Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
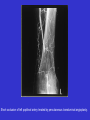
Lower limb ischaemia Peripheral vascular disease commonly affects the arteries supplying the leg and is mostly caused by atherosclerosis. Restriction of blood flow, due to arterial stenosis or occlusion, often leads patients to complain of muscle pain on walking (intermittent claudication). Any further reduction in blood flow causes ischaemic pain at rest, which affects the foot. Ulceration and gangrene may then supervene and can result in loss of the limb if not treated. The term intermittent claudication means leg pain sufficient to cause the patient to stop, which is produced by exercise and relieved by rest, and is caused by arterial occlusive disease. The pain is reproducibly caused by a given degree of exercise and relieved within minutes by rest. One who claudicates is called a claudicant, although the term claudicator is also frequently used. * 5% of males older than 50 years have intermittent claudication * 5% of claudicants progress to critical ischaemia each year * 75% of patients remain stable or show clinical improvement * Peripheral vascular disease is an independent risk factor for cardiovascular disease * At 5 years of follow-up o 10% claudicants and 50% of those with critical ischaemia have had an amputation. o 20% claudicants and 50%of those with critical ischaemia have died usually from ischaemic heart disease This presentation is based on TASC recommendations. TASC - TransAtlantic Inter-Society Consensus about management of peripheral arterial disease (pad). Claudication: * Calf or thigh pain precipitated by exercise * Usually occurs after predictable distance * Described as 'cramp' or 'tightness' * Relieved by rest * Progression of symptoms is important - worsening or improvement * Impact on social function should be identified * Need to differentiate form spinal stenosis - Also cause exercise induced leg pain - Usually associated with neurological symptoms and relieved by spinal flexion - Peripheral pulses can be present in patients with intermittent claudication Peripheral arterial disease is not simply a hemodynamic disorder. Additional factors are involved in the pathogenesis of this disease. Key factors include deconditioning, because these patients are very inactive. In addition, several studies have shown skeletal muscle injury in patients with chronic arterial occlusive disease. This injury has been characterized as a distal axonal denervation leading to loss of muscle fibers and mild atrophy of the affected muscle. Fontaine classification of chronic leg ischaemia Stage I Asymptomatic Stage II Intermittent claudication A - walking distance >200m B - walking distance <200m Stage III Ischaemic rest pain Stage IV Ulceration or gangrene, or both Angiogram showing bilateral occlusions of superficial femoral arteries in thighs. Collaterals arising from the profunda femoris artery can functionally bypass this occlusion Although many patients with claudication remain stable, about 150-200 per million of the population progress to critical limb ischaemia (Fontaine III or IV) each year. Many patients with critical limb ischaemia can undergo revascularisation, which has a reasonable chance of saving the limb. History and examination Diagnosis of peripheral arterial disease is based mainly on the history, with examination and ankle brachial pressure index being used to confirm and localise the disease Peripheral arterial disease is a marker for systemic atherosclerosis; the risk to the limb in claudication is low, but the risk to life is high. Patients with intermittent claudication experience cramping pain and weakness in the calf and/or buttocks on walking. The pain usually disappears when standing still and occurs at a fixed distance walked before it recurs. It comes on more rapidly when walking uphill than on the flat. Disease of the superficial femoral artery in the thigh results in absent popliteal and foot pulses and often causes calf claudication. Disease of the aorta or iliac artery results in a weak or absent femoral pulse, often associated with a femoral bruit. Disease at this level may cause calf, thigh, or buttock claudication. The history of claudication due to chronic peripheral arterial occlusive disease is characteristic and reproducible enough that diagnosis usually can be made on the basis of interrogation alone in the large majority of patients. The Edinburgh claudication questionnaire is highly specific (91%) and sensitive (99%) for the condition. The differential diagnosis includes both venous and neurogenic claudication (nerve root compression from a herniated disc or osteophytic encroachment, or spinal cord stenosis). Differential diagnosis of intermittent claudication Characteristic Intermittent claudication Venous claudication Nerve root pain Quality of pain Cramping "Bursting" Electric shock-like Onset immediate, Gradual, consistent Gradual, can be immediate Can be inconsistent Relieved by Location Standing still Muscle groups (buttock, thigh, calf) Legs affected Usually one Elevation of leg Whole leg Usually one Sitting down, bending forward Poorly localised, can affect whole leg Often both In general it is important to document: — The location of the pain or discomfort. — The duration of the symptom. — Whether it is worsening or improving with time and whether conservative therapy has had an effect. — The distance the patient can now walk before (a) experiencing the discomfort and (b) being forced to stop. — The elapsed time after exercise is stopped before the pain is relieved. — The type of rest or position of patient (standing at rest, sitting, lying) necessary to relieve the pain. — Whether the pain returns after the same time and distance if exercise is then resumed. There is therapeutic importance to uncovering underlying conditions that may aggravate though not cause claudication, for example, anemia, polycythemia, cardiac failure or arrhythmia, and chronic pulmonary disease with hypoxemia. Also, it should be remembered that atherosclerosis is often present at several arterial sites in the same patient, and PAD is often accompanied by coronary artery disease or carotid artery disease. Physical examination In evaluating claudication, a complete examination of the patient is necessary to detect potentially important contributing factors that may significantly impact management. The physical examination should not be limited to a vascular examination focused primarily on the extremity circulation, as described in the following passages. At the very least, it should assess the circulatory system as a whole. Discovery of systemic hypertension, cardiac murmurs or arrhythmias, carotid bruits, signs of respiratory impairment, anemia, or an abdominal aortic aneurysm are the rewards of such an examination. The skin of the legs, especially the feet and nails, should be examined for changes in color and temperature and other abnormalities such as swelling, scars of previous ulceration, and the presence of any of the so called “trophic” changes associated with severe chronic ischemia: thin, dry skin, loss of hair or subcutaneous fat, and thickened nails. Close to one third of patients with PAD have clinically significant coronary atherosclerosis, and in those who are claudicants it is often masked by exercise restrictions. Occult MI is not uncommon, and a resting ECG should be routinely obtained on all new patients with IC if no recent report is available. Approximately one fourth of PAD patients have hypertension, and in these consideration should be given to the possibility of renal artery narrowing. Finally, approximately 10% to 15% have cerebrovascular disease, mostly in the form of carotid stenosis. Walking Distance Because the major clinical manifestation of IC is walking impairment, walking distance is the primary objective parameter for the assessment of treatment. The usual treadmill exercise test to assess the hemodynamic significance of arterial occlusive disease in the lower extremities is performed in a vascular diagnostic laboratory. The patient walks at a standard speed and grade on a treadmill until claudication pain is experienced or a time limit has been reached, for example, 5 minutes at 3.5 km/h on a 12% incline. The latter is equivalent to walking nearly 600 meters at average speed. Pulse palpation Pulse palpation should be correlated with claudication distance and location of pain, usually indicates the location and severity of the responsible arterial lesion(s). Auscultation of bruits may give additional useful information. Method of palpating dorsalis pedis pulse. Examine pulse from the foot of the bed, keeping the fingers flat for the dorsalis pedis , while applying counterpressure with the thumb. The dorsalis pedis artery lies superficially on the dorsum of the foot, although its position varies considerably. Method of palpating posterior tibial pulse. Examine pulse from the foot of the bed, using the fingertips for the posterior tibial, while applying counterpressure with the thumb. The posterior tibial artery lies deeper behind the medial malleolus. Many healthy people have only one foot pulse. Method of palpating popliteal artery with patient's knee slightly flexed. Use thumbs to apply counterpressure while palpating the artery, which lies deep in popliteal fossa, with fingers. The popliteal pulse can be difficult to palpate in muscular patients. A prominent popliteal pulse suggests the possibility of a popliteal aneurysm. Method of palpating femoral pulse in skin crease of groin. Counterpressure on the lower abdomen pushes the skin crease towards the inguinal ligament and reduces the risk of missing the puls For example, a decreased amplitude of the femoral pulse, along with a loud bruit proximally over the iliac artery, usually indicates the presence of a significant iliac stenosis. With complete occlusion, no pulsation or bruits are present. Monitoring pulses and bruits after a brief period of exercise occasionally will provide additional information if pulses disappear or bruits accentuate. Simply combining the pulse findings with the location and severity of the ischemic symptoms allows the presence and segmental location of the responsible arterial lesions to be predicted with accuracy comparable to that of noninvasive testing (close to 90%). Hand-held doppler * Reflection of an ultrasound wave off a stationary object does not change its frequency * Reflection off a moving object results in a change of frequency * The change in frequency is proportional to velocity or blood flow * Hand held 8 MHz doppler probe is used to assess arterial system * Can be used to measure arterial pressures * Measurements can be made at rest and after exercise * In normal individual lower limb pressures are greater than upper limb * Ankle-brachial pressure index (ratio of best foot systolic to brachial systolic pressure) The ankle-brachial pressure index (ABPI) should be measured in both legs in all new patients with intermittent claudication, in both legs. A blood pressure cuff is placed on the upper arm and inflated until no brachial pulse is detected by the Doppler device. The cuff is then slowly deflated until a Doppler-detected pulse returns (the systolic pressure). This maneuver is repeated on the leg, with the cuff wrapped around the distal calf and the Doppler device placed over the dorsalis pedis or posterior tibial artery. The ankle systolic pressure divided by the brachial systolic pressure gives the ABI. We can also wrap the caff around other parts of the leg (e.g. tigh) and take segmental limb pressures. ABI First, it objectively confirms or rules out the existence of hemodynamically significant occlusive disease between the heart and the ankle, which in almost all cases lies distal to the renal arteries. Second, it provides a rough measure of the severity of the occlusive disease for correlation with the patient’s symptoms. Third, it can serve as an aid in differential diagnosis, in that patients with exercise-related leg pain of other causes will either have a normal ankle pressure or a degree of reduction which does not fit with the severity of disability. Finally, the ABPI can detect lesser disease in the contralateral extremity, which may not be suspected because it is masked by the more severe symptomatic leg. Special considerations in evaluating diabetic patients. Patients with long-standing diabetes commonly develop calcified, incompressible vessels, which cause false high SLP measurements, particularly at the ankle level. The presence of this artifact is obvious when the measured SLP are all unbelievably high (eg, 300 mm Hg) or ABPI is greater than 1.5, but subtler degrees can be misleading. Relationship of clinical features to ABPI * In normal individuals pressures do not fall flowing exercise * In claudicants the ABPI falls and recovery is delayed * In diabetic lower limb pressures are falsely elevated due to calcification in the vessel wall * ABPI in patients with claudication is not well correlated with their exercise performance on a treadmill . Toe pressures * Provides accurate assessment of distal circulation * Not influenced by calcification in pedal vessels * Medical calcification particularly seen in diabetics * Normal toe pressures are 90-100 mmHg * Toe pressure less than 30 mmHg suggests critical limb ischaemia Noninvasive localization of lesions If it is desirable to localize and gauge the severity of occlusive arterial lesions to assist in planning an intervention; then duplex scanning or magnetic resonance angiography (depending on local availability, experience, and cost) can be used as a preliminary, noninvasive examination before angiography. In many cases, the information supplied by simpler tests such as segmental limb pressure or pulse volume recording is adequate for decision making. It should be noted that common practice in relation to noninvasive investigations used in patients differs widely between Europe and North America. For example, segmental limb pressures (SLP), pulse volume recordings (PVR), and velocity waveform analysis (VWF) are much more widely used in North America, where there is already considerable experience in their use and interpretation. In Europe, however, a preferred alternative to these tests is duplex scanning. Segmental limb systolic pressure measurement (SLP) SLP is now widely used because it accurately detects and segmentally localizes hemodynamically significant large-vessel occlusive lesions in the major arteries between the heart and the measuring point. Segmental measurements at levels down the leg (upper and lower thigh and calf), in addition to the ankle, are obtained in the same fashion as the ankle pressure (AP). A sphygmomanometer cuff is placed at a given level with a Doppler probe over one of the pedal arteries, and the systolic pressure in the major arteries under the cuff is measured. The location of occlusive lesions is apparent from the pressure gradients between the different cuffs. Segmental plethysmography or pulse volume recordings (PVR) A plethysmograph is any instrument that detects and graphically records volume change. To perform segmental plethysmography, any instrument that measures the relative change in volume associated with each cardiac cycle in the segment of limb encircled by a plethysmographic sensor may be used. In common practice calibrated air-filled cuffs, much like sphygmomanometer cuffs, are employed. They are placed around the leg at selected locations and connected to a plethysmograph, which produces a “pulse volume recording” (PVR). Doppler Velocity Wave Form (VWF) This is used in some Vascular Diagnostic Laboratories, instead of PVR, to complement SLP. Here, arterial VWF is recorded using a continuous-wave Doppler over the femoral, popliteal, posterior tibial, and dorsalis pedis arteries. Similar to the interpretation of PVR, qualitative differences in the magnitude and contour of VWF between two adjacent recording points identifies the presence of an occlusive lesion in the intervening arterial segment. However, VWF recording and analysis is very operator dependent, and for that reason PVR are preferred by most. Duplex ultrasound * Combined pulsed doppler and real time B mode ultrasound * Allows imaging of vessels and any stenotic lesion * Flow and pressure wave form can be also be assessed Doppler wave forms from normal and diseases arteries In normal individuals a 'triphasic' wave is obtained * Rapid antegrade flow during systole * Transient reverse flow in early diastole * Slow antegrade flow in late diastole An arterial stenosis results in the following distal to the lesion: * Decreased rate of rise of the antegrade flow * A reduced amplitude of the forward velocity * Loss of reverse flow (i.e. a 'biphasic' wave form) * At the stenosis velocity is increased * Severe stenosis result in a monophasic waveform * Duplex ultrasound has sensitivity of 80% and specificity of 90% for stenotic lesions in the femoral and popliteal segments Magnetic resonance angiography * Time of flight sequences * No contrast required. CT angiography * Required intravenous contrast and ionising radiation * Spiral CT and reconstruction can provide detailed images * Particularly useful for the assessment of aneurysmal disease Angiography Angiography in a patient with intermittent claudication is usually indicated only when a decision has been made to intervene, should a suitable lesion be identified. * Usually performed using digital subtraction techniques * Catheter inserted using Seldinger technique * Femoral artery is commonest site of venous access * Generally safe procedure performed under local anaesthetic •Potential complications include * Contrast-related o Anaphylactic reaction o Toxic reactions o Deterioration in renal function * Technique-related o Haematoma o Arterial spasm o Sub-intimal dissection o False aneurysm o Arteriovenous fistula o Embolisation o Infection Blood tests The following blood tests should be performed in all new patients presenting with intermittent claudication: — complete blood count (hemoglobin, hematocrit, white cell count); — platelet count; — fasting blood glucose or hemoglobin A1c; — creatinine; — fasting lipid profile; — urinalysis (for glycosuria/proteinuria). The following laboratory investigations should be performed selectively in atypical patients (eg, those with early age of onset, atypical distribution of occlusive lesions, personal or family history of thrombotic events, lack of any of the common risk factors for, or a family history of, atherosclerosis, unexpected failed interventions): — hypercoagulability screen; — homocysteine levels. Homocysteine Recently, several reports have shown a strong association between increases in plasma homocysteine concentration and PAD. This may be an important risk factor in patients younger than 50 years who present with claudication. ECG A baseline resting electrocardiogram is recommended in new patients with intermittent claudication, but in the absence of family history, risk factors, or suggestive symptoms or signs, there is as yet no good evidence for routine further investigation of other circulations in such patients. Patients with peripheral arterial disease have a high associated prevalence of coronary, cerebrovascular, and renal artery disease. Patients with symptoms or signs suggesting atherosclerotic disease in other regions will need further investigations and special assessment. Algorithm for investigation of suspected intermittent claudication Investigation There are many causes of leg pain that can occur in the presence of asymptomatic peripheral vascular disease. Therefore, the absence of pulses does not necessarily imply a causal link. Furthermore, the presence of pulses at rest does not exclude symptomatic peripheral vascular disease. A good history together with an ankle brachial systolic pressure index of less than 0.9 confirms the diagnosis. Duplex ultrasound scanning is useful for delineating the anatomical site of disease in the lower limb. Many hospitals still use arteriography for this purpose or when the results of duplex scanning are equivocal. This invasive and expensive investigation should not be requested unless there is a plan to proceed with revascularisation, if possible. Algorithm for treatment of intermittent claudication Principles of treatment Intermittent claudication seems a relatively benign condition, although severe claudication may preclude patients from manual work. The risk of generalised vascular disease is probably more important. Patients with claudication have a three times higher risk of death compared with age matched controls. The overriding issue in the management of patients presenting with IC is that they are at significant risk of developing severe and often fatal cardiovascular complications; thus, their most serious problem is not the limitation of walking, even though that may be their only symptom. The first priority in designing a treatment plan for these patients is to try to modify the known risk factors for the progression of atherosclerosis and development of atherothrombotic complications. It is important to explain to the patient the rationale for this strategy and that it is not designed to improve the claudication distance. Modification of risk factors is therefore vital to reduce death from myocardial infarction and stroke. All patients should be advised to stop smoking and take regular exercise. They should also be screened for hyperlipidaemia and diabetes. Obesity reduces exercise capacity, and losing weight will improve the walking distance. Only when best medical treatment has been instituted and given sufficient time to take effect should endovascular or surgical intervention be considered, as most patients' symptoms improve with best medical treatment to a point where invasive intervention is no longer needed. Best medical treatment is beneficial even in patients who eventually need invasive treatment, as the safety, immediate success, and durability of intervention is greatly improved in patients who adhere to best medical treatment. Factors which may influence the decision to treat claudication For Severe symptoms Job affected No better after exercise training Stenosis or short occlusion Proximal disease Unilateral disease Against Short history Continued smoking Severe angina or chronic obstructive airways disease Long occlusion Distal disease Multilevel disease Exercise programmes A program of exercise therapy (preferably supervised) should always be considered as part of the initial treatment for patients with intermittent claudication. A recent meta-analysis of 21 supervised exercise programmes showed that training for at least six months, by walking to near maximum pain tolerance, significantly improved pain free and maximum walking distances. Treadmills can be used for objective measurement of walking distance and for exercise training Smoking cessation in peripheral arterial disease All patients with peripheral arterial disease should be strongly and repeatedly advised to stop smoking. Cessation rates are likely to be enhanced by a special program. Unfortunately, rates of cessation after simple oral or written advice from a doctor are as low as 13% at two years. Randomised controlled trials have shown that nicotine replacement treatment approximately doubles the cessation rate in unselected smokers. Control of diabetes in peripheral arterial disease Patients with diabetes and peripheral arterial disease should have aggressive control and normalization of blood sugar. Fasting blood sugars should range from 80 to 120 mg/dL, and postprandial sugars should be <180 mg/dL; hemoglobin A1c should be <7.0%. Diabetic foot care in peripheral arterial disease All diabetic patients with peripheral arterial disease should receive special advice and regular supervision to minimize the risks of developing diabetic foot complications. Lipid control in peripheral arterial disease Because of the high incidence of coexistent coronary disease and similar mortality risk to coronary patients, patients with peripheral arterial disease with a low-density lipoprotein (LDL) cholesterol level greater than 125 mg/dL should be placed on therapy. In the first instance, a diet should be tried. If this fails to achieve a goal of LDL cholesterol level less than 100 mg/dL, then medications should be tried. Control of hypertension in peripheral arterial disease Peripheral arterial disease patients with hypertension should have this risk factor controlled. Reducing blood pressure to <140/85 mm Hg ACE (angiotensin converting enzyme) inhibitors should be considered in all patients, even if normotensive. However, clinicians should be aware that when drug therapy results in a large decrease in systemic blood pressure, some patients may experience a slight worsening of their claudication symptoms. Hypercoagulable states in intermittent claudication Patients with intermittent claudication who have a hypercoagulable state and proven arterial or venous thrombosis should be anticoagulated with acenocumarol (Europe),coumarins (USA). Antiplatelet therapy in peripheral arterial disease All patients with peripheral arterial disease (whether symptomatic or asymptomatic) should be considered for treatment with low-dose aspirin, or other approved antiplatelet (unless contraindicated), to reduce the risk of cardiovascular morbidity and mortality. Patients with intermittent claudication mostly receive drug treatment for coexisting disease (eg, hypertension), risk factor modification (eg, hyperlipidemia), and as prophylaxis against thrombotic events associated with atherosclerosis (eg, antiplatelet drugs). No pharmacological agent has proved efficacious enough in providing significant reduction or elimination of symptoms of claudication to gain widespread acceptance and use for improving walking. However, a number of types of drugs have been promoted for this indication, Pharmacotherapy for symptoms of intermittent claudication Although some controlled clinical trials with pentoxifylline, naftidrofuryl, buflomedil, and recently cilostozol, have shown statistically significant improvement in walking distance, the average benefit was small. Greater benefit, observed in a minority of patients, may warrant a short course of therapy with continued use of such agents if sufficient benefit is observed. Recent clinical trials have shown a greater benefit of cilostazol for both walking distance and quality of life, which may warrant more widespread use. However, currently there are insufficient data to recommend the routine use of pharmacotherapy in all patients with claudication. Cytokines - future treatment? Vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF) are mitogenic agents for the development of new collateral channels in models of peripheral ischemia. VEGF has been shown to augment collateral vessel development and increase capillary density in skeletal muscle in a rabbit model. This effect has been observed when the VEGF protein is administered by intraarterial infusion and when the DNA encoding for VEGF is given by intramuscular injection. Early phase I and phase II trials are now in progress to determine whether this novel therapy has a clinical application in patients with claudication and severe leg ischemia. Invasive therapy Before offering a patient with intermittent claudication the option of any invasive therapy, endovascular or surgical, the following considerations must be taken into account: — a predicted or observed lack of adequate response to exercise therapy and risk factor modification; — the patient must have a severe disability, either being unable to perform normal work or having very serious impairment of other activities important to the patient; — absence of other disease that would limit exercise even if the claudication was improved (eg, angina or chronic respiratory disease); — the individual’s anticipated natural history and prognosis; — the morphology of the lesion must be such that the appropriate intervention would have low risk and high probability of initial and long-term success. The decision to consider a patient for interventional therapy is arrived at by the patient balancing existing disability against the procedural risk and likelihood of longterm success of an intervention. Choosing between techniques with comparable short- and long-term benefit When two techniques of revascularization (endovascular and open surgery) give equivalent short-term and long-term benefit, the technique with the least morbidity and mortality must be used first. Cost also should be considered. Endovascular techniques The number of percutaneous transluminal angioplasties performed for claudication has risen steeply in recent years. In some situations endovascular techniques have virtually replaced conventional surgery. Percutaneous transluminal angioplasty seems best suited for stenoses or short occlusions of the iliac and superficial femoral vessels. Angioplasty carries a small but definite risk of losing the limb because of thrombosis or embolisation, and patients should be informed of this risk. Percutaneous transluminal angioplasty: * Angioplasty of the aorto-iliac segment has a 90% 5 year patency * Angioplasty of the infra-inguinal vessels has a 70% 5 year patency * Best results seen with short segment stenoses less than 2 cm long •Complications occur in less than 2% of patients o Wound haematoma o Acute thrombosis o Distal embolisation o Arterial wall rupture Short occlusion of left popliteal artery treated by percutaneous transluminal angioplasty. The balloon catheter is passed through the occlusion over a guide wire and inflated. Appearance after angioplasty PTA with implantion stent Metallic stents push back the atheroma and improve on the initial lumen gain after angioplasty alone. The indications for iliac stents include a residual stenosis or dissection after angioplasty and long occlusions, but there seems little evidence to justify their routine use. Deployment of stents more distally has produced disappointing results due to high restenosis rates. Occlusion of the right common iliac artery before (left) and after (right) insertion of stent Morphological stratification of iliac lesions Abbreviations: CIA, common iliac artery; EIA, external iliac artery; CFA, common femoral artery. Treatment of choice for TASC type A and D aortoiliac lesions: Endovascular procedure is the treatment of choice for type A lesions, and surgery is the procedure of choice for type D lesions. Role of stenting for residual pressure gradient, dissection, or elastic recoil: Stenting improves the technical and initial clinical success in cases of residual pressure gradient or dissection after angioplasty, or in cases of elastic recoil. Between these two groups are types B and C lesions, in which no firm recommendations can be made about the preferred interventional option. At present, endovascular treatment is more commonly used in type B lesions, and surgical treatment is more commonly used in type C lesions. It should be emphasized that there is no sufficient solid evidence to make any firm recommendations, particularly in the case of types B and C. The indications for iliac artery stenting, which are generally accepted in clinical practice, are as follows: — insufficient hemodynamic result of PTA due to elastic recoil based on residual pressure gradient; — massive, lumen-obstructing dissection; — treatment of chronic occlusions; — iliac artery ulceration associated with symptoms; — restenoses after previously performed PTA; — complex lesions for which primary stenting may give more satisfactory results. Morphological stratification of femoropopliteal lesions Treatment of choice for TASC type A and D femoropopliteal lesions: Endovascular procedure is the treatment of choice for type A lesions, and surgery is the procedure of choice for type D lesions. Femoropopliteal stenting in PAD: Femoropopliteal stenting as a primary approach to the interventional treatment of intermittent claudication or CLI is not indicated. However, stents may have a limited role in salvage of acute PTA failures or complications. Morphological stratification of popliteal and tibial lesions Unlike the aortoiliac and femoropopliteal segments, the infrapopliteal vessels are usually not treated unless there is critical acute or chronic limb ischemia. Therefore, most of the experience in infrapopliteal endovascular recanalization has come from patients with limb-threatening ischemia. Surgery Surgery is rarely necessary in patients with IC; in fact, surgery should be avoided initially and other options pursued in most patients. Ordinarily, if exercise therapy fails or is rejected by the patient for other reasons, these patients may try pharmacotherapy or be referred for imaging to evaluate the possibility of balloon angioplasty. If these options are not possible, or fail, surgery may be considered. The decision involves an individualized risk to benefit analysis, balancing the benefit of relieving that particular patient’s disability against the immediate risks (morbidity/mortality/technical failure) and the risk of late failure of the proposed surgical procedure. This weighing of risk and benefit must be settled in the patient’s favor. Endarterectomy is an acceptable option when truly localized disease is present, for example, the narrowing of the aorta and common iliac arteries alone. Otherwise, patency rates are unsatisfactory, and bypass grafting is more appropriate. The traditional operation for aortoiliac occlusive disease is an aortofemoral bypass, performed with a prosthetic graft because of the large caliber of the vessels. Axillobifemoral bypass is an extra-anatomic bypass that reduces the risk of proximal reconstruction by avoiding an abdominal incision with aortic dissection and clamping. However, its primary patency is inferior to aortobifemoral bypass and, in spite of improving results, it is still not recommended for the treatment of IC. Infrainguinal bypass procedures are best performed with autogenous vein grafts, although the results of prosthetic bypasses are acceptable if the graft does not cross the knee joint. Considering the quite dismal results of percutaneous angioplasty and stenting for disease in the crural arteries, autogenous vein bypass to the distal vessels should be considered as first-line therapy in patients with limb-threatening ischemia and distal disease. Polyester (Dacron) aortobifemoral bypass grafts have five year patency rates of over 90% but are associated with a mortality of up to 5%. Complications include graft infection and postoperative impotence. Femoropopliteal bypass grafting, using autologous long saphenous vein, polyester, or polytetrafluoroethylene (Goretex) yields patency rates of less than 70% at five years. The early patency of prosthetic grafts seems similar to that of vein grafts, although the long term results seem less good. Femoropopliteal bypass grafts should rarely be used for patients with claudication. Surgery for intermittent claudication: — Surgery should be offered to treat severe symptoms only after other forms of medical therapy have been recommended and have either failed or been rejected for good reason. — If used, surgery for IC should employ the procedure offering extended clinical benefit with a high benfit-to-risk ratio. — If necessary, surgery is the treatment of choice of type D lesions but may be used also in type B and C lesions. Types of bypass graft include: * Biological grafts o Autografts + Long saphenous vein - in-situ or reversed + Internal mammary artery o Allografts + Dacron coated umbilical vein * Synthetic grafts o Dacron - woven or knitted +/albumin coated o Woven grafts - smaller pores. No preclotting required o Velour - Polyfluorotetraethylene (PTFE) Choice of graft material * Determined by long term patency rates * Autologous vein is best graft material but not always available * Interposition of vein between PTFE graft and artery at distal anastomosis can improve long term patency Comparative three year patency of vein and synthetic grafts: Above knee anastomosis Below knee anastomosis Vein PTFE 85-90% 75-80% 70-75% <50% Benefits of vein versus prosthetic grafts for above-knee femoropopliteal bypass. In favor of vein — Better long-term patency rates — Avoidance of "staged" approach to femoral popliteal — Need for other use overestimated. — Lower risk of graft infection In favor of prosthesis — Close to equivalent long-term patency rates — Fewer wound complications — Vein available for secondary or coronary bypass — Shorter operative time Reasons for graft failure * Less than 30 days - technical failure * 30 days to 1 years - neointimal hyperplasia at distal anastomosis * More than 1 years - progression of distal disease Success of treatment for intermittent claudication — Objective outcome: relevant improvement in walking distance as measured by a standardized exercise test; — Symptomatic outcome: improvement on a validated disease-specific health status questionnaire; — General quality of life: improvement on a validated generic health status questionnaire; — Postrevascularization: objective proof of patency of any revascularized segment (ideally with imaging). Use of prophylactic antibiotics with prosthetic grafts Patients undergoing prosthetic grafts should have prophylactic antibiotic therapy perioperatively Antiplatelets as adjuvant pharmacotherapy after revascularization Antiplatelet therapy should be started preoperatively and continued as adjuvant pharmacotherapy after an endovascular or surgical procedure. Unless subsequently contraindicated, this should be continued indefinitely. Caution should be used in patients in whom use of anticoagulants is proposed. Surveillance program for bypass grafts and transluminal angioplasty Patients undergoing bypass graft placement in the lower extremity for the treatment of claudication or limb-threatening ischemia should be entered into a surveillance program. This program should consist of: — interval history (new symptoms); — vascular examination of the leg with palpation of proximal, graft, and outflow vessel pulses; — periodic measurement of resting and, if possible, post-exercise ankle-brachial indices; — duplex scanning of the entire length of the graft, with calculation of peak systolic velocities and the velocity ratios across all identified lesions; Surveillance programs should be performed in the immediate postoperative period and at regular intervals for at least 2 year Critical limb ischaemia European Working Group on Critical Leg Ischaemia (1991): ' Persistently recurring ischaemic rest pain requiring regular adequate analgesia for more than 2 weeks, or ulceration or gangrene of the foot or toes, with an ankle pressure of <50 mmHg or toe pressures of <30 mmHg or reduced TCPO2 (<30 mmHg) ' The term critical limb ischemia should be used for patients with chronic ischemic rest pain, ulcers, or gangrene attributable to objectively proven arterial occlusive disease. Most of these patients would be expected to require a major amputation within the next 6 months to a year in the absence of a significant hemodynamic improvement. The term critical limb ischemia implies chronicity and is to be distinguished from acute limb ischemia. Ischemic rest pain is characterized by severe, often intolerable discomfort in the toes, forefoot, or heel that is not relieved with the use of simple analgesics and only responds to strong analgesics or opiates. The pain is caused by ischemia, areas of tissue loss, ischemic neuropathy, or a combination of these; it occurs or worsens with reduction of perfusion pressure. In most cases, walking capacity is very severely impaired, often becoming almost impossible. Ischemic rest pain most typically occurs at night but can occur even during the day when the patient is resting in supine position. The pain is often severe, enough to wake the patient at night and force him or her to rub the foot, get up, or take a short walk around the room. Partial relief may be obtained by the dependent position and application of heat, whereas elevation and cold increase the severity of the pain. Often, patients sleep with their ischemic leg hanging over the edge of the bed, or sitting in an armchair all night; as a consequence, ankle and foot edema develop, which further increases ischemia and pain. Contracture of the knee and ankle joints may occur. Gangrene can ensue when the reduced arterial supply to the limb does not meet with the metabolic demands of the ischemic leg. Late stages of CLI are characterized by sensory loss and muscle weakness. Infection may precede or may complicate the nonhealing ulcer. Most patients with CLI have multilevel, multivessel disease, often with three-vessel tibioperoneal occlusive disease. Limb loss and cardiovascular mortality and morbidity ensue rapidly if CLI is not treated. Treatment options include surgical revascularization, amputation, and endovascular intervention. The main treatment goals for CLI are limb preservation, quality-of-life improvement, and a reduction in cardiovascular complications from the underlying diffuse atherosclerosis. Patients with CLI usually not only have multilevel disease in the involved extremity but also have a higher likelihood of significant atherosclerosis in other circulations, are a higher operative risk, and have a more limited life expectancy compared with patients with intermittent claudication. Despite aggressive correction of distal ischemia, these patients have a limited life expectancy, with less than 60% surviving more than 3 years after treatment. Prompt referral of patients with critical limb ischemia to a vascular specialist will improve the chances of successful treatment. Multidisciplinary approach is necessary in critical limb ischemia: Close cooperation between disciplines is particularly desirable for the timely diagnosis and treatment of both diabetic and nondiabetic patients with critical limb ischemia. Diabetes mellitus accentuates the risk of CLI by four times, while continued tobacco abuse triples the risk. Diabetes mellitus leads to rapid progression of atherosclerosis at a premature age and preferentially affects distal calf vessels. This diffuse distal disease that is associated with diabetes poses challenges for the surgeon or endovascular specialist. It has been estimated that 40% to 45% of all amputees are diabetic. A diabetic patient with CLI is 10 times more likely to need amputation compared to a nondiabetic. Gangrene associated with critical limb ischaemia Foot ulcer associated with critical limb ischaemia History and examination Patients with critical limb ischaemia often describe a history of deteriorating claudication, progressing to nocturnal rest pain. Ulceration or gangrene commonly results from minor trauma. Nocturnal rest pain often occurs just after the patient has fallen asleep when the systemic blood pressure falls, further reducing perfusion to the foot. Severe ischemia is often associated with atrophy of the calf muscles, loss of hair growth over the dorsum of the toes and foot is another relatively common sign of severe arterial insufficiency; it often is accompanied by thickening of the toenails secondary to slowness of nail growth. In more advanced cases, there is atrophy of the skin. In severe, long-standing cases, the color of the skin is usually extremely pale or cyanotic; there may be rubor on dependency because of chronic dilatation of the precapillary and postcapillary vessels. Arterial ulcers usually involve the tips of the toes, the heel of the foot, or wherever local pressure has caused further decrease of perfusion. Arterial ulcers typically have irregular borders; the base of the ulcer is pale unless inflammation or infection, as occurs in many cases, gives rise to local reactions such as the production of exudate and pus. These may lead to crust formation, covering the ulcer surface, which in many cases leads to a decrease in pain. Gangrene usually affects the digits; in severe cases, it may involve the distal parts of the forefoot. Any minor local trauma such as cutting the toenails may elicit formation of an ulcer and lead to gangrene; local pressure (shoes, use of local heat) also can cause ulcer and gangrene formation on any other place of the foot or leg. Gangrenous tissue, if not infected, has a tendency to shrink and eventually lead to mummification of the part affected. Hanging the foot out of bed increases perfusion and produces the typical dusky red hue due to loss of capillary tone. Elevation causes pallor and venous guttering. Inspect the foot carefully for ulceration under the heel and between the toes. Swelling suggests deep infection. If you can palpate foot pulses consider an alternative cause of pain. Patients with critical limb ischaemia require urgent referral to a vascular surgeon. Critically ischaemic foot displaying typical dusky red hue on dependency (ischaemic rubor) Critical limb ischaemia * Characterised by rest pain * Occurs when foot is elevated (e.g. in bed) * Improved with foot dependent * May be associated with ulceration or gangrene * Foot pulses are invariably absent Investigation The ankle brachial systolic pressure index is usually less than 0.5. Arterial calcification may result in falsely increased pressures, and caution is needed when relying on Doppler pressures alone, especially in diabetic patients. All patients with critical limb ischaemia should ideally have arteriography with a view to endovascular treatment, if feasible. Duplex scanning may be used instead of angiography and for mapping of the long saphenous vein before distal bypass surgery. Dependent Doppler or pulse generated run-off can help to determine the most suitable artery to receive a distal bypass graft if these cannot be identified by angiography. The diagnostic evaluation of patients with critical limb ischemia should be directed toward the following objectives: — objective confirmation of the diagnosis; — localization of the responsible lesion(s) and a gauge of relative severity; — assessment of the hemodynamic requirements for successful intervention ( proximal, distal or combined revascularization of multilevel disease); — assessment of individual patient operative risk; — assessment of atherosclerotic risk factors; — assessment of atherosclerosis in other systems. To achieve the objectives listed previously, the following investigations should be used in patients with critical limb ischemia: — complete clinical history and examination, including the coronary and cerebral circulation; — basic hematologic and biochemical tests; — resting ECG; — ankle or toe pressure measurement or other objective measures for the severity of ischemia; — imaging of the lower limb arteries in patients considered for intervention; — duplex scan of the carotid arteries should be done in selected patients at high risk; — a more detailed coronary assessment in selected patients. Principles of treatment The same principles and techniques used to treat claudication also apply to critical limb ischaemia. However, critical limb ischaemia is usually caused by multilevel disease, which means that success rates are lower. Treatment focuses on saving the limb, although modification of risk factors remains important. The principal urgent components of basic treatment of CLI are the control of pain and any infection in the ischemic leg, prevention of progression of thrombosis if this is thought to be a precipitating factor in the ischemia, and the optimization of cardiac and respiratory function. While instituting basic treatment, the full precise morphology of the PAD should be simultaneously established by some form of imaging technique. This will determine further management of the arterial lesion. If not promptly diagnosed and intervened upon, CLI can lead to limb loss, gangrene, sepsis, myocardial infarction, and death. Studies have shown that within the first several months of the diagnosis of CLI, death occurs in 9%, myocardial infarction in 1%, stroke in 1%, amputation in 12%, and persistent CLI in 18% of patients. One- and 2-year mortality rates are noted to be 21% and 31.6%, respectively. Algorithm for treatment of critical limb ischaemia Control of Risk Factors Patients with CLI have the same cardiovascular risk factor profile as patients with claudication. However, patients with CLI have a more diffuse and extensive degree of atherosclerosis. Therefore, their risk of cardiovascular events and mortality is higher than that of patients with claudication. Despite the end-stage nature of this disease, aggressive systemic risk factor modification is still warranted. Ideally, the patient should be treated with the least risky and least morbid but most successful and durable procedure. Comorbid risk factors will modify this ideal to give priority to patient safety. High-risk, frail patients may be best treated with less invasive interventions, even though durability may not be optimal. In some patients, revascularization procedures should be abandoned for primary amputation when patient factors suggest extremely high morbidity and mortality or the arterial anatomy predicts a poor outcome of intervention. Pain control in critical limb ischemia Adequate treatment of ischemic pain is mandatory in all patients with critical limb ischemia and may require short-term use of narcotics. Pain control should be individualized and multifactorial. However, pain control treatment should not delay definitive treatment of the arterial lesion. Opiates can be supplemented by nonsteroidal anti-inflammatory drugs if these are not contraindicated. Apart from rehydration, adequate analgesia alone may be the best treatment for patients with dementia or other severe comorbidity. If opiate analgesia remains inadequate, then lumbar sympathectomy (surgical or chemical) or spinal cord stimulation may help. Topical therapy for ischemic ulceration Topical therapy for ischemic ulceration should be guided by the principles of wound care. The extremities should be kept clean, with appropriate debridement. Systemic antibiotic therapy in patients with critical limb ischemia Systemic antibiotics are required in patients who develop cellulitis or spreading infection in ischemic ulcers or gangrene but should not delay more definitive treatment. Use of prostanoids in critical limb ischemia Patients who have a viable limb in whom revascularization procedures are impossible, carry a poor chance of success or have previously failed, and particularly when the alternative is amputation, may be treated with prostanoids. Vasoactive drugs in treatment of critical limb ischemia Very few vasoactive drugs have been properly investigated in patients with critical limb ischemia. Because the results are unconvincing or negative, current drugs cannot be recommended in patients with chronic critical limb ischemia. Endovascular treatment Percutaneous transluminal angioplasty or stenting of proximal disease may relieve ischaemic rest pain, but healing of ulceration or gangrene usually requires restoration of foot pulses. This may necessitate extensive angioplasty of the superficial femoral, popliteal, and tibial arteries. Endovascular treatment can also reduce the magnitude of subsequent surgery. Invasive treatment The primary aim is revascularization to provide sufficient blood flow to relieve the rest pain and heal skin lesions. Most patients with CLI have multisegment arterial disease, and often the elimination of the most proximal obstruction might be sufficient to achieve these aims. The decision about what type of revascularization to recommend ideally should be made by a multidisciplinary team. Important issues that may influence the recommended decision are: — lesion morphology; — risk of surgery for that particular patient; — previous procedures (ie, bypass or angioplasty); — patient’s life expectancy; — local expertise and experience with particular surgical or endovascular procedures. In general, endovascular procedures are safer and require shorter hospitalization compared with surgical procedures. Surgery Patients with a pattern of arterial disease considered unsuitable for endovascular treatment will usually require surgery. Fit patients with proximal disease benefit greatly from aortobifemoral bypass grafting. In unfit patients the options include crossfemoral bypass for unilateral disease or axillobifemoral bypass for bilateral disease. These extra-anatomic procedures have lower patency rates. Surgical treatment options for aortoiliac disease Many patients with distal disease will require bypass grafting to the popliteal or crural arteries below the knee. Autologous vein grafts give the best patency rates (70% at one year). Postoperative duplex surveillance may improve patency by permitting the detection and treatment of vein graft stenoses before occlusion occurs. Treatment of chronic critical leg ischemia due to bypass graft occlusion In patients with chronic critical leg ischemia, surgical revision or graft replacement is the preferred treatment for bypass graft occlusion. Thrombolysis may be considered as a treatment option in patients who present early after their bypass graft occlusion where the limb is not immediately threatened. Lumbar sympathectomy in critical limb ischemia There is currently insufficient scientific evidence for the selection of patients likely to benefit from lumbar sympathectomy for the treatment of critical limb ischemia. Primary amputation Primary amputation is defined as amputation of the ischemic lower extremity without an antecedent attempt at revascularization. Amputation is considered as primary therapy for lower limb ischemia only in selected cases. Primary major amputation for critical limb ischemia is indicated in advanced distal ischemia with: — unreconstructable arterial occlusive disease; — necrosis of significant areas of weight-bearing portion of the foot; — fixed, unremediable flexion contracture of the leg; — a terminal illness or very limited life expectancy because of comorbid conditions. Secondary amputation Unreconstructable vascular disease has become the most common indication for secondary amputation, accounting for nearly 60% of patients. Persistent infection despite aggressive vascular reconstruction is the second most common diagnosis. The goals of secondary amputation are the relief of ischemic pain, the complete removal of all diseased, infected and necrotic tissue, the achievement of complete healing and the construction of a stump suitable for ambulation with a prosthesis. It is the goal of amputation to obtain primary healing of the lower extremity at the most distal level possible. Preservation of the knee joint has enormous advantages for wearing artificial limbs and subsequent mobility. However, there is little point in risking a non-healing, below knee amputation if the patient seems unlikely to walk again. Similarly, a patient with good prospects of wearing an artificial limb will fare better with an above knee amputation, if below knee amputation seems unachievable. Local amputation of ulcerated or gangrenous toes will not heal without revascularisation. Success of treatment for critical limb ischemia should take into account an improvement in the following: Objective outcome: Complete healing of skin lesions. Standardized reporting criteria should include technical success, hemodynamic testing, procedural morbidity, limb function, and amputation and mortality rates. Technical success Treatment of critical limb ischemia may require more than one treatment modality, for example, thrombolytic therapy and bypass grafting. Technical success does not require the restoration of palpable pedal pulses in all cases. Many procedures, such as profundaplasty, may provide increased distal perfusion through collateral beds. Successful revascularization should lead to an increase in ankle-brachial index Limb salvage Limb salvage after treatment for chronic critical limb ischemia (CLI) is defined as preservation of a functional foot. Because patients with advanced CLI may present with ischemic gangrene of the toes, forefoot, or heel, removal of this necrotic tissue is an essential part of any therapeutic regimen. Healing of wounds Complete healing refers to a continuous viable, epithelial covering over all previously open wounds. Long incisions are often required for surgical intervention. Mortality rate Procedural mortality is defined as death within 30 days of the intervention or within the same hospitalization as the intervention, if this is longer than 30 days. Traditionally, the standard has been to report as procedural mortality only those patients who die within 30 days of therapy. Patients with CLI, however, often have severe comorbid conditions that may be worsened by the procedure.