Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
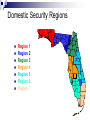
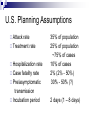
Disaster Response And Respiratory Care Objectives Understand the universal characteristics of disasters and the components of an all hazards approach to disaster management involving healthcare practitioners. Demonstrate understanding of the role of Respiratory Therapists in disaster response and emergency management; and, describe the role of Respiratory Therapists as volunteers for disaster response. Objectives Explain the various levels of equipment and support Respiratory Therapists will utilize in responding to mass casualty incidents and disasters. Discuss the implication of Pandemic Influenza as it relates to planning and response capability and capacity. Describe the impact of Bioterrorism and manmade disasters to health care systems, providers, and disaster preparedness plans. What’s The Fuss? How Do We Respond To This… So We Don’t Feel Like This… Disaster Characteristics Increased death, injury, illness that can’t be managed Coordination public, government, and private organizations Equal triage distribution Notification of family Evacuation/Sheltering of evacuees Disaster Characteristics Media attention Heightened security; crime scene Immediate and long term emotional support Significant property damage Impact of Disasters In the past 20 years “Although the yearly death totals from disaster declined by approximately 30%, the number of people affected by disaster increased 59%” (AARC Times. 2006. p. 8) Consequence Management The objective of consequence management is: Provide support Save lives Relieve suffering Mitigate further harm Preparedness Cycle Health systems will be prepared through a continuous cycle of planning, equipping, training and exercising. Plan Train P.E.T.E. Plan Public Health Preparedness Strategic Plan Equip Ventilators, Train OSHA, PPE, Pharmaceuticals, etc… DHS, Other Exercise Local, Regional, Statewide, Interstate, National Public Health Response County Health Departments Pre-hospital Outpatient Services Hospitals Pharmacies Laboratories Mortuary Services Health Care System Surge Capacity Domestic Security Regions Region 1 Region 2 Region 3 Region 4 Region 5 Region 6 Region 7 Integrated Plans Federal National Response Framework (NRF) Supported by National Incident Management System (NIMS) and the National Disaster Medical System (NDMS) Comprehensive Emergency Management Plan (CEMP) Provides guidance Integrated and coordinated response Emergency Support Functions (ESF-8) Follows NRF Integrated Plans State Florida Department of Health Bomb, Blast, Burn (B3) Biological (B4) Pandemic Influenza Public Health and Medical Preparedness Strategic Plan 2007-2010 County CEMP Plans Hospital CEMP Plans Goal of Surge Thinking Maximize survival for all players! Minimize morbidity! Maximize resource utilization! Will require new thinking! Natural Disasters Natural Disasters Tornadoes Forest Fires Floods Blizzards Cyclones/Typhoon Hurricanes Heatwave Tsunami Volcanic Eruption Earthquakes Mudslides Limnic Eruption Draught/Famine Hail Natural Disasters - Florida Hurricanes Tornadoes Forest Fires Flooding Freezing Sinkholes Drought Heatwave Hail Natural Disasters - Florida 2004 July 31 to December 3 9 Hurricanes; 5 Tropical Storms Charley, Frances, Jeanne, Ivan 2005 June 8 to January 6 15 Hurricanes; 12 Tropical Storms Katrina, Rita Cost – 2004 Hurricane Season Florida’s hospitals incurred $163.2 million in unexpected costs Expenses related to facility modifications to reduce damage from future storms would exceed $48 million Average hospital impact of more than $1 million Total impact on hospitals > $200 million Lessons Learned Preparation Facility Planning Power, Medical Gases, Water, Etc. Flood zone Material Resources Communication Redundancy Contingency plans Incident Command! Lessons Learned Workforce issues Adequate staff Hospital Planning Incident Command Education/Training Special Needs Behavior Health Patient & Employee Lessons Learned Hospital Security Facility support Protective measures Patient Safety Mutual Aid Public and private partners Medivac Man-Made Disasters Unintentional / Accidental Engineering Failures Transportation Planes, Trains, Automobiles, Shipping Environmental Bridges, Buildings, Dams Oil spills, pollution, waste runoff Explosions Mine disasters Industrial accidents War Fire Terrorism Poking skunks is dangerous! Terrorism The goals of terrorists are to: Create confusion, fear, chaos, and mistrust. Break down the physical and political infrastructure. Intimidate, subjugate, and weaken authority. HOW WILL OUR ENEMIES FIGHT US? UNCLASSIFIED Chemical Biological Radiological A Weapon of Mass Destruction is a device or material specifically designed to produce casualties or terror. CBRNE incidents may result from industrial accidents, acts of war, or acts of terrorism. Nuclear Energetics / Explosives Chemical Agents Mustard gas Sarin Phosgene Cyanide Chlorine Chemical Agents Industrial Chemicals Warfare Agents Choking Agents Blood Agents Blister Agents Nerve Agents Exposure To Chemicals Routes of exposure Inhalation, skin contact, ingestion, injection Effect depends on dose Larger dose: earlier and more severe effects Effects may be immediate or delayed Individual susceptibility varies Age, chronic illness, medications Biological Agents: Undetectable by human senses + Prolonged incubation period + Limited surveillance capability = Unrecognized exposure Bio-threats Biological agents may be: Bacteria Viruses Toxins They are naturally occurring and / or can be bioengineered as Weapons of Mass Destruction. Routes of Transmission Absorption: Skin and mucus membranes Inhalation Respiratory through air droplets Ingestion Gastrointestinal through consumption of food or drink Injection From needle or other object Vectors Letters / packages Insects / animals Contaminated food / water Contaminated clothing Air via aerosol dissemination device CDC Category A Agents Anthrax (Bacillus anthracis) Botulism (Clostridium botulinum toxin) Plague (Yersinia pestis) Smallpox (Variola major) Tularemia (Francisella tularensis) Viral Hemorrhagic Fevers (Filoviruses [e.g., Ebola, Marburg] and Arenaviruses [e.g., Lassa, Machupo]) Nuclear / Radiological Agents Any source that emits radiation Radiation Exposure External – deposited on skin Internal – inhaled, swallowed, absorbed through skin, or introduced through wounds of radioactive materials – uptake by body cells, tissues, or organs such as kidney, liver, and bone Incorporation Symptoms of Radiation Exposure Nausea Vomiting Diarrhea Changes in mental status Early Detection Is your key to limiting potential exposure. Time is a huge factor in how much exposure one could receive. Radiation Penetration Alpha - a Beta - b Gamma - g Image Source http://www.awe.co.uk/ Neutron - n Dirty Bomb vs. Atomic Bomb The atomic explosions that occurred in Hiroshima and Nagasaki were conventional nuclear weapons involving a fission reaction. A dirty bomb is designed to spread radioactive material and contaminate a small area. Terrorist Attacks So called suicide attacks Unfortunate experience and expertise from Israel Use of explosives and shrapnel (bolts, nails, nuts) Predominate injury is lung injury (blast injury) 50% of patients who survive to hospitalization develop ARDS and require mechanical ventilation Terrorist Attacks 20 attacks > 10 wounded Total of 1475 wounded, 92 ICU admissions, 80 patients requiring MV 52% of patients had acute lung injury Blast injury is the major mechanism Aschkenasy-Steuer et al Crit Care 2005;9:1186 Terrorist Attacks 1983-2004 all multiple casualty events 875 patients from 31 events in Jerusalem Average of 28 patients per event ICU admission 5% (n=43) - of these70% had blast lung injury 73% of patients required mechanical ventilation Avidan V, J Trauma. 2007 May;62(5):1234-9. Plausible Scenarios Trauma – natural or man-made Nerve agents – sarin, tabun, VX, soman Pulmonary Irritants – phosgene, ammonia Biologic Agents – plague, tularemia, anthrax, botulism Radiologic Events – nuclear weapon, dirty bomb Plausible Scenarios SCENARIO TIME TO MV DURATION OF MV VICTIMS NEED FOR MV Immediate Days to weeks < 100 Hemo – pneumothorax, blast injury, burns smoke inhalation Nerve Agent Immediate Hours Up to 1000 Paralysis, bronchospasm, bronchorrhea Pulmonary Irritants Hours Days to weeks Up to 1000 ARDS, pulmonary edema, airway injury Biologics Hours to days Days to weeks 1000 ARDS, hemorrhagic pulmonary edema Radiologic Days to weeks Days to weeks Hundreds Traumatic lung injury, sepsis, Trauma Rubinson L, Biosecur Bioterror. 2006;4(2):183-94. Vulnerabilities Hard Targets Military instillations Government buildings Secure Areas Soft Targets Hospitals Schools Churches Prevention Efforts Rely on: Federal, State, & Local Law Enforcement Agencies Hospital Hazard Vulnerability Assessments Accreditation and Regulatory Authorities Diligence, Observation, Reporting Safety Committees >>> Performance Improvement Probability vs. Impact NUCLEAR WEAPON BIOLOGICAL AGENT IMPROVISED NUCLEAR DEVICE POTENTIAL IMPACT RADIOACTIVE MATERIAL PROBABILITY/LIKELIHOOD CHEMICAL AGENT OR TOXIC INDUSTRIAL CHEMICAL Pandemic Influenza Is it here yet? Natural Biologic Threat What is a pandemic? The spread of disease over a wide geographic area affecting much of the population Natural Biologic Threat Pandemic Influenza Increased morbidity (sickness) and mortality (death) Social disruption Economic disruption Seasonal vs. Pandemic Flu Seasonal Pandemic Yearly Rarely Familiar New virus Mild/Moderate Symptoms Very young, very old; Health problems Vaccine available virus Severe symptoms Healthy people No vaccine Influenza Disease Characteristics Inflammation of the respiratory system Headache Fever Chills Cough Muscle aches Several days sick, several weeks recovering Pan Flu Stats Pandemic Influenza History 1918 1957 1968 Frequency 50 – 100 million deaths 2 million deaths 1 million deaths ~ every 35 years Duration 1 – 3 years Worldwide 6 – 9 months, 3 months? Waves 1 – 3, 4 – 8 weeks/wave National Strategy 1. Stop, slow or otherwise limit the spread of a pandemic to the United States 2. Limit the domestic spread of a pandemic, and mitigate disease, suffering and death 3. Sustain infrastructure and mitigate impact to the economy and the functioning of society U.S. Planning Assumptions Attack rate Treatment rate Hospitalization rate Case fatality rate Pre/asymptomatic transmission Incubation period 35% of population 25% of population ~75% of cases 10% of cases 2% (2% - 50%) 30% - 50% (?) 2 days (1 – 8 days) Florida Planning Assumptions Cases Hospitalized (10%) Surge Beds (130%) ICU ICU Ventilator Surge Ventilators Dead (2%) Florida population: 18.3 million 1st Wave/2nd Wave Total 3.2 million 6.4 million 320,000 65,000 640,000 48,000 24,000 5,000 64,000 128,000 Plan Components Rapid Response Isolation & Quarantine Social Distancing Non-Pharmaceutical Interventions Pharmaceutical Interventions On-going Planning Issues Community Interventions Hospital Planning Support Alternate Medical Treatment Sites Mass care with limited supplies and resources Current Situation Human Deaths* 353 cases, 221 deaths (62.2% Mortality) 14 countries Bird Deaths 150 – 200 million bird deaths >50 countries (Asia, Europe, Africa) *WHO, 24 January 2008 Respiratory Care Your Role In A Disaster Healthcare Considerations Adequate bed space ICU Capability and Capacity Workforce reduction Options Pharmaceutical stockpiles Material resource utilization Continuity of quality Standard of Care Command & Control / Security Plan Infection Control Employee and Community Education Financial Challenge Healthcare Considerations External Influences Social & Economic Disruption Mutual aid difficulties School and Child Welfare issues Internal Influences Employee Issues Single parent families Both parents work in health care Children sick, parent / employee(s) not working Hospital Issues Patient Volume High-volume demand for medical attention Competition for scarce medical resources Impact on caregivers Need for psychological support Need for security Material Resource Management IV Tubing Lab Resources Pharmaceutical IV Fluids Antibiotics Antiviral Vaccine Mechanical Ventilators Medical Gas supply Food Services Environmental Service supplies Linens The Gas Source Issue The Gas Source Issue What is the best source of oxygen? What about home health agencies and their patients? Power is an issue! Necessary Ventilator Features for Each Scenario? Where will mechanical ventilation be performed? Who will perform mechanical ventilation? Where will the gas supply come form? How long will it last? Does the ventilator’s capabilities match the needs of the patient, skill of the operator? Necessary Ventilator Features for Each Scenario? Most mass casualty injuries result in ARDS All scenarios except nerve agent exposure require constant volume delivery, control of airway pressures, monitoring, alarms, and control of PEEP and FIO2 When nerve agents result in paralysis – airway control and short term ventilation – “good air in – bad air out” may be all that is necessary Ventilator Characteristics FDA approved for adults/peds Ability to operate without compressed gas Battery life 4 hrs Volume control CMV and IMV PEEP to 20 cm H2O Utilize both high and low pressure O2 sources Control of RR, PEEP, VT, Flow or I:E Monitor Paw and VT Alarms Disconnect, apnea, high/low pressure, high pressure source gas disconnect Ventilator Characteristics Rugged Light weight (<10kg) Easy to use Gas consumption low Battery life - long Easy to trigger < $10 K Vendor support and longevity Maintenance Training Critical Factors In a MCI – many patients will need ventilation exceeding not only equipment but staff capabilities Likely that critical care RRT will supervise noncritical care RRT and others in care of the ventilated patients The ventilator must have adequate alarms and monitoring The ventilator must have a simple interface and be easy to use Specific Devices Concerns Education and training Universal response Decentralization of supplies and equipment Operability in MCI environments Safety Age capability Compensation Legal protection Communications Vulnerable Populations Volunteerism FEHVR Florida Emergency Health Volunteer Registry, the Florida Department of Health online system for health care providers and other private volunteers. https://www.servfl.com/ Medical Reserve Corps Mission: To augment local community health and medical services with pre-identified, trained and credentialed volunteers during emergency medical operations and vital public health activities. Purpose: The Florida Medical Reserve Corps (MRC) Network was established for the purpose of effectively facilitating the use of health professional volunteers in local, state, and federal emergency responses in every county within Florida. Licensure Renewal Statement If you are renewing to active status, would you be available to provide health care services in special needs shelters or to help staff disaster medical assistance teams during times of emergency or major disaster? □ Yes Other Issues Disaster Implications Communities Food, Water, Shelter Power Economic and Social Disruption Child Safety Domestic Animals Personal Property Damage Disaster Implications Patient Populations Food, Water, Shelter Power for medical equipment Medications Renal Dialysis Increase hospital surge! Healthcare Impacts Road Closures Hospital Closures / Evacuation Workforce Shortage Resource Management HVAC Water, Food Sanitation Supplies Management Surrounding Issues Just-In-Time Inventory Access Equipment & Supplies Vent Circuits Aerosol and Humidity Medications Oxygen Supplies Other Medical Supplies Infrastructure Support Mutual Aid Agreements Vendor Agreements Hospital Agreements Government Agreements Local (i.e. – City, Municipality, County) Regional State / Inter-State Federal Infrastructure Support Workforce & Staffing Personal Plan PPE Plant Facilities Security Plans Facility Safety Communication Devices Phones: cell, satellite, land based 800 mgHz / MED Radios Pagers Overhead paging systems Dispatcher Email HAM Radio Special Populations This is an everyday issue for hospitals on a small scale. We need to plan to support large numbers of persons who are hard to reach or have disabilities. Deadly Misconceptions “It won’t happen here” It won’t happen to me” “Someone else will take care of it” Q & A? Thank You! Acknowledgements The 2008-2009 Florida State Working Group Ventilator Capability Team members are: John Wilgis, MBA, RRT - Florida State Working Group Ventilator Capability Team Chair, Director, Emergency Management Services, Florida Hospital Association Melanie McDonough, MSHS, RRT - Florida State Working Group Ventilator Capability Team, Education SubGroup Chair, Director of Clinical Education, Cardiopulmonary Sciences, University of Central Florida Scott Kirley, RRT - State Working Group Ventilator Capability Team, Equipment Sub-Group Chair, West Centrak Florida Disaster Services, Inc. Mary Martinasek, MPH, RRT-NPS, RPFT, AE-C - Florida State Working Group Ventilator Capability Team, Response Sub-Group Chair, American Public Health Student Assembly- Secretary Kris-Tena Albers, ARNP, CNM, MN - Florida State Working Group Ventilator Capability Team Liaison, Public Health Preparedness Hospital Liaison, Florida Department of Health Dr. Jennifer Bencie Fairburn, MD, MSA, Director, Division of Emergency Medical Operations, Florida Department of Health Dr. David V. Shatz, MD, FACS - Professor of Surgery, Trauma Surgery/Surgical Critical Care, University of Miami Paul Stephan, MPS, RRT - Program Director, Respiratory Care, Santa Fe Community College Randy De Kler, MS, RRT - Program Director, Respiratory Care, Miami Dade College Phil Khan, RRT - Florida Society for Respiratory Care Sandra J. Barker, MS, RRT - Director, Cardiopulmonary Services, Largo Medical Center Timothy J. Coons - Director, Cardio-Pulmonary Services, Shands Hospital at the University of Florida Bill Cunningham, BS, RRT - Adult Critical Coordinator, Cardiopulmonary Services, Shands Hospital at the University of Florida Joseph Albino, BS, RRT - Manager, Respiratory Care, Mease Dunedin Hospital Kelly Sebree, RRT, NPS - Director, Respiratory Care, Lawnwood Regional Medical Center References: Anonymous. (2006). Ventilation for Life – Mechanical ventilators in Mass Casualty Incidents. AARC Times. 30(3), 8-11. Anonymous. (2007). List of Disasters. Wikipedia. The Free encyclopedia. Retrieved 8/14/07 from: http://en.wikipedia.org/wiki/List_of_disasters Barnett, D.J., Balicer, R.D., Blodgett, D. Fews, A.L., Parker, C.L., Links, J.M. (2005). The Application of the Haddon Matrix to Public Health Readiness and Response Planning. Environmental Health Perspectives. 113(5), 561-566. Branson, R. (2007). Augmenting Positive Pressure Ventilation Capacity. AARC Summer Forum Journal Conference Presenation. Bunch, D. (2006). Are We Ready for the Worst? AARC Times. 30(3), 36-44. Committee Working Document. (May 2005). Florida HRSA National Hospital Bioterrorism Preparedness Program FY05 Projects. Carlton, P.K. (May 30, 2007). A Culture of Preparedness. Texas A&M University. Health Science Center. Retrieved June 30, 2007 from: www.tamhsc.edu/homeland/ References: Florida Hospital Association. (May. 2005). Eye of the Storm: Impact of the 2004 Hurricane Season on Florida Hospitals. Retrieved 6/30/07 from: http://www.fha.org/protected/hospitalpreparedness.html Hall, B. (2007). Dirty Bombs. Eastern Shore (VA) Health District. Retrieved from personal email. Rubinson, L., O’Toole, T.O. (2005). Critical care during epidemics. Critical Care. Vol. 9. BioMed Central Ltd. Published on-line 4/27/2005 at http://ccforum.com/inpress/cc3533 Rubinson, L., Nuzzo, J., Talmor, D., O’Toole, T., Kramer, B., Inglesby, T. (2005). Augmentation of hospital critical care capacity after bioterrorist attacks or epidemics: Recommendations for the Working Group on Emergency Mass Critical Care. Critical Care Medicine. 33(10), E1-13. State of Florida, Department of Health, Division of Emergency Medical Operations. Office of Public Health Preparedness (2007). Working Together for a Safe and Secure Future: Florida Public Health and Medical Preparedness Strategic Plan 2007 – 2010. Retrieved June 30, 2007 from Florida Department of Health. References: State of Florida, Division of Emergency Management. (2007). Public Information. Retrieved June 30, 2007 from: www.floridadisaster.org Tynan, B. (2007). Pandemic Influenza: Healthcare Planning. Florida Department of Health. Retrieved through personal email. U.S. Department of Health and Human Services. (2007). Federal Planning & Response Activities. Retrieved 7/1/07 from: http://www.pandemicflu.gov/plan/federal/index.html U.S. Department of Health and Human Services. (2007). State and Local Government Planning & Response Activities. Retrieved 7/1/07 from: http://www.pandemicflu.gov/plan/states/index.html U.S. Department of Homeland Security, Federal Emergency Management Agency (2007). Introduction to Incident Command System. Emergency Management Institute. Retrieved 6/30/2007 from: http://emilms.fema.gov/