Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
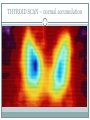
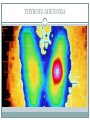
THYROID DYSFUNCTION DEGHAS LECTURE Thyroid Hormone Control TSH THS regulation- TRH , T3,T4 TSH synthesis of T3,T4 TSH thyroid gland growth FUNKCE ŠTÍTNÉ ŽLÁZY T3 RECEPTOR THYROID HORMONES Most of the T4 nda T3 in plasma bound to TBG Only free hormones are active ! The fT3 has 8 x higher activity than the fT4 20% of the T3 comes directly from the thyroid 80 % of the T3 se formed in tissues (esp. liver and kidney) from T4 by 5’-deiodase Identic amount of rT3 formed by 5-deiodase THYROID HORMONE FUNCTION Body growth ( gene expression GH) Maturation of CNS Adrenergic effect– β-1 receptor response to catecholamines basal metabolic rate ( cytochromes of the respiratory chain, cytochromoxidase and Na+-K+-ATPase) mobilize energy stores and catabolism (lipolysis, glycogenolysis, gluconeogenesis) GOITER TYPES OF GOITER ACCORDING TO FUNCTION: Euthyroid Hypothyroid Hyperthyroid ACCORDING TO STRUCTURE: Diffuse (colloid) Nodular HYPOTHYROIDISM-SYMPTOMS Fatigue, somnolence, muscle weakness, letargy, depression Bradypsychia, memory and concentration problems Bradycardia, decreased DBP Cold intolerance Constipation Body weight gain Diminished deep tendon reflexes Eybrow loss, dry skin, decreased sweating Pericardial and pleural effusions Forearm edema Hoarseness LABORATORY FINDINGS: PRIMARY HYPOTHYROIDISM: TSH, fT3,fT4 SECONDARY HYPOTHYROIDISM: TSH, fT3,fT4 TERTIARY HYPOTHYROIDISM: TRH, TSH, fT3,fT4 HYPOTHYROIDISM: cholesterol is typical 72-year old woman with hypothyroidism Cretenism HYPOTHYROIDISM-CAUSES PRIMARY HYPOTHYROIDISM (origin in the thyroid): Chronic lymphocytic thyroiditis – CLT (Hashimoto) Thyroidectomy Radiation therapy or nuclear catastrophy Lack or excess of iodine Drugs (methimazol, sunitinib, carbamazepin, amiodaron,) Infiltrative dieseases (e.g. Riedel’s goiter) HYPOTHYROIDISM SECONDARY HYPOTHYROIDISM – origin in the pituitary Craniopharyngioma, chromophobe adenoma, teratoma TERTIARY HYPOTHYROIDISM – origin in the hypothalamus Extremely rare CLT (HASHIMOTO) The most common cause of hypothyroidism ! Women 30-50 y! 9 x higher incidence in women than in men Positive PA/FA for autoim.dis., HLA-DR3, -DR4, -DR5, often vitiligo or alopecia Hepatitis C history Often as part of the “polyglandular syndrom” Autoimmun. inflam.-cellular and humoral resonse (cytotoxic T cells, auto-antibodies: anti TPO, anti TGB, anti TSH-R) CLT - DIAGNOSIS SYMPTOMS – initially unapparent (sometimes hyperthyroid ) Most of the cases dg. as advanced disease, when hypothyroidism is clinically present LAB TESTS: TSH, fT3,fT4 Anti TPO (95%), anti TGB (70%), anti TSH-R US: non-homogenic, hypoechogenic, often diminished thyroid FNAC: lymphocytic thyreoiditis, later fibrosis DIFF. DG. OTHER CAUSES OF HYPOTHYROIDISM Low T3/T4 syndrome fT3,fT4, rT3, clinically irrelevant no thyroxin supplementation needed CLT - THERAPY L-thyroxin replacement 25, 50, 75, 100, 150 μg tablets Avarage replacement dose 1.6 μg/kg/ PO daily Goal: TSH 0.5 – 2.0 mIU/l THYROIDECTOMY INDICATIONS for thyroidectomy: Graves’ disease Toxic adenoma, toxic multinodular goiter Thyroid carcinoma I131 THERAPY Graves’ disease Thyroid carcinoma EXTERNAL RADIATION ( > 25 Gy) Hodgkin’s lymphoma– neck lymphadenopythy Malginant tumors of the head and neck Nuclear catastrophy DRUGS Lithium Amiodarone Phenytoin Carbamazepine Ethonamide (anti-TBC) Overdose with thyreostatic drugs: Methimazole Propylthiouracil TPO inhibitors: sunitinib, sorafenib, imatinib INFILTRATIVE DISEASE (less common) Riedel’s fibrotic goiter Hemochromatosis Sclerodermia Leukemias Amyloidosis Riedel’s goiter Synonym: Riedel’s thyroiditis Extremely rare Etiology: unknown Slowly growing goiter-extremely solid consistency Painless Fibrotic inflammation w. lymphocytic infiltration Dif.dg.: tumor ! Possible destruction of the parathyroid glands Retrosternal expansion: stridor, dysphagia DIAGNOSIS OF HYPOTHYROIDISM TSH, fT3, fT4 Ultrasound Fine Needle Aspiration Cytology (FNAC) Antibody titre measurement (anti TPO, anti TGB, anti R-TSH) Scintigraphy (I131 accumulation) THYROID ULTRASOUND SEVERE HYPOTHYRODISM-MYXEDEMA EMERGENCY (result of prolonged and severe hypothyroidism) Triggered by: infection, trauma, surgery, cold Weakness, impaired conciousness to COMA Hypothermia Hypotension Hypoventilation Hypoglycemia Hyponatremia Edema, swollen tongue THERAPY OF MYXEDEMA INTENSIVE CARE UNIT Support of vital functions, ventilation support Glucocorticoids Glucose infusion Sodium supplementation L-thyroxin 100-200 μg IV initially Slow rewarming in hypothermia HYPERTHYROIDISM NEUROPSYCHIATRIC SYMPTOMS Restlessness Irritability Insomnia Anxiety Emotional lability Personality changes Psychosis Hyperactive deep tendon reflexes HYPERTHYROIDISM CARDIOVASCULAR SYMPTOMS cardiac output (tachycardia, periph. resistance) SBP, DBP Atrial fibrillation (in 20-30 %) Congestive heart failure Cardiomyopathy Mitral valve prolapse, mitral regurgitation HYPERTHYROIDISM GASTROINTESTINAL SYMPTOMS Increased peristaltics Malabsorption Hyperphagia in young patients Loss of appetite in older patients Vomiting Dysphagia due to enlarged goiter Liver enzyme elevation, esp. ALP, rarely steatosis HYPERTHYROIDISM METABOLIC SYMPTOMS Weight loss total cholesterol, HDL cholesterol Hyperglycemia (insulin action antagonism) cortisol HYPERTHYROIDISM MUSCLE SYMPTOMS Adynamia Muscle weakness (esp. thigh muscles) HYPERTHYROIDISM BONE SYMPTOMS Bone resorption Porosity of the cortical bone, thinner trabecular bone ALP, osteocalcin (higher bone turnover) Hypercalcemia leading to PTH suppression conversion of D2 to D3 Ca2+ resorption from the gut Ca2+ renal elimination OSTEOPOROSIS in chronic hyperthyroidism HYPERTHYROIDISM GENITOURINARY SYMPTOMS Polyuria, polydypsia SHBG MEN: total but free testosteron: gynecomastia, loss of libido, erectile dysfunction, impaired spermatogenesis WOMEN: total, but free estradiol: oligo-, amenorrhea, infertility HYPERTHYROIDISM LUNG SYMPTOMS Dyspnea O2 consumption, CO2 production Respiratory muscle weakness Trachea stenosis by enlarged goiter HYPERTHYROIDISM – SKIN SYMPTOMS Sweating Warm, moist, fine skin Fine hair Fine nails, onycholysis Hyperpigmentation Vitiligo Alopecia areata HYPERTHYROIDISM HEMATOLOGY SYMPTOMS erytrocyte volume (MEV) Normocytic normochromic anemia (due to increased plasma volume) ferritin autoimmune hematologic diseases (pernicious anemia, idiopatic trombocytopenic purpura=ITP) Risk of thrombosis (fibrinogen, v. Willebrand f., thrombocyte aggregation) HYPERTHYROIDISM-ETIOLOGY GRAVES' DISEASE (60-80 % of hyperthyroidism) Toxic multinodular goiter (15-20%) Thyroid adenoma (single thyroid nodule 3-5%) Subacute de Quervain thyroiditis Drugs: thyroxin excess (hyperthyreosis factitia), amiodarone, iodine (contrast agents) Second. hyperthyroidism (pituitary adenoma)-rare GRAVES’ DISEASE Autoimmune disease Genetic background-HLA-DQA1*0501 Viral infection as trigger ? Production of TSH-receptor antibodies = = TSI (thyroid stimulating antibodies) In GD sometimes initially hypothyroid period GRAVES' DISEASE DIAGNOSIS CLINICAL SYMPTOMS OF HYPERTHYROIDISM GRAVES' ORBITOPATHY LAB TESTS: TSH, fT3,fT4 TSI (> 95%) Anti TPO (70%) HYPERTHYROIDISM – GRAVES' ORBITOPATHY 25 % patients with Graves’ disease Correlation of orbitopathy with the severity of hypothyroidism Deposition of collagen and glycosaminoglycans in the muscles, enlargement of the retroorbital space Exophtalmos Upper eyelid retraction Von Greafe’s sign (lid lag on infraduction) Koch’s sign (bulbus lag on supraduction) Lagophtalmos GRAVES’ ORBITOPATHY GRAVES’ ORBITOPATHY GRAVES' DISEASE THERAPY Beta blockers Thyrostatic drugs-blocking MJT and DJT synthesis (methimazole, thiamazole, propylthiouracil) Radiactive iodine 131I (dos 200-2000 MBq)thyreostatics before and after the procedure recom. EUTHYROIDISM RESTORED AFTER SEV.MONTHS Subtotal thyroidectomy (after sev.months) if large goiter, thyreotoxic crisis) DIFF.DG. OTHER CAUSES OF HYPERTHYROIDISM Vegetative instability Psychosis High fever Cocaine, Amphetamine Tachycardia of different origin THYROTOXIC CRISIS Etiology: spontaneously in Graves disease autonomic adenomas (nodes) iodine agents thyroxin overdose inefficient thyrostatic therapy THYROTOXIC CRISIS STAGES Stage I: Tachycardia > 150, AF, Fever > 41°, sweating, psychomotoric agitation, diarrhea, vomiting, adynamia Stage II: + somnolence, psychotic symptoms Stage III: coma w/wo adrenal failure, shock THYROTOXIC CRISIS THERAPY EMERGENCY-INTENSIVE CARE UNIT Thiamazol 80 mg IV every 8 hours Beta-blockers Corticosteroids Fluid: 3-4 Liters IV/D Calorie intake: 3000 kcal/D Lowering body temperature (ice) Sedation Thromboembolic prophylaxis THYREOTOXIC CRISIS THERAPY IN SEVERE CASES (e.g. iodine induced): PLASMAPHERESIS SUBTOTAL THYROIDECTOMY SUBACUTE de QUERVAIN'S THYROIDITIS Rare cause of hyperthyroidism Incidence 5 x higher in women than men Etiology: probably viral infection, often after respiratory infection Clinical signs: hyperthyroidic-euthyr-hypothyroidic, painful thyroid, Lab tests: ESR, CRP, normal leukocytes Therapy: mostly spontaneous healing, NSA, rednisolon are optional MULTINODULAR GOITER AUTONOMOUS ADEMOMA DIAGNOSIS: 131I accumulation on thyroid scan, US CLINICAL SYMPTOMS of hyperthyroidism THERAPY: thyreostatics, radioactive iodine MULTINODULAR GOITER ULTRASOUND OF A THYROID NODULE THYROID SCAN – normal accumulation THYROID ADENOMA