo Nordisk FlexPen ® (Novolog ®, Novolog ® Mix 70/30): up to 60 units; 1 unit increments Eli Lilly pens (Humalog ®,Humalog ® Mix 75/25™, NPH, 70/30): up to 60 units; 1 unit increments Needles Pen Needles BD – 29 G: ½” (12.7mm) – 31 G: 3/16” (5 mm) or 5/16” (8 mm) Novo Nordisk – NovoFine® – 30 gauge x 1/3” (8mm) – 31 gauge x ¼” (6mm) Caution with obese patients if use shorter needles Syringes: 1/3, ½, 1 cc Several times enlarged NovoFine® 30 [30 gauge x 1/3” (8mm)] Disposable Needle Alternate Testing Sites Alternative Site Testing: Cons Lag time of 5-30 minute between forearm & finger – blood flow to finger is 3-5 x faster than arm – significant when BG changing rapidly When not to use (use fingers) – – – – BG rapidly changing suspect low BG hypoglycemic unawareness within 1-2 hours after meals Bruising at site Other Methods of SMBG Continuous ambulatory blood glucose monitoring – CGMS (Continuous Glucose Monitoring System) System Gold™ • Medtronic MiniMed • 72-hour; BG recorded q5min – 24-hour glucose patterns – detect unrecognized hypoglycemia – Requires HCP support Noninvasive: GlucoWatch G2 Biographer – Cygnus – Requires a prescription Self-Monitoring of Blood Glucose (SMBG) - ADA Recommendations Type 1 Diabetes : 3 x daily Type 2 Diabetes: optimal frequency and timing not known; “sufficient to facilitate reaching glucose goals” Postprandial BG may be necessary to reach A1C goals and/or reduce risk of hypoglycemia Self-management training: how to use the data to adjust food intake, exercise or pharmacologic therapy Diabetes Care 2006 Self-Monitoring:Outcomes Improve overall control: Best studies: HbA1c 0.7% lower in type 1 HbA1c 0.6% lower in type 2 Meta-analysis HbA1c 0.25% lower Other Emerging Therapies Pharmacologic – PPAR/PPAR dual agonists • Muraglitazar (Pargluva; Advisory committee met 9/9/05; recommended approval) • Tesaglitazar (Galida) – Alternative insulin dosage forms (IH, buccal; transdermal; nasal) • Inhaled insulin, Exubera • Islet cell transplants – Rimonabant (Acomplia) Monitoring – Continous blood glucose monitoring