Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
RHEUMATOID ARTHRITIS
RA- Epidemiology/ Genetics
Most common inflammatory arthritis
Prevalence: 0.8 % of population ( increasing
prevalence with age)
M:F 1:3
Age range: 4th to 5th decade
Genetic predisposition: HLA DR4, HLA DR1,
HLA DR3
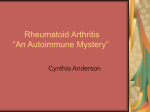
The progression of Rheumatoid Arthritis
Pathogenesis of
rheumatoid
arthritis. The figure
summarizes some of
the cytokines and
cellular interactions
believed to be
important in RA. The
molecular targets for
biologic agents
currently used in the
treatment of RA are
shown. It is thought
that TNF plays a
particularly
important role by
orchestrating
production of other
cytokines. (IL =
interleukins; MMP =
matrix
metalloproteinases;
PGE = prostaglandin
E; TCR = T-cell
receptor; TNF =
tumour necrosis
factor; VEGF =
vascular endothelial
growth factor)
Clinical
Manifestations
Summary:
Major Pathologic Features
Rheumatoid arthritis
Systemic
Chronic inflammation of synovial membrane
Associated progressive destruction of articular/
periarticular structures
Subcutaneous nodules
Extra-articular manifestations
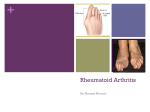
Progression of RA
Early
Middle
Late
Progression of RA
Mild
© The Arthritis Foundation
Moderate
Severe
ACR 1987 CLASSIFICATION CRITERIA FOR
RHEUMATOID ARTHRITIS
Requires four out of the seven criteria:
1. Morning stiffness*
2. Arthritis of three or more joints*
3. Arthritis of hand joints*
4. Symmetric arthritis*
5. Rheumatoid nodules
6. Serum rheumatoid factor
7. Radiographic changes
*Must have been present for at least six weeks
Clinical features
Presentation is with pain, joint swelling and
stiffness affecting the small joints of the hands,
feet and wrists.
Large joint involvement, systemic symptoms and
extra-articular features may also occur.
The typical features are symmetrical swelling of
the metacarpophalangeal (MCP) joints and
proximal IPJs.
These and other joints are actively inflamed if
they are tender on pressure, and have stress pain
on passive movement or effusion/soft tissue
swelling.
Clinical features
Erythema is not usually a feature and its
presence implies coexistent sepsis.
Characteristic deformities develop with longstanding disease, including 'swan neck'
deformity, the boutonnière or 'button hole'
deformity, and a Z deformity of the thumb
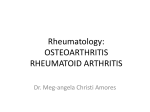
Swan neck deformity
Ulnar deviation of the
fingers with wasting of
the small muscles of
the hands and synovial
swelling at the wrists,
the extensor tendon
sheaths, the
metacarpophalangeal
and proximal
interphalangeal joints.
Clinical features
In the foot, dorsal subluxation of the MTP
joints may result in 'cock-up' toe deformities.
This causes pain on weight-bearing on the
exposed MTP heads and development of
secondary adventitious bursae and callosities.
In the hindfoot, calcaneovalgus (eversion) is
the most common deformity, reflecting
damage to the ankle and subtalar joint.
This is often associated with loss of the
longitudinal arch (flat foot) due to rupture of
the tibialis posterior tendon.
Clinical features
Popliteal ('Baker's') cysts usually occur in
combination with knee synovitis.
Synovial fluid communicates with the cyst
but is prevented from returning to the joint
by a valve-like mechanism.
Extraarticular Manifestation
Rheumatoid Nodules
Vaculitis
Pleuropulmonary manifestations
Peripheral neuropathy
Episcleritis, keratoconjunctivitis sicca
Felty’s Syndrome : chronic RA, splenomegaly,
neutropenia, anemia
Osteoporosis
RA – Laboratory Evaluation
No specific test for RA
RA factors- found in 2/3 of RA adult
Seen in 5 % of healthy subjects
10-20% among >65 years old
Can be positive in SLE, Sjogren’s, chronic liver disease,
sarcoidosis, interstitial pulmonary fibrosis, infectious
mononucleosis, hepatitis B, TB, Leprosy, syphillis,
SBE, visceral leishmaniasis, schistosomiasis, malaria
High titers signifies poor prognosis/ extraarticular
manifestations
Rheumatoid Factors
Fc
Fab
IgG
IgG
Fc
Fab
IgM RF
ACR
IgG
IgG RF
RA – Laboratory Evaluation
Anti –CCP (anti-cyclic citrullinated peptide antibody)
More specific but same sensitivity to RA factor
Associated with HLA beta1
ESR
Increased among majority of RA patients
CBC
Anemia ( Normocytic normochromic)
Radiographic Changes
Juxtaarticular osteopenia
Loss of articular cartilage and erosions
Management
Of Rheumatoid arthritis
Objectives of RA Treatment
• Relieve pain
• Decrease joint inflammation
• Prevent joint destruction
• Restore function of disabled joints
• Correct deformed joints
• Maintain quality of life
Management
Physical rest, targeted anti-inflammatory
therapy and passive exercises are the
mainstays, with the aim of relieving
symptoms, suppressing inflammation, and
conserving and restoring function in affected
joints.
A multidisciplinary approach is required,
including doctors, nurses, physiotherapists
and occupational therapists, and patient
education and counselling play a key role.
Management
During treatment, periodic assessment of
disease activity, progression and disability is
essential.
In the vast majority, management is
outpatient-based, but hospital admission can
be helpful in patients with very active disease
for a period of bed rest, multiple joint
injections, splinting, regular hydrotherapy,
physiotherapy and education.
Mx- Drug therapy
Prompt introduction of DMARD therapy plays
a central role.
The patient should be advised that this will
not improve symptoms immediately, but in
the longer term there is a good chance that
symptoms will come under control and joint
damage will be prevented.
If the first-choice drug fails to control disease
activity, other DMARDs can be added
Mx-Drug therapy
If adverse effects occur, the patient should be
switched to another DMARD.
If disease activity persists despite an adequate
trial of two DMARDs including methotrexate,
anti-TNF therapy should be considered.
Most patients also require NSAID and other
analgesics.
Because of the delayed onset of action,
corticosteroids are often given when DMARDs
are commenced to give symptomatic relief.
MANAGEMENT OF RHEUMATOID ARTHRITIS:
Some Disease-modifying Anti-rheumatic Drugs (DMARDS)
DMARD
Methotrexate
Hydroxychloroquine
Sulfasalazine
Leflunomide
Azathioprine
Cyclosporine
Gold
MONITORING
Hematologic, lung, liver (avoid alcohol)
Ophthalmologic
Hematologic, GI
Hematologic, liver
Hematologic, liver
Renal, blood pressure
Hematologic, renal
MANAGEMENT OF RHEUMATOID ARTHRITIS:
Symptomatic Medications
NSAIDs
Analgesics
Corticosteroids
Surgery in RA
Synovectomy of the wrist or finger tendon
sheaths of the hands may be required for pain
relief or to prevent tendon rupture when
medical interventions have failed.
In later stages when joint damage has
occurred, osteotomy, arthrodesis or
arthroplasty may be required.
Possible Causes of Premature
Death in RA
• Chronic inflammation results in accelerated
atheroclerosis leading to stroke or myocardial
infarction
• Renal disease
• Respiratory disease
• Gastrointestinal disease
• Infection