Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
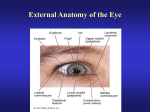
Anatomy & Physiology of Vision 1. Describe the anatomy of the eye, orbit and visual pathways and the physiology of vision. The eyeball is within the orbit consisting of the lacrimal, maxilla, zygomatic, frontal, sphenoid and ethmoid bones. These bones also provide protection for the eyeball. There are 6 extrinsic muscles of the eyeball and they are attached to the orbit as well as the eyeball. There are 4 rectus (straight muscles) that move the eye up and down or side to side. There are 2 oblique (slanted) muscles that rotate the eye. The cranial nerves that innervate these muscles are CN 3, 4 and 6 (oculomotor, trochlear and abducens) The eyeball has 3 layers – sclera, choroid and retina. The sclera is the thickest layer and is made of fibrous connective tissue. It is the visible white part of the eye. The anterior part of the sclera is the cornea. It differs because it is transparent, has no capillaries, covers the iris and pupil and is the first part of the eye that refracts (bends) light. The choroid layer contains the blood vessels and a dark blue pigment that absorbs light and prevents glare. The anterior portion contains 2 parts, the ciliary body and the iris. The ciliary body is a circular muscle that surrounds the lens, connected by suspensory ligaments. The lens is made of a transparent, elastic protein and has no capillaries. The shape of the lens is changed by the ciliary muscle that enables light to be focused. The iris is the coloured part of the eye, the colour being derived from melanin. It is genetically determined. There are 2 sets of smooth muscles that change the diameter of the pupil (radial and circular fibres). The radial fibres dilate the pupils and this is a sympathetic response. Circular fibres constrict the pupils and this is a parasympathetic response. The retina lines the posterior 2/3rds of the eyeball and contains the visual receptors called the rods and cones. Rods detect the presence of light and cones detect colours. Rods are more abundant at the periphery of the retina, cones are more abundant at the centre of the retina. An area called the fovea only contains cones and is the best area for detecting colour. There are 2 cavities within the eyeball – the anterior and posterior cavities. The posterior cavity is between the lens and the retina and contains vitreous humor. It is a semi-solid liquid that keeps the retina in place. The anterior cavity is between the back of the cornea and the front of the lens and contains aqueous humor. It is the tissue fluid of the eyeball and is formed by the capillaries in the ciliary body. It flows anteriorly through the pupil and reabsorbed by the sclera venous sinus (canal of Schlemm) which is found at the junction of the iris and cornea. The eye is nourished by this aqueous humor. Physiology of Vision This involves light rays being focused on the retina and nerve impulses being transmitted to the visual areas of the cerebral cortex in the brain. Refraction of light follows the path of cornea, aqueous humor, lens and vitreous humor. The lens is the only adjustable part of this refraction system. When looking in the distance the ciliary muscle is relaxed and the lens is elongated and thin. When looking at nearer objects the ciliary muscle is contracted to form a smaller circle, the lens recoils and bulges in the middle and now has greater refractive power. When light rays strike the retina, they stimulate chemical reactions in the rods and cones. In rods, the chemical rhodopsin breaks down to form scotopsin and retinal (derivative of Vit A). This chemical reaction generates an electrical impulse and rhodopsin is then resynthesised in a slower reaction. Adaptation to darkness (going outside at night) may take a while because if you’ve come from a well lit area, most of the rhodopsin has already been broken down and the resynthesising is slow. In the opposite situation where you are woken up to a bright light, it can seem painful because in the dark all your rhodopsin in your rods has been resynthesised and when you suddenly awaken to a bright light, all the rhodopsin is broken down at once which generates a lot of impulses. This intensity of impulse generation may be interpreted in the brain as pain. After a few minutes, it’s not so painful because the rhodopsin is being resynthesised again. There are 3 types of cones and retinal plays a role in the generation of impulses from cones. There are red-absorbing, blue absorbing and green absorbing cones. The impulses generated in rods and cones are transmitted to ganglions which converge at the optic disc to form the optic nerve. The optic nerves come together at the optic chiasma just in front of the pituitary gland. The medial fibres cross over to the other side, the lateral fibres stay on the same side (important for binocular vision). The visual areas are in the occipital lobes of the cerebral cortex. The visual areas integrate the images from each eye and produce a single image that has depth and 3-dimension. The visual areas also right the image because the image on the retina is upside down. 2. Outline the mechanisms by which the visual pathway can be damaged and describe the types of visual field defects that may result. This is taken exactly from the lecture notes, sorry I didn’t go and research some more but I’m guessing the list of visual field defects are numerous so the ones in the lectures are the ones they can examine on. Visual field defects can be classified into 2 types: Homonymous – similar regions affected in each eye. E.g. right visual fields of both eyes Heteronymous – different regions affected in each eye. E.g. left visual field of one eye and right visual field of the other eye. Specific Deficits: Monocular blindness – blindness in one eye due to optic nerve lesion before the optic chiasm Bitemporal (heteronymous) hemianopsia – loss of temporal visual fields of each eye due to lesion at the optic chiasm Nasal hemianopsia – loss of nasal vision in one eye due to lesion in lateral edge of optic chiasm Homonymous hemianopsia – loss of left or right visual fields for both eyes due to lesion in right optic tract Upper left quadrantanopsia – loss of vision in left upper quadrant of each eye due to lesion in Meyer’s loop Lower left quadrantanopsia – loss of vision in lower left quadrant of each eye due to lesion in medial fibres of visual tract.