Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
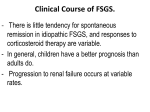
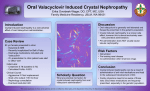
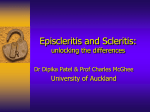
Immunoglobulin A Nephropathy as a Systemic Underlying Cause of Bilateral Anterior Scleritis Aruoriwo Oboh-Weilke, MD Florian A. Weilke, MD InnovisHealth Fargo,ND PURPOSE We report a case of a patient who presented with a bilateral anterior scleritis which occured 5 months apart. The patient had been diagnosed with biopsy proven Immunoglobulin A (IGA) nephropathy 4 years prior to her ocular complication of scleritis. INTRODUCTION Scleritis is an ocular inflammatory condition caused by an immune-mediated vasculitis which results in inflammation and destruction of the sclera 1. It causes significant pain and may lead to structural changes of the globe in association with visual morbidity 1. Scleritis can be divided into four clinical types: Nodular anterior, diffuse anterior, necrotizing anterior and posterior scleritis 8 INTRODUCTION IgA nephropathy is the most common biopsy-proven pattern of glomerulonephritis worldwide 4. Both clinical and histologic factors, have been suggested to impact on prognosis 4. The clinical picture of this renal disease includes, proteinuria, acute kidney injury, and the nephrotic syndrome 4. CASE REPORT A 31 year old caucasian female was referred for an ophthalmology consultation by her internist. The patient stated she had noticed redness of her left eye for one week. This was accompanied by boring left ocular pain. The patient had seen an optometrist who started her on topical steroids. She reported worsening of the symptoms on this regimen. She then saw her internist who started her on systemic steroids and promptly referred her to the eye clinic. CASE REPORT On review of systems, the patient admitted to blurry vision, pain on eye motion and blood in her urine. On further questioning about her medical problems, she stated that she had been diagnosed and treated for IgA nephropathy for 4 years. She previously had proteinuria and microscopic hematuria as manifestations of her renal condition and had been followed by her nephrologist. Her diagnosis of IgA nephropathy had been confirmed by a renal biopsy. Her last follow-up with her nephrologist was 1 year prior to this presentation and she was noted to have a stable renal status at that time. CASE REPORT On physical examination, the patient’s VA was OD 20/25 and OS 20/40 EOM were full, however, there was pain on motion. Pupils and IOPs were normal. Slit Lamp Exam revealed diffusely inflammed temporal conjunctival and underlying scleral vessels with scleral and episcleral edema. There was minimal blanching with the application of topical phenylephrine. Dilated fundus exam was normal and did not reveal any choroidal folds RESULTS The patient was continued on the oral steroids and tapered according to her symptoms. Her symptoms resolved after 2 weeks. A work-up for more common causes of scleritis was undertaken. CBC, ESR, RF, ANA, c-ANCA, p-ANCA, uric acid and ACE levels were all negative. A 24 hour urine collection revealed proteinuria. An appointment was made for the patient to see her nephrologist, to evaluate whether there was any worsening of her renal status. RESULTS 5 months after this episode, the patient presented with similar symptoms and signs in the right eye. A diagnosis of diffuse anterior scleritis was made and she was initially treated this time with NSAIDS. She responded well and showed resolution after 1 week. OD few days after presentation DISCUSSION Scleritis is an ocular inflammatory condition that is immune-mediated. It is usually associated with an underlying systemic immunological disease in about 50% of the cases 2. Several well known etiologies are Connective tissue diseases such as rheumatoid arthritis, ankylosing spondylitis, systemic lupus erythematosus, and with vasculitidies such as Wegner's granulomatosis and polyarteritis nodosa 1. It can also be associated with infectious disease such as syphilis, tuberculosis and herpes zoster 1. There have however, only been a few reports in the literature citing IgA nephropathy as an underlying systemic cause . DISCUSSION IgA nephropathy is a renal disease that may progress over a period of 20 years to chronic kidney disease, and then to end-stage renal disease requiring renal replacement therapy 5. Studies have shown that the use of corticosteroids can reduce proteinuria and prevent progression to end-stage renal disease 7. IgA nephropathy is generally considered to be an immune-complex-mediated glomerulonephritis 6. DISCUSSION 3Nomoto et al performed a follow-up study of 113 patients all known to have various types of primary glomerular diseases. The patients were followed for 33 months to determine the clinical spectrum of primary glomerulonephritis. The study revealed six patients exhibited scleritis. All of these six patients with scleritis were noted to have IgA nephropathy. None of the other patients diagnosed with other forms of glomerulonephritis showed scleritis during the study period. This suggests that a similar autoimmune mechanism may be responsible for the manifestation of IgA nephropathy and the development of scleritis. CONCLUSION While evaluating a patient with scleritis, it is important to perform a complete review of systems and to pay close attention to the patient’s past medical history. This case report draws attention to another underlying cause of a well known ocular entity. A work-up which includes evaluation of the renal function should be entertained in patients presenting with scleritis. REFERENCES 1 External Disease and Cornea. Basic and Clinical Science Course 1999-2000; 219-224 2 Scleritis and IgA nephropathy. Arch Intern Med. 1980 Jun;140(6):783-5. 3 Scleritis in IgA nephropathy: a case report. Zhonghua Yi Xue Za Zhi (Taipei). 1995 Oct;56(4):279-82. 4 Clinicopathologic correlation in IgA nephropathy. Semin Nephrol. 2008 Jan;28(1):10-7. 5 Natural History of Primary IgA Nephropathy. Semin Nephrol. 2008 Jan;28(1):4-9. REFERENCES 6 Pathogenesis of IgA nephropathy. Contrib Nephrol. 2007;157:1-7. 7 Treatment of IgA nephropathy: corticosteroids, tonsillectomy, and mycophenolate mofetil. Contrib Nephrol. 2007;157:37-43. 8 Atlas of Clinical Ophthalmology. Mosby,2000; 5.22-5.23