Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
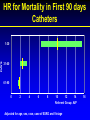
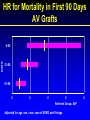
Transitions of Care in ESRD Patient Management Improving Handoffs Antonia Harford, MD UNM Nephrology OBJECTIVES • Review Epidemiology of ESRD – Mortality/Hospitalization in ESRD • Transitions of care in ESRD: – Discharge Handoffs • Future Collaborations – Communication at transfer – Nurse navigator ESRD Patient counts, by modality Incident & December 31 point prevalent ESRD patients. Total Medicare ESRD expenditures, by modality Period prevalent ESRD patients, patients with Medicare as secondary payor are excluded. USRDS 2011 • ESRD patients have higher rates of hospitalization and mortality than age matched controls in general population • 20% of ESRD pts account for 80% ESRD Medicare expenditure All-cause standardized hospitalization & mortality ratios in large dialysis organizations, 2009 Figure 10.19 (Volume 2) January 1 point prevalent hemodialysis patients with Medicare as primary payor (SHRs); January 1 point prevalent hemodialysis patients (SMRS). SHRS & SMRS are calculated based on national hospitalization & death rates; adjusted for age, gender, race, & dialysis vintage. ESRD • Mortality • Hospitalization – Cardiovascular – Cardiovascular • Sudden Death • CHF • CAD • Fluid overload – Stroke – Infection • Vascular Access • Pneumonia – Withdrawal from dialysis – Vascular Access Cx – Infection • Vascular Access • Pneumonia – Hyperkalemia – Fracture Time-series curves for death A:Modifiable factors B: Fixed factors Chan K E et al. CJASN 2011;6:2642-2649 ©2011 by American Society of Nephrology Change in adjusted all-cause & causespecific hospitalization rates, by modality Figure 3.1 (Volume 2) Period prevalent ESRD patients. Adj: age/gender/race/primary diagnosis; ref: ESRD patients, 2005. Incident HD pts (n = 303,289), A: relative risk of death B: Hospitalization Relative risk of A: death and B : Hospitalization at each 1week interval compared with a reference group of patients who survived the first year of dialysis Chan K E et al. CJASN 2011;6:2642-2649 ©2011 by American Society of Nephrology Access events & complications in prevalent dialysis patients (CPM data; rate per patient year) Table 2.c (Volume 2) Catheter, fistula, graft: prevalent hemodialysis patients age 20 & older, ESRD CPM & claims data. Peritoneal dialysis device: prevalent peritoneal dialysis patients age 20 & older. Access use at first outpatient hemodialysis, by preESRD nephrology care, 2009 Incident hemodialysis patients, 2009. HR for Mortality in First 90 days Catheters DAYS 1-30 31-60 61-90 0 2 4 6 8 10 12 14 Referent Group: AVF Adjusted for age, sex, race, case of ESRD and Vintage 16 HR for Mortality in First 90 Days AV Grafts DAYS 0-30 31-60 61-90 0 2 4 6 Referent Group: AVF Adjusted for age, sex, race, case of ESRD and Vintage 8 Associations of pneumococcal vaccination & Mortality and Hospitalization Gilbertson D T et al. Nephrol. Dial. Transplant. 2011;26:2934-2939 © The Author 2011. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For Permissions, please e-mail: [email protected] Cause-specific rehospitalization rates in the 30 days following live hospital discharge, by age, 2009 Figure 3.4 (cont.; Volume 2) Period prevalent hemodialysis patients age 20 & older, 2009; unadjusted. Includes live hospital discharges from January 1 to December 31, 2009. Medical Errors & ESRD • Poly-pharmacy • Multiple providers • Multiple handoffs Cumulative number of medications in Part D-enrolled ESRD patients, by race/ethnicity & low income subsidy (LIS) status, 2008 ) Point prevalent Medicare enrollees alive on January 1, with Part D enrollment, October 1–December 31, 2007 & 2008. The Bundle & ESRD Medications • Presently the dialysis units bundle the cost of outpatient dialysis related injectables as part of the “Bundle” • In 2014, the outpatient dialysis facility will dispense all outpatient meds associated with dialysis Top 25 drugs used by Part D-enrolled dialysis patients by frequency & net cost, 2008 Part D claims for all dialysis patients, 2008. ESRD Discharge • Multiple handoffs, because of: – Multiple co-morbidities – Poly-pharmacy – Multiple providers – Multiple levels of care Unforeseen consequences • Reduction in trainee work hours did not result in the expected decrease in medical errors • Reduction in trainee work hours had resulted in an increased # of hand-offs: Rates of All Harms, Preventable Harms, and High-Severity Harms per 1000 Patient-Days, Identified Rates of All Harms, Preventable Harms, and High-Severity Harms per 1000 Patient-Days, Identified by Internal and External Reviewers, According to Year. by Internal and External Reviewers, According to Year. Landrigan CP et al. N Engl J Med 2010;363:2124-2134. Hand/Offs • Considerations: – What is the most effective H/O? • Telephone, email, text, EMS – How do we teach H/O? – Who is responsible for H/O? • Trainee, nurse navigator, attending – Identify patients at increased risk for medical error at H/O Inter facility Transfer form Transitional Care Models: Decreasing LOS & Hospital Days • Disappointing results with reducing hospital admission & readmission rates • Among CKD patients initiating dialysis, those enrolled in a multidisciplinary CKD care model had a significantly lower mean hospital days compared to controls OBJECTIVES • Review Epidemiology of ESRD – Mortality/Hospitalization in ESRD • Transitions of care in ESRD: – Discharge Handoffs • Future Collaborations – Communication at transfer – Nurse navigator Future Directions – Promoting communication at transitions of care – Improving Handoffs: Bidirectional – Health care navigators: DCI CMS Innovation Grant Collaboration in Transitions of Care in ESRD • Hypothesis: Collaboration between Hospitalist & Renal services utilizing Nurse navigators will decrease LOS & total hospital days Collaboration in Transitions of Care in ESRD • Specific Aim 1: Identify the 20% ESRD pts with frequent re-admissions to UNMH. Randomize 50/50 to usual care vs Nurse navigator • Specific Aim 2: Compare Missed HD treatments, ER utilization , hospital admission, readmission, LOS, total hospital days between groups