Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
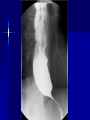
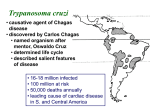
Achalasia/Chagas Disease Kunwar Sohal, PGY 3 April 20, 2010 Achalasia Greek term that means "does not relax" Loss of peristalsis in the distal esophagus (whose musculature is comprised predominantly of smooth muscle) and a failure of LES relaxation Histologic examination reveals decreased numbers of neurons (ganglion cells) in the myenteric plexuses Degeneration preferentially involves the nitric oxide-producing, inhibitory neurons that effect the relaxation of esophageal smooth muscle; the cholinergic neurons that contribute to LES tone by causing smooth muscle contraction are relatively spared Etiology Etiology of primary achalasia is not known, however certain recognized diseases can cause esophageal motor abnormalities similar or identical to those of primary achalasia – Chagas Disease – Malignancy: most common cause of pseudoachalasia in most populations, through invasion of plexus or as paraneoplastic syndrome – Achalasia like motor abnormalities: amyloidosis, sarcoidosis, neurofibromatosis Diagnosis A barium swallow is the primary screening test when achalasia is suspected on clinical grounds Diagnostic accuracy of barium swallow for achalasia is approximately 95 percent Manometry: required for confirmation in virtually all cases – Elevated resting LES pressure, above 45mm Hg – Incomplete/absent LES relaxation: in response to a swallow – Aperistalsis of the smooth muscle portion of the body of the esophagus Treatment Nitrates and CCBs Botulinum toxin injection: poisons the excitatory (acetylcholine-releasing) neurons that increase LES smooth muscle tone – Initial success rates of close to 80 percent are similar to those seen with endoscopic balloon dilation and surgery – Symptom relief wanes with time (70 percent at 3 months, 53 percent at 6 months, and 41 percent at 12 months Dilation of LES: for poor surgical candidates Surgical Myotomy Heller Myotomy and Toupet fundoplication Myotomy: cut muscles Toupet (posterior) fundoplication, the fundus is wrapped around the back of the esophagus Chagas’ Disease Caused by the protozoan parasite, Trypanosoma cruzi Humans can become infected with resulting acute or chronic disease Found only in Central and South America, Mexico and the southern United States WHO has estimated that 16 to 18 million people are infected with T. cruzi, with an estimated annual infection rate of 300,000 and an annual mortality rate of >50,000 patients Prevalence estimates are largely based upon results of testing in blood banks. Between 1960 and 1989, the prevalence of infected blood in selected cities of South America ranged from 1.7 percent in Sao Paulo, Brazil, to 53 percent in Santa Cruz, Bolivia 70 to 90 percent of infected individuals are asymptomatic carriers of T. cruzi and never develop any symptoms Chagas’, contd Vector for this infection is the reduviid bug, also known as the "kissing bug" Once a bug is infected, it remains so for life and can transmit infection for several years Chronic Chagas’ Disease Pathogenesis of chronic Chagas' disease is unclear Extensive debate over whether the complications that arise are due directly to parasite invasion or to secondary autoimmune mechanisms Approximately 50 percent of infected individuals develop cardiac and/or digestive forms of the diseasetypically demonstrate cardiomegaly, megaesophagus, and megacolon Dilationmore R sided, signs of systemic congestion (ascites, hepatomegaly) predominate over pulm edema The most characteristic cardiac anatomic lesion is the ventricular apical aneurysm which, in one series, was noted in 52 percent of 1078 autopsied chagasic patients Histologic examination shows chronic mild myocarditis Acute Most patients are asymptomatic during the acute stage of infection In a minority, acute infection may be associated with a persistent local reaction, or either Chagoma (swelling and local lymphadenopathy) or for bites involving the orbit Microscopic examination shows intense parasitism in virtually every organic system, with prominent inflammatory changes in the vicinity of ruptured infected cells Diagnosis Diagnosis is generally made by testing with at least two different serologic tests CDC recommends ELISA and IFA (immunofluorescence assay) Treatment If confirmatory testing is positive The treatment is indicated for patients with the acute form of the disease or in congenital disease, no good studies in chronic Recommendations do suggest that adults aged 1950 yrs without advanced Chagas cardiomyopathy, that antitrypanosomal drug treatment should generally be offerred (Bern et al, JAMA 2007) Nifurimox is typically their first line treatment (easier to release by CDC under current protocols), for 90 days