Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Herpes simplex virus wikipedia , lookup
Schistosoma mansoni wikipedia , lookup
Toxocariasis wikipedia , lookup
Chagas disease wikipedia , lookup
Toxoplasmosis wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Herpes simplex wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
African trypanosomiasis wikipedia , lookup
West Nile fever wikipedia , lookup
Marburg virus disease wikipedia , lookup
Hookworm infection wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Leptospirosis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Trichinosis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Hepatitis C wikipedia , lookup
Onchocerciasis wikipedia , lookup
Sarcocystis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Hepatitis B wikipedia , lookup
Fasciolosis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Neonatal infection wikipedia , lookup
Leishmaniasis wikipedia , lookup
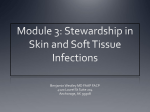
Musculoskeletal system infection Infection of skin ( Cellulitis, Subcutaneous layer infection). Infection of skeletal muscles ( Infectious Myositis). ( Infectious Pyomyositis). Infection of Tendon (Tendonitis, Infectious Tenosynovitis). Infection of Bursa (Bursitis) Septic arthritis. Infection of bone (osteomyelitis). Infection of skin Infection of skin: Cellulitis and subcutaneous layer infection: Cellulitis is a diffuse inflammation of connective tissue with severe inflammation of dermal and subcutaneous layers of the skin. Cellulitis can be caused by normal skin flora or by exogenous bacteria. It often occurs where the skin has previously been broken: cracks in the skin, cuts, burns, insect bites, surgical wounds, intravenous drug injection or sites of intravenous catheter insertion. Cellulitis Bacterial causes of cellulitis: Group A Streptococcus and Staphylococcus are the most common cause of cellulitis. Predisposing conditions for cellulitis include: Insect or spider bite, animal bite, tattoos, itchy skin rash, recent surgery, athlete's foot, dry skin, eczema, and drugs injections. Signs and symptoms: Erythema, edema, with necrosis and inflamed margins. Pus formation mainly associated with the pyogenic infection. Cellulitis The reddened skin or rash may considered as a signal of deeper, more serious infection of the inner layers of skin. Once below the skin, the bacteria can spread rapidly, entering the lymph nodes and the blood stream and spreading throughout the body. This can result in influenza- like symptoms with a high temperature and sweating or feeling very cold. Cellulitis Bacterial infection of dermis could extend to hypodermis(the subcutaneous layer of skin) causing: - Hair follicle root infection (folliculitis) - Sweat gland infection - Bursae infection (Bursitis) -Fibrous bands infection Leading to deep fascia infection and necrotizing fasciitis. Folliculitis could extend in the hypodermis layer to form: Furuncles: large, painful, raised nodules with an underlying collection of dead and necrotic tissue. Carbuncles result from the untreated furuncles. Multiple sinus tracts are usually present. Chills and fevers are associated with carbuncles and indicate systemic spread of the pathogenic bacteria. Bacteremia with secondary spread to other tissues is common with carbuncles. Bursitis Bursitis: The most common pathogen is Staphylococcus aureus. Ultrasonography (US) will not differentiate an infected bursa and post-traumatic bursitis. So, accumulated fluid should be collected for laboratory investigations. Erythema, edema and inflammation of Bursae Infectious Tenosynovitis and Tendonitis Infectious Tenosynovitis and Tendonitis: Tenosynovitis is the inflammation of the fluid-filled sheath ( the synovium) that surrounds a tendon. Symptoms of tenosynovitis include pain, swelling and difficulty moving the particular joint where the inflammation occurs. Acute tenosynovitis is caused predominantly by Staphylococcus aureus or Streptococcus pyogenes and most frequently involves the tendon sheaths of the flexor muscles . It is usually the result of a penetrating injury ( animal bite, puncture wound) and may be complicated by the presence of foreign bodies. Pus accumulated within the tendon sheath should be extracted for microbiology laboratory tests (by US help). Tenosynovitis and Tendonitis Necrotizing Fasciitis Necrotizing fasciitis (NF): Commonly known as flesh-eating disease is a rare infection of the deeper layers of skin and subcutaneous tissues, easily spreading across the fascial plane within the subcutaneous tissue. Type I describes a polymicrobial infection, whereas Type II describes a monomicrobial infection. Many types of bacteria can cause necrotizing fasciitis : Group A Streptococcus (Streptococcus pyogenes), Staphylococcus aureus, Vibrio vulnificus, Clostridium perfringens, and Bacteroides fragilis. Necrotizing fasciitis Group A Streptococcus made up most cases of Type II infections. However, since as early as 2001, another serious form of monomicrobial necrotizing fasciitis has been observed with increasing frequency. In these cases, the bacterium causing it is methicillinresistant Staphylococcus aureus (MRSA). The infection begins locally at a site of trauma, which may be severe (such as the result of surgery), or minor. Over 70% of cases are recorded in patients with one of the following clinical situations: immunosuppression, diabetes, alcoholism/drug abuse, malignancies, and chronic systemic diseases. Bacterial cellulitis & Necrotizing fasciitis Staphylococcal cellulitis Caucasian male with necrotizing fasciitis. The left leg shows extensive redness and necrosis. Necrotizing Fasciitis Pathophysiology: "Flesh-eating bacteria" cause the destruction of skin and muscle by releasing toxins (virulence factors), which include Streptococcal pyogenic exotoxins. Streptococcus pyogenes produces an exotoxin known as a superantigen. This toxin is capable of activating T-cells non-specifically, which causes the overproduction of cytokines and severe systemic illness (Toxic shock syndrome). Streptococcus pyogenes cellulitis Necrotizing Fasciitis The Streptococcus Cellulitis Streptococcus pyogenes infection: Erythema, edema, and pus formation. Bacterial cellulitis & Necrotizing fasciitis Laboratory diagnosis: Clinical specimen: Pus exudate, wound swab. Culture: Clinical specimens should be cultivated on blood agar, chocolate agar, and lactose differential medium by four quadrant streaking method. Identification of Staphylococcus aureus : Gram+ve Cocci in clusters. Bacterial cellulitis & Necrotizing fasciitis Identification of Streptococcus pyogenes Gram +ve Cocci arranged in chains or in pairs. Beta Hemolytic due to its phospholipase C activity. Bacitracin sensitive. Subcutaneous Mycosis Subcutaneous Mycosis: SPOROTRICHOSIS: Chronic infection involving cutaneous, subcutaneous and lymphatic tissue. Frequently encountered in gardeners. May develop in otherwise healthy individuals. Most common in Mexico, endemic in Brazil, Uruguay, South Africa. Etiology: Sporothrix schenkii, thermally dimorphic fungus naturally present in soil. At 37°C: Round/cigar-shaped yeast cells, at 25°C: Septate hyphae, rosettelike clusters of conidia at the tips of the conidiophores. SPOROTRICHOSIS SPOROTRICHOSIS: Pathogenesis and Clinical findings: Skin: lesions usually follows minor trauma, appear in the form of nodules that ulcerate ulcer necrosis. Skin/subcutaneous tissue lymphatic vessels lymph nodes Systemic dissemination: Skeletal muscles, bones, joints. Diagnosis: Samples: aspiration fluid, pus, biopsy Microscopy: direct microscopic examination (KOH) and histopathological examination (methenamine silver stain) reveal yeast cells and asteroid body. Culture: on Sabouraud dextrose agar for 4-6 weeks at 25°C (Moulds). At 37°C (yeast) Serology: Yeast agglutination test, sporotrichin skin test. CHROMOBLASTOMYCOSIS CHROMOBLASTOMYCOSIS: Post-traumatic chronic infection of subcutaneous tissue. Papules verrucous flower-like lesions on lower extremities. Necrosis and subcutaneous inflammation. Etiology: Fonsecaea and Phialophor species. Pigmented (dematiaceous) fungi in soil. Diagnosis: Direct microscopic examination of lesion scrapings (KOH): sclerotic body. Skin scrapings from a patient showing characteristic brown pigmented, planate-dividing, rounded sclerotic bodies. MYCETOMA MYCETOMA: Post-traumatic chronic infection of subcutaneous tissue Common in tropical climates. Etiology: Saprophytic fungi (Eumycetoma) and Actinomyces (Actinomycetoma): Madurella mycetomatis, and Exophiala jeanselmei. Clinical findings: Site: feet, lower extremities, hands Findings: abscess formation, draining sinuses containing granules and deformities. Dissemination: muscles and bones. Treatment: Eumycetoma: surgery and antifungal therapy (Potassium iodide (Topical/oral), And Amphotericin B. Actinomycetoma: antibiotic combinations Chromoblastomycosis & Mycetoma Chromomycosis of the foot caused by Fonsecaea pedrosoi Mycetoma of foot: Madurella mycetomatis Protozoan infection of skin Protozoan infection of skin: Leishmania genera: The Blood and Tissue Mastigophora. 1- L. donovani: The causative organism of Visceral leishmaniasis (Kala-azar) 2- L. tropica: The causative organism of Cutaneous leishmaniasis of old world (Oriental sore) 3- L. mexicana: The causative organism of Cutaneous leishmaniasis of new world (Chiclero ulcer) 4-L. braziliense: The causative organism of Mucocutaneous leishmaniasis of new world. LEISHMANIA DONOVANI LEISHMANIA DONOVANI: (Visceral leishmaniasis, Kala-azar, Dum-Dum fever) Distribution: India, (1. d donovani), Mediterranean Coast, China (L d infantum), Central Africa (1. d. archibaldi), South America (1. d chagasi). Habitat: Reticuloendothelial system (blood, spleen, liver, bone marrow, lymph node, skin). Morphology: Leishmania exist in two forms: 1-Leishmania form (amastigote): in tissues of man. 2- Leptomonad form (promasigote): in the gut of vector LB. (Sand fly) or in culture. D.H.: Man, Dog and Rodents (Dog and Rodents act as a reservoir host in certain areas as Mediterranean Coast, Central Africa and South America). LEISHMANIA DONOVANI Vector: Female sand fly of the genus Phlebotomus. Life cycle in vector: (Cyc1opropagative transmission): When the sand fly takes an infected meal, the amastigotes go to mid gut where they multiply and by the end of the 2nd day, it will be converted into promastigotes which elongate, Multiply and increase in number forming rosettes filling the lumen of the mid gut (fifth day). Promastigotes return back to pharynx, buccal cavity and proboscis, now they are ready to infect another person, where they change into amastigotes (promastigotes do not invade salivary gland of the vector). LEISHMANIA DONOVANI Life cycle of Leishmania: LEISHMANIA DONOVANI Pathogenesis: - The promastigote engulfed by skin macrophages, converted into the amastigote stage. - The skin macrophage carry the microbe to viscera via blood stream, where it infects the R.E.S. - Skin, liver, spleen, bone marrow, kidney, and lymph nodes will be colonized by infected macrophage. LEISHMANIA DONOVANI Clinical picture: -Onset: usually gradual with high or low grade fever. -Toxaemia, anorexia, loss of weight. -Splenomegaly, Hepatomegaly, jaundice, disturbed liver function, ↑globulin and ↓ albumin, reversed A/G ratio. -Anaemia, leucopaenia with monocytosis. - Lymphadenopathy. -Glomerulonephritis and dysentery with leishmania bodies in urine and stool. -Nasal and pharyngeal granulomata LEISHMANIA DONOVANI