Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
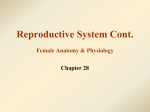
Functions of the Female Reproductive System Produce hormones (estrogen and progesterone) for secondary sexual characteristics. Produce one large oocyte at regular intervals and release it in such a way that it enters the oviduct (“Fallopian tube”,“uterine tube”). Receive semen from the male and transport it into the oviduct. Produce hormones (estrogen and progesterone) which prepare the uterus for pregnancy each cycle by thickening its inner lining; Getting rid of this thickened lining each cycle if pregnancy does not occur. Protect and nourish the embryo and fetus during pregnancy, then expel it through the vagina Produce milk to nourish the newborn Organs of the female reproductive system Let’s start with the Ovary: Located within pelvis, 2 to 5 cm (1 to 2 inches) lateral to the uterus Approximately 3cm x 2cm x 1cm Central region, or “medulla”, consists of connective tissue with many blood vessels. Outer region, or “cortex”, has all of the follicles within which oocytes develop and are ovulated. Maturation of an oocyte is called oogenesis, which leads to ovulation (release of the oocyte from the ovary) During oogenesis, the oocyte is surrounded by one or more layers of follicular cells (also called granulosa cells) forming a follicle The developing oocyte and its follicle: Four stages before ovulation 1. Primordial Follicles: All formed before birth - hundreds in each ovary Have not yet begun development – remain dormant until puberty Consists of primary oocyte surrounded by a single layer of flat follicular cells The developing oocyte and its follicle: Four stages before ovulation 2. Primary Follicles: Develop only after puberty; 3 to 4 enter this stage each cycle No change in primary oocyte Follicle has begun development – cells are larger The developing oocyte and its follicle: Four stages before ovulation 3. Secondary Follicles: 1 or 2 primary follicles progress to this stage each cycle Primary oocyte larger, finishes first division of meiosis to become a secondary oocyte, also forming a polar body. Follicle grows larger as follicular cells divide to form many layers; spaces begin to develop in center of follicle The developing oocyte and its follicle: Four stages before ovulation 4. Mature or Vesicular Follicle Most follicles which made it to “secondary” will reach this stage Follicle is very large; Many layers of cells surrounding fluid-filled center called antrum Secondary oocyte covered with thick, clear membrane called zona pellucida; pushed to one side in follicle and surrounded by mass of follicular cells called cumulus oophorus Big Question: How is this process of oogenesis regulated? Oogenesis and growth of the follicle are regulated by the pituitary gland, which lies just below the brain The next stages, ovulation and formation of a corpus luteum, will also be controlled by the pituitary gland. Oogenesis and growth of the follicle in the ovary are stimulated by follicle stimulating hormone (FSH) from the pituitary During oogenesis under the stimulation of FSH, follicular cells surrounding the oocyte secrete the hormone estrogen, which stimulates the inner lining of the uterus to thicken and begin secreting mucus, getting ready for pregnancy This estrogen from the follicular cells also inhibits the pituitary gland from secreting any more FSH. Thus, no more follicles will be stimulated to develop until it stops. Rupture of the follicle is ovulation. The secondary oocyte, surrounded by the zona pellucida and cumulus oophorus, is released from the surface of the ovary, where it can be captured by the open end of the oviduct. The cumulus oophorus now called the corona radiata. Ovulation is triggered when the pituitary gland increases its secretion of a different hormone, called luteinizing hormone. Luteinizing hormone also causes the follicular cells of the now empty follicle to develop into a corpus luteum. This structure secretes the hormone progesterone, which inhibits the secretion of luteinizing hormone from the pituitary gland Before ovulation: Cells of follicle secrete estrogen, which stimulates the lining of the uterus to develop. After ovulation: Cells of the corpus luteum secrete progesterone, which maintains the uterine lining in this “ready for pregnancy” condition If fertilization and pregnancy do not occur, after a few days the corpus luteum deteriorates and stops producing progesterone. Without its stimulus, the uterus can not maintain its thick lining, so this falls off and is shed as menstruation. If fertilization and pregnancy occur, the placenta of the embryo secretes a hormone called chorionic gonadotropin, which stimulates the corpus luteum to keep secreting progesterone, which in turn keeps the lining of the uterus thick and full of blood vessels. When the oocyte is released from the surface of the ovary during ovulation, it is picked up by the oviduct, or Fallopian Tube, a hollow muscular tube which leads from near the uterus to the ovaries. Oviduct or Fallopian Tube: Lateral End: Wide opening, or infundibulum, surrounds the surface of the ovary. The edge is surrounded by finger-like fimbria. Middle Part: Wide ampulla Medial End: Narrow isthmus leads into uterus. Cavity of oviduct is continuous with cavity of uterus By mechanisms not completely understood: The oviduct moves the oocyte toward the uterus The oviduct moves sperm away from the uterus Fertilization occurs in ampulla of oviduct, forming the zygote, which goes through repeated mitotic cell divisions to eventually form the embryo. Oviduct moves this growing mass of pre-embryo cells toward uterus: takes 3 or 4 days. Secretions from oviduct are necessary to keep sperm, oocyte, and embryo alive. Uterus: Anterior to rectum; Posterior & superior to bladder Narrowed inferiorly to form cervix, which projects into vagina Uterus: Outer layer = Myometrium: Thick layer of muscle Inner layer = Endometrium: Lots of glands & blood vessels Two layers of endometrium: Basal layer: Closer to myometrium; Remains after menstruation; Regrows functional layer Functional layer: Closer to cavity; Thickens every cycle when stimulated by estrogens; Embryo implants here during pregnancy; Dies and falls off during menstruation Mass of Uterus: Immediately before menstruation: 100 – 150 grams Immediately after end of menstruation: 50 – 100 grams At end of pregnancy: 1,000 – 1,500 grams Uterus extends from vagina inferiorly to bottom of sternum superiorly Lies anterior to all other abdominal organs except bladder Vagina: Thin-walled, tubular Inferior to uterus; Anterior to rectum Posterior to bladder & urethra Receives penis and semen during sexual intercourse Passage for delivery of fetus or menstrual flow External Genitalia: The vagina opens between the inner labia or labia minora, into a space called the vestibule. Outside of those are the outer labia or labia majora. At the anterior junction of the outer labia is the clitoris … Note that the urethra also opens into the vestibule, but the anus opens posterior to it. The head, or glans, of the clitoris which is visible is only a small part of this organ. Two shafts of erectile tissue extend backwards along the pelvic floor on either side of the urethra and vagina. These are the same erectile tissues located in the penis of a male, called corpora cavernosa Oviduct Ovary Lateral to uterus Uterus Bladder Pubic Bone Clitoris Labium minora Vagina Urethra Labium majora x