Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
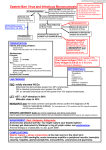
Epstein Barr Virus in Immunosuppressed Host Epstein Barr Virus = Human herpesvirus 4 Infects more than 95% of the world's population. Humans are the only known reservoir of Epstein-Barr virus. EBV is present in oropharyngeal secretions and is most commonly transmitted through saliva. The virus replicates in nasopharyngeal epithelial cells. Viral replication viremia lymphoreticular system, including the liver, spleen, and B lymphocytes in peripheral blood. Host immune response to the viral infection includes activation of CD8+ T lymphocytes = atypical lymphocytes found in the peripheral blood. The T lymphocytes kill EBV-infected B cells and eventually reduce the number of Epstein-Barr virus–infected B lymphocytes to less than 1 per 106 circulating B cells. Latent viral infection of memory B cells Clinical Manifestations Most commonly associated with infectious mononucleosis Classically affects adolescents and young adults Children often asymptomatic Self-limited course Classic triad of symptoms Sore throat +/- tonsillar Exudate (85% of pts) Lymphadenopathy (usually posterior cervical chain) Present in ~100% of pts Fever! – 98% of pts ** e.g. Saturday Night Fever Splenomegaly – seen in 50% pts Rash! Generalized maculopapular, urticarial or petechial rash Erythema nodosum has been reported, but is rare Rash more common in pts treated with antibiotics (esp. ampicillin or amoxicillin) Reactive Lymphocytes! Lymphocytosis = most common lab finding Absolute count > 4500 Differential count > 50% Most pt’s have >10% atypical lymphocytes on peripheral smear = CD8+ Tcells Less common manifestations of EBV “EBV can affect virtually any organ.” Hepatitis Fulminant liver failure Jaundice is rare Glomerulonephritis/ Acute Kidney Injury Pneumonia/Pleural effusion Myocarditis Pancreatitis Myositis Hepatitis! Increased infiltration by CD8+ T cells Inflammation of the liver Transaminitis Neurologic syndromes Guillian-Barre Cranial nerve palsies Encephalitis Aseptic meningitis Transverse myelitis Optic neuritis Oral Hairy Leukoplakia! Vs. Oral Candidiasis Epstein-Barr virus serology Antibodies to Epstein-Barr virus antigens Antibodies to viral capsid antigen (VCA), early antigens (EAs) Epstein-Barr nuclear antigen (EBNA). Primary acute Epstein-Barr virus infection is associated with VCA-IgM, VCA-IgG, and absent EBNA antibodies. The antibody pattern in recent infection (3-12 mo) includes positive findings for VCA-IgG and EBNA antibodies, negative VCA-IgM antibodies, and, usually, positive EA antibodies. Patients who are immunocompromised and have persistent or reactivated Epstein-Barr virus infections often have high levels of antibodies to EA/D or EA/R. Monospot Rapid slide agglutination tests, including Monospot assays, have been developed to measure acute infectious mononucleosis heterophile antibodies in a rapid qualitative fashion. Slide tests use either horse RBCs or bovine RBCs. All commercial kits for rapid diagnosis of acute infectious mononucleosis heterophile antibodies have low sensitivity (63-84%), with a negative predictive value of more than 10%. Spot tests rarely yield false-positive results in patients with lymphoma or hepatitis. Treatment In most cases, no treatment is necessary --------------------------------------------------- Corticosteroids for tonsillar edema / respiratory distress In vitro trials of acyclovir Our patient was treated with Valcyte 900mg po q day IVIG for immune-mediated thrombocytopenia THE END