Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
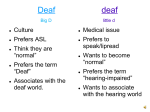
How Dysfluency Impacts Assessment © 2009 Office of Deaf Services All Rights Reserved “Psychiatry is unique among the medical fields in that most of the symptoms are conveyed by or through communication, and communication also is the primary method and nature of treatment.” Robert Q. Pollard Who We Are, Why It Matters Office of Deaf Services established 2003 Long standing interest in language issues with deaf people who have mental illness First efforts in the early 90’s DeafBlind in DD Habilitation Centers Who We Are, Why It Matters Small, “old South” rural state with limited resources Need to maximize what’s available Focus on supplementing direct services with interpreting Led to MH interpreting standard and then to trying to figure out how to deal with dysfluent consumers Improve CDI/Visual-Gestural communication services Collaboration with Neil Glickman’s program Who We Are, Why It Matters We learned that this stuff helps our clinicians too Better diagnosis Better intervention strategies Better communication strategies with consumers Able to better discuss symptoms with Psychiatrists and other hearing clinicians “Deaf – Hearing Different” Hearing Thought World Deaf Thought World Language = English Language English Language is a positive Language can indicator of intelligence indicate intelligence but not by itself Language impairment = organic disorder Language impairment likely means “no signs at home” No Language = No Sense “Those who are born deaf all become senseless and incapable of reason.” Aristotle, 355 BC In hearing people absence of language as an indicator of pathology Birth defect (mental retardation) Trauma/disease (aphasia) Exceptions were extremely rare “Wild Boy of Aveyron” Genie Language Deprivation v. Dysfluency Dysfluency is an umbrella concept Disruption of language - may be: Thought disorder/psychosis Trauma/Etiological Aphasia/TBI/Stroke/other illness or injury Cognitive Disability Developmental (i.e. lack of exposure) Language Deprivation v. Dysfluency Language Deprivation is a form of dysfluency Literally lack of exposure to language Sometimes called “low functioning” Extremely rare with hearing children – not so rare with deaf Glickman argues that it is not as common as advocates say it is Has specific markers Markers of Language Deprivation Fund of knowledge deficits Poor vocabulary Sign features formed incorrectly May be missing (Topic-comment, Clear referents, Time indicators, Grammar) Repeated signs Isolated signs/phrases 3rd person Visual space Adapted from: Glickman, Neil. 2007. The Journal of Deaf Studies and Deaf Education 2007 12(2):127-147 Deprivation or Thought Disorder? It is important to know the difference! Easy to confuse the two Diagnosis may be confounded if not clear Big trap (and clue) for many clinicians: Fund of Information/Knowledge Deficits Is FOI deficit or thought disorder? Trap: “Hearing people don’t understand it either” ignores vastly different starting places Deprivation or Thought Disorder? Thought Disorder Inappropriate facial and/or emotional expression. Bizarre language content. Behaviors suggesting hallucinations. Guardedness and volatility. Deteriorated language skills. Appearance and behavior. Language improves with medication Language Deprivation Fund of knowledge deficits Poor vocabulary Sign features formed incorrectly May be missing (Topiccomment, Clear referents, Time indicators, Grammar) Repeated signs Isolated signs/phrases 3rd person Visual space Adapted from: Glickman, Neil. 2007. The Journal of Deaf Studies and Deaf Education 2007 12(2):127-147 Make or Break Assessment The communication assessment will be crucial to treatment planning Provides basis for differential diagnosis Identifies areas where remedial work can be done Documents needs for collaterals Baseline for improvement or decompensation Helps “NFC” hearing team members understand issues A Digression: We call it a communication assessment rather than a language assessment for several reasons We are not SLPs Considers more than just language Focus on functionality rather than linguistics Assessment Questions The Big Four Severity of hearing loss Cause of hearing loss (etiology) Genetic? Syndromic? Disease? Trauma? Age of onset Family communication Let’s see why this stuff is important Assessment Questions Assessment Questions Rule out any medical causes for the dysfluency Also rule out co-morbidity Supporting information: Identifying specific linguistic errors for patterns Establishing baseline for future comparison Identifying strengths When It’s Both… (or More) Working with Deaf people who have SMI, you likely you will encounter people with both language deprivation and thought disorders Does it matter? Better language gives tools for better coping skills (aka, Aristotle was not all wrong!) If psychotic, medication will improve functioning but if language deprived, medication will not improve functioning Implications for forensics and treatment Questions? Contacts Office of Deaf Services Alabama Department of Mental Health PO Box 301410 Montgomery, AL 36130 www.mh.alabama.gov/MIDS www.mhit.org Steve Hamerdinger Charlene Crump Director, Deaf Services Voice/VP 334 239 3558 [email protected] Statewide MHI Coordinator VP 334 353 3558 [email protected]