Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Spinal cord:
ascending & descending pathways
2012/3/26
Josh Wu
Spinal cord
• White matter (pathways)
abundant in upper cord
contain sensory & motor pathways
serving all 4 limbs
o cuneate fasciculus (CF)
carries information from UE
only in C segments
ogracile fasciculus (GF)
carry information from LE
present in both C & L levels
• Gray matter (neuron cell body)
cervical & lumbosacral enlargements
innervation of limbs
Types of spinal neuron
• In thick sections of spinal cord
nerve cells exhibit a laminar
(layered) arrangement.
• True lamination is confined to post.
horn
• 10 laminae of Rexed
defined in gray matter
correlate findings from animal
research in different labs
Types of spinal neuron
• Smallest neurons
soma diameters 5-20μm
propriospinal
entirely contained within cord
Some are confined within a single segment; others span 2 or more segments
by way of neighboring propriospinal tract
Functions
1. participate spinal reflexes
2. intermediate cell stations
motor projection: interposed between fiber tracts descending
from brain to locomotor apparatus ()
sensory transmission ( to CNS)
Types of spinal neuron
• Medium-sized neurons
soma diameters 20-50μm
in all parts of gray matter except substantia gelatinosa
Function
relay (projection) cells: receiving inputs from post root afferents
and projecting to brain ()
forming tracts (a functionally homogeneous group of fibers)
• Largest neurons
soma 50-100μm
alpha motor neurons (αMN): supply skeletal muscles
gamma motor neurons (γMN) (smaller): supply muscle spindles
Renshaw cells (med part of ant horn): tonic inhibition on αMN
Other structures
• individual ganglion surround with modified
Schwann cells called satellite cells
• stem axon: bifurcates
• ganglion cells enter post. n. roots
Exception: visceral afferents enter cord by ventral
roots failure post. rhizotomy (surgical section
of post roots) to relieve pain for intra-abdominal
cancer
Spinal ganglia
• located in intervertebral foramina
ant. + post. roots = spinal n.
thoracic ganglia: 50,000 unipolar neurons
ganglia serving limbs: 100,000 cells
• cord shows no evidence of segmentation
internally
• Reality: nuclear groups in cell columns
spanning several segments
Central terminations of post root afferents
• medial stream
medium + large fibers
divide within post funiculus for
ascending/descending branches swing
into post gray horn synapse in laminae
II, III, & IV
largest ascending fibers run all way to post
column nuclei (gracilis-cuneatus) in
medulla oblongata
these long fibers form bulk of FG & FC
• lateral stream
small (Aδ + C) fibers
divide into short ascending/descending
branches within posterolateral tract of
Lissauer
synapse on neurons in lamina I (marginal
zone), lamina II (substantia gelatinosa), and
some dendrite to laminae III-V
ASCENDING SENSORY PATHWAYS
• Conscious sensations
(perceived at cerebral cortex)
1. Exteroceptive sensations
From external world
somatic receptors on body surface or telereceptors serving vision/hearing
include touch, pressure, heat, cold, and pain.
2. Proprioceptive sensations
arise within body
locomotor system (muscles, joints, bones) and vestibular labyrinth
pathways to cerebral cortex for position (stationary) & kinesthetic
(movement) sense
• Non-conscious sensations (refer to cerebellum)
1. Non-conscious proprioception
to cerebellum through spinocerebellar pathways
essential for smooth motor coordination
2. Interoception (Enteroception)
unconscious afferent signals involved in visceral reflexes
Sensory testing
• Routine assessment of somatic exteroceptive sensation includes:
1. Touch: by finger tip or a cotton swab
2. Pain: by applying point of a pin
3. Thermal sense: by warm or cold test tubes
In alert & cooperative patients, active & passive tests of conscious
proprioception can be performed
• Active proprioception tests: execute activities with eyes closed
1. toe the line without swaying
2. finger-to-nose test
3. heel-to-knee test
• Passive proprioception tests:
1. Joint sense (mainly by passive stretching of neuromuscular spindles)
clinician grasps thumb or great toe by sides and moves it while asking patient
to name direction of movement ('up' or 'down')
2. Vibration sense.
vibrations of a tuning fork applied to radial styloid process or to shaft of tibia
Question 1
heel-to-knee test
1
2
3
4
Question 2
1
2
3
4
Question 3
1
2
3
4
Ascending Pathways
Somatic Sensory Perception
posterior column-medial lemniscal
pathway (PCML)
spinothalamic pathway
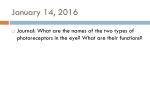
SOMATIC SENSORY PATHWAYS
Common features:
• Both comprise 1st, 2nd, 3rd-order sets of
sensory neurons
• 1st-order somas (primary afferents) occupy
post. root ganglia
• 2nd-order somas occupy CNS gray matter on
same side as 1st-order neurons
• 2nd-order axons cross midline and then
terminate in thalamus
• 3rd-order neurons project: thalamus somatic
sensory cortex
• Both pathways are somatotopic: orderly map
of body parts can be identified in gray matter
• Synaptic transmission from 1 2 & 23
neuron can be modulated (inhibited or
enhanced) by other neurons
3rd
1st
2nd
spinothalamic pathway
Posterior Column-Medial Lemniscal pathway
• 1st-order afferents include largest somas in post.
root ganglia
receive info from largest sensory receptors:
1.Meissner's and Pacinian corpuscles
2.Ruffini endings
3.Merkel cell-neurite complexes
4.neuromuscular spindles
5.Golgi tendon organs
LE: FG (fasciculus gracilis)
UE: FC (fasciculus cuneatus)
• 2nd-order afferent
LE: FG NG (nucleus gracilis)
UE: FC NC (nucleus cuneatus)
• Crossed midline in great sensory decussation of
medulla oblongata medial lemniscus pons
& midbrain terminates in VPL (ventral
posterolateral nucleus) of thalamus
• trigeminal lemniscus
terminating in VPM (ventral posteromedial
nucleus)
• 3rd -order afferents
thalamus somatic sensory cortex
Function of PCML pathway
• Chief functions
conscious proprioception + discriminative touch provide parietal lobe with an
instantaneous body images both at rest & during movement
Without background information impair execution of movements
• Clinical correlation
disturb PCML in demyelinating diseases, e.g. multiple sclerosis
sensory ataxia: movement disorder resulting from sensory
impairment
P’t can stand unsupported only with feet well apart and with gaze
directed downward
broad-based gait, Max stamping action for remains conscious
proprioceptive function
severe swaying as patient stands feet together with eyes closed
tandem Romberg's sign: Inability to 'toe the line' with eyes closed
loss kinesthetic sense: finger-to-nose and/or heel-to-knee tests
two-point discrimination test impair of tactile discrimination
joint sense and vibration sense may also be impaired
Tactile, painful, and thermal sensations are preserved
Ascending Pathways
• Uncrossed
• Proprioception
• Touch (2 point
discrimination)
Spinothalamic pathway
2nd-order sensory neurons
• projecting from laminae I-II, IV-V of post
gray horn to contralateral thalamus
• receive excitatory & inhibitory synapses from
neurons of substantia gelatinosa 'gating'
(modulatory) effects on sensory transmission
• cross midline in ant. commissure at all
segmental levels
• anterolateral pathway is divisible into
ASTT (anterior spinothalamic tract) ant.
funiculus
LSTT (lateral spinothalamic tract) lat.
funiculus
merge in brainstem as spinal lemniscus
joined by trigeminal afferents
VP (ventral post) nucleus of thalamus
3rd-order sensory neurons
• project from thalamus to somatic sensory
cortex
Functions of Spinothalamic pathway
• modality segregation: postoperative sensory testing
ASTT touch
LSTT thermal & noxious sensations
• Both LSTT & ASTT are somatotopically arranged
front back
neck leg
Percutaneous cordotomy
• interrupt spinothalamic pathway on one or both sides for
relief of intractable pain
1. passed needle between atlas/axis into subarachnoid
space
2. advanced into anterolateral region of cord under
radiologic guidance
3. pass mild current elicit paresthesia (tingling) on
opposite side of body destroy anterolateral pathway
• P’t is insensitive to pinprick, heat, or cold on opposite side
• touch sensitivity
• performed for terminal cancer patients not benign
wears off after about a year
Ascending Pathways
thermal
noxious
crossed
Touch
Spinocerebellar pathways
• 4 fiber tracts run from spinal cord to cerebellum
1. PSCT (posterior spinocerebellar)
non-conscious proprioception
2. cuneocerebellar
report continuously state of internuncial
3. ASCT (anterior spinocerebellar)
neurons in spinal cord
4. RSCT (rostral spinocerebellar)
Non-conscious proprioception
(1)
• both uncross control by each cerebellar
(2)
hemisphere
(3)
PSCT (post. spinocerebellar tract)
(4)
from LE primary afferents enter FG
nucleus dorsalis originates in post thoracic
nucleus in lamina VII at base of post gray
horn nucleus extends T1-L1 segmental
levels
very fast conduction
largest fibers in CNS (ext diameter: 20μm)
receives primary afferents from m. & joints
also receives collaterals from cutaneous
sensory neurons
tract ascends close to surface of cord &
enters inferior cerebellar peduncle
cuneocerebellar tract from accessory NC
UE & upper trunk through FC
enters inferior cerebellar peduncle
Stretch reflex
Ia internuncial serving reciprocal inhibition
non-conscious proprioception
kinesthesia
Information from reflex arcs
• 2 tracts originate in intermediate gray matter
of cord
• their main function is to monitor activity
state of spinal reflex arcs
ASCT
• lower half of cord
component fibers cross initially run close
to surface midbrain superior cerebellar
peduncle & recross within cerebellar white
matter
RSCT
• upper half of cord
ascends without crossing & enters inferior
cerebellar peduncle
SRT (Spinoreticular tracts)
•
•
•
•
oldest somatosensory pathways
half of SR fibers may be uncrossed
without somatotopically arranged
SR fibers originate in laminae V-VII
accompany spinothalamic pathway
brainstem
• 2 interrelated functions
1. induce cerebral cortex waking state
2. report to limbic cortex of ant cingulate gyrus
about nature sti pleasurable or aversive
• phylogenetically old 'paleospinothalamic'
pathways reticular formation emotional
somatic sensory sti.
ant.
SRT
post.
OTHER ASCENDING PATHWAYS
• ST (spinotectal tract):
runs alongside spinothalamic pathway
resembles in its origin & functional composition
ends in superior colliculus (joins crossed visual inputs)
involved in visuospinal reflex
• SOT (spinoolivary tract):
sends tactile information to inf. olivary nucleus in
medulla oblongata
important function in motor learning
modify cerebellar activity in response to
environmental change
motor adaptation
• spinocervical tract
well developed in cat (small spinothalamic pathways)
vestigial or absent in humans
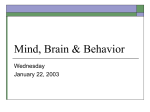
Summary of Ascending Pathways
PCML (motor)
Spinocerebellar
emotional
Spinothalamic
(Pain, Touch)
Question 4 (2 point)
• pathway for this
functional performance
1. PSCT
2. RSCT
3. Spinothalamic
4. PCML
Question 5 (2 point)
• Location of the soma for this 2nd-order afferent
1. Left nucleus gracilis
2. Right nucleus gracilis
3. Left nucleus cuneatus
Move “up” & “down”
4. Right nucleus cuneatus
16 Spinal cord: descending
pathways
Cell types
α-motor neurons (αMN)
large, supply extrafusal fibers of skeletal m.
Tonic & phasic αMN
• Tonic αMN
innervate slow, oxidative-glycolytic m. fibers
depolarized & slowly conducting axons with small spike amplitudes
• Phasic αMN
innervate squads of fast, oxidative & fast, oxidative-glycolytic m. fibers
larger, higher thresholds, rapidly conducting axons with large spike amplitudes
from propriospinal sources
usually 1st recruits when voluntary movements are initiated
γ -motor neurons (γ MN)
small, supply intrafusal fibers of neuromuscular spindles
Renshaw cells
• in med. part of ant. horn
• form inhibitory, glycinergic synapses on αMN
• negative feedback, or recurrent inhibition
Cell columns
• Each motor neurons columns supplies a group of m. having similar functions
• individual m. are supplied from cell groups (nuclei) within columns
6 somatomotor cell columns
(C3-5), Diaphragm
lat. limb m.
(C5-8, L2-S2),
Arm, thigh
(C6-8, L3-S3),
Forearm, leg
(C8, T1, S1-2)
intrinsic m.
med. trunk m.
(T1-L2), Intercostals,
abdominals
(all segments), Erector spinae
DESCENDING MOTOR PATHWAYS
• Important pathways descending to spinal cord are
1. corticospinal (pyramidal) (CST)
2. reticulospinal (extrapyramidal) (RST)
3. vestibulospinal
4. tectospinal
5. raphespinal
6. aminergic
7. Autonomic
c
c
c
Corticospinal tract (CST)
• Main voluntary motor pathway
• sources
1. about 50% from primary motor
cortex in precentral gyrus
2. supplementary motor area on
med. side of hemisphere
3. premotor cortex on lat. side
4. somatic sensory cortex
5. parietal lobe
6. cingulate gyrus
(contributions from 2 sensory areas
mentioned terminate in sensory nuclei of
brainstem & spinal cord modulate
sensory transmission)
Corticospinal tract
• CST pathway
corona radiata & internal capsule
brainstem crus of midbrain &
basilar pons medulla oblongata
forms pyramid
• Corticonuclear: gives off fibers to
activate motor cranial nerve nuclei
for face, jaw, and tongue m.
Corticospinal tract (CST)
Just above spinomedullary junction
1.About 80% of fibers cross midline in
pyramidal decussation
2.descend on contralateral side of spinal
cord as LCST (lat corticospinal tract)
3.About 10% enter ACST (ant
corticospinal tract) occupies ant
funiculus at cervical & upper thoracic
levels cross in white commissure
& supply MN for deep m. in neck
4.About 10% of pyramidal fibers enter
LCST on same side
• CST contains about 1 million nerve
fibers
• All corticospinal fibers are excitatory
& use glutamate as transmitter
Targets of LCST
Distal limb motor neurons
• A unique property of corticomotoneuronal fibers of LCST is fractionation
selectively activate small groups of neurons
• most obvious in index finger flex/ext quite independently
• essential for skilled movements (buttoning a coat or tying shoe laces)
• when lost, seldom recover completely
• α & γ MN are coactivated by LCST during a given movement
spindles in prime movers are signaling active stretch while those in
antagonists are signaling passive stretch
Renshaw cells
• cocontraction of prime movers & antagonists fix one or more joints
• inactivation of Ia inhibitory internucials by Renshaw cells
Excitatory internuncials
• MN supplying axial & proximal limb m. are recruited indirectly by LCST
using excitatory internuncials in intermediate gray matter & ant. horn base
Targets of LCST
Ia inhibitory internuncials
• Also located in intermediate gray matter
• first neurons to be activated by LCST during
voluntary movements causes antagonist m. to
relax before prime movers contract
Sequence of voluntary movement
(knee flexion)
1) Activation of Ia internuncials to
inhibit antagonist αMN
2) activation of agonist α & γ MN
3) activation of extrafusal &
intrafusal m. fibers
4) feedback from actively stretched
spindles excitation of agonist
αMN & antagonist αMN
5) Ia fibers from passively stretched
antagonist spindles find respective
αMN refractory
DESCENDING MOTOR PATHWAYS
• Important pathways descending to spinal cord are
1. corticospinal (pyramidal) (CST)
2. reticulospinal (extrapyramidal) (RST)
3. vestibulospinal
4. tectospinal
5. raphespinal
6. aminergic
7. Autonomic
c
c
c
Reticulospinal tracts (RST)
• originate in reticular formation of pons &
medulla oblongata
• partially crossed
• PRST (pontine reticulospinal tract)
descends in ant funiculus acts on
extensor MN
• MRST (medullary reticulospinal tract )
Descends (partly crossed) in lat funiculus
flexor MN
• Both tracts act on MN supplying trunk &
proximal limb muscles
• Both pathways exert reciprocal inhibition
• RS system is involved in 2 different kinds
of motor behavior: locomotion &
postural control
Reticulospinal tracts (RST)
Locomotion
• Walking & running are rhythmic events involving all 4 limbs
• 2 side movements are reciprocal to flexor/extensor contractions &
relaxations
• Locomotion: initiated from locomotor center in lower midbrain for
humans (in pons for lab animal)
• pattern generators: intermediate gray matter at upper end of spinal
cord initiate rhythmic movements
• human locomotion is less 'spinal' than quadrupeds
• In human, removal of entire cerebral hemisphere during childhood
or adolescence bilaterally organized motor system controlling
proximal & axial m. exist for return near-perfect locomotor
function, but never recover manual skill on contralateral side
2 distinct pathways: pyramidal vs. extrapyramidal (reticulospinal)
Posture
• position held between movements, e.g. standing, sitting
• postural fixation: immobilization of proximal limb joints by
cocontraction of surrounding muscles, leaving distal limb parts free
to do voluntary business
Resident Evil
DESCENDING MOTOR PATHWAYS
• Important pathways descending to spinal cord are
1. corticospinal (pyramidal) (CST)
2. reticulospinal (extrapyramidal) (RST)
3. vestibulospinal
4. tectospinal
5. raphespinal
6. aminergic
7. Autonomic
c
c
c
Vestibulospinal tract
• originates in vestibular nucleus in medulla
oblongata descends in ant funiculus
• tone of antigravity m. is automatically
increased as head is tilted
• keep center of gravity between feet
Tectospinal tract
• crossed pathway: from tectum of
midbrain med. part of ant gray horn at
cervical & upper thoracic levels
• access to axial MN
• important in reptilian brain
responsible for orienting head-trunk
toward visual or auditory sources
• similar to automatic functions in humans
Raphespinal tract
• originates in/beside raphe nucleus in
medulla oblongata descend on both
sides within Lissauer
• modulate sensory transmission between
1st & 2nd-order neurons in post gray horn
(particular pain)
Aminergic pathways
• from specialized cell groups in pons &
medulla oblongata descend in outer
parts of ant & lat funiculi wide
distributed in spinal gray matter
• neurotransmitters: norepinephrine &
serotonin (classed as biogenic amines)
• inhibitory effects on sensory neurons &
facilitatory effects on motor neurons
Central autonomic pathways
• Originate part from autonomic control centers
in hypothalamus & part from several nuclear
groups in brainstem descend beside
intermediate gray matter terminate in
intermediolateral cell columns to preganglionic
sympathetic & parasympathetic fibers of
peripheral autonomic system
• required for normal baroreceptor reflex
activity
SCI patient blood pressure in carotid sinus as
sitting up compensatory sympathetic
activity to maintain blood flow to brain
• originate in reticular formation tonic
inhibitory on sacral parasympathetic system
required for normal bladder/rectal function
severe injury to spinal cord or cauda equina
results in reflex voiding when is only half full
BLOOD SUPPLY OF SPINAL CORD
Arteries
• Close to foramen magnum, 2 vertebral a. give off
ant/post spinal branches
• ant branches fuse to form a single ant spinal a.
• spinal a. are boosted by several radiculospinal
branches from vertebral & intercostal a.
• small radicular a. enter every intervertebral
foramen to nourish nerve roots
• rare vascular disorders in spinal cord
• artery of Adamkiewicz : largest radiculospinal
a. from lower intercostal or upper lumbar a.
supplies lumbar enlargement & conus
medullaris
be careful when abdominal aortic aneurysm
clamp is placed above a. postoperative
paraplegia with incontinence
Veins
• Drainage by ant/post spinal v. outward along nerve roots
• obstruction edema of cord progressive loss of function
Clinical
Panel
16.3
Spinal
cord
injury
automobile accidents are commonest cause of SCI (16 ~30 y/o with cervical injury)
•
• T & L level results in paraplegia (paralysis of lower limbs)
C level causes tetraplegia (quadriplegia)
Spinal shock
• Below injury level in first few days following a complete cord transection
1.
2.
3.
4.
Paralysis movement
limbs flaccid & absent tendon reflexes
Anesthesia (loss of all forms of sensation)
Paralysis of bladder & rectum
• hyperpolarization of spinal neurons below lesion level (release inhibitory transmitter glycine)
• patient develops postural hypotension interruption of baroreceptor reflex wearing an
abdominal binder for compensation
Return of spinal function
• Several days or weeks later
1.
2.
3.
4.
5.
Reflex progressively restored & upper motor neuron signs appear
Muscle tone becomes excessive (spastic)
Tendon reflexes become abnormally brisk
Babinski sign can be elicited on both sides
Ankle clonus is commonly seen
• bladder condition is important for 2 dangers on infection & formation of bladder stones
initial, atonic bladder, insert a sterile catheter to ensure unobstructed drainage
later, automatic bladder, emptying itself every 4-6 h through a reflex arc
• Considerable interest has been aroused by observations in several spinal rehabilitation centers,
patients with complete cord transections can be trained to activate spinal locomotor generators
Question 7 (2 point)
• Which of the following symptoms can be
observed in chronic complete SCI patients
B
A
C
Ans: (1) A only; (2) A+B; (3) A+B+C; (4) B+C
sensory
motor
PCML (motor)
Spinocerebellar
c
Spinothalamic
(Pain, Touch)
c
c
Thanks for your attention!!