Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
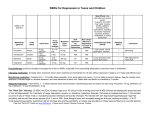
SSRI’s and the Black Box Warning: Patient Advocacy or Alarmist Propaganda? Master’s Project Presentation Lucas Kennedy April 3, 2008 Adolescent Depression: the basics • Major Depressive Disorder is defined by the DSM as follows: “Either depressed /irritable mood or loss of pleasure along with at least three other symptoms present over the same 2 – week period” Prevalence • Depression is estimated to occur in 2% of all children (under 12 years old) and 4 – 8% of adolescents (those 12 – 18). • 20% of all American adolescents will experience a bout of certified clinical depression by 18 and about 65% will experience more fleeting episodes. • 20-40% of adolescents diagnosed with MDD will subsequently receive a bipolar diagnosis while 75% will later be diagnosed with an anxiety disorder. Suicide Statistics • About 50% of adolescents diagnosed with MDD will experience a suicide attempt. • This same group is four to five times more likely to attempt suicide at some point in their lives than teenagers who are not depressed. • Approximately 90% of persons who commit suicide have been found to suffer from bipolar disorder, major depression or some other psychiatric disorder upon psychological autopsy. Trends in Treatment Number of office visits where children and adolescents reported depression 1995-96 2002-03 1.44 million 3.22 million Percentage prescribed antidepressants 47% 52% Percentage of patients who were prescribed SSRI’s 76% 81% 83% 68% Proportion of patients who received psychotherapy of mental health counseling A History of Controversy • December of 2003: National Institute for Health and Clinical Excellence (NICE) in Great Britain declared all SSRI’s but fluoxetine to be not only ineffective but actually increase chances of suicide related events one to three fold, effectively banning their use in those under 18 years of age. • October of 2004: The FDA announces a “black box warning” associated with the use of all antidepressants in patients under the age of 18 as a caution to both patients and practitioners about the hazards of prescribing antidepressants in youth. Australia, New Zealand and Canada soon followed suit with restrictions of varying degrees on antidepressant usage in children and adolescents. The FDA’s Numbers • The “black box warning” instituted by the FDA was based upon a meta-analysis of 24 placebo controlled randomized trials involving 4400 youth with OCD, MDD and other psychiatric disorders. • Studies on nine separate medications, including SSRI’s and some other drug classes, were included in the metaanalysis. • The FDA found that the risk of suicidal thinking or behavior amongst patients receiving active drug was 4% while those receiving placebo had a risk of only 2%. Further Studies • JAMA completed another meta-analysis in April of 2007 of 13 studies involving pediatric depression which included a total of 2910 patients. • These studies involved both SSRI’s and second generation antidepressants such as nefazodone and mirtazepine. • They found that the rate of suicidality in active treatment groups was 3% while the rate in those receiving placebo was 2%. • The calculated risk difference resulted in a NNH of 112. • The pooled risk difference between the groups was 1% with a 95% C.I. of -0.1% to 2%. As a result, JAMA found the risk of increased suicidal ideation to be statistically insignificant. The Power of Anecdotal Evidence • Not a single completed suicide has been reported during clinical trials of any antidepressant currently being used in the treatment of youth MDD. Let me repeat……………. • Not a single completed suicide has been reported during clinical trials of any antidepressant currently being used in the treatment of youth MDD. Part of the Problem • The field of research involving antidepressant usage in youth is relatively young itself: The very first randomized controlled trial specifically designed to measure the efficacy of antidepressants in children was conducted in 1997. • As a result, we do not have a large body of work to draw from as practitioners to assess risk or efficacy of pharmaceutical antidepressants in children and adolescents. • This also leaves open the possibility that some of the more severe or rare side effects may not be observed until these drug therapies have been used in much larger segments of the population (i.e. hundreds of thousands or millions) Part of the Problem • None of the trials used by the FDA, JAMA or any other organization were originally designed to measure suicidal behavior or tendencies. • All of these studies were designed to assess efficacy of antidepressants in relieving depressive symptoms. • Information on suicidality included in the FDA report, and all subsequent meta-analyses, was based on retrospectively assessed definitions applied to information gleaned from adverse event logs and psychological questionnaires. • Richmond made note of this in a 2005 review: “these trials were not designed to detect a difference in suicidality, leading to heterogeneity in the manner in which adverse events data were collected.” Part of the Problem Another valid concern is the lack of any defining characteristics for many of the phrases that get tossed about concerning suicidal behavior. “In the American studies, the concept of suicidality was no more clearly demarcated than what constituted a child. Terms used to define suicidality included – though not in any uniform way across studies – behavioral activation (itself a vague concept), disinhibition, impulsivity emotional lability, self-inflicted harm, suicide ideation, suicide attempts and completed suicide. In one study, a child who slapped herself was considered to be suicidal, as was another child, who in a fit of anger banged his head into a wall. An event involving a child frustrated by his school performance who stabbed himself in the neck with a pencil was labeled merely an accident.” John Bostwick: Mayo Clinic Part of the Problem What is the relative danger of suicidality? Vitiello and Swede noted: “suicidal ideation is not an accurate predictor of suicide since most persons with such ideation do not attempt to die by suicide.” Part of the Problem • Selection of subjects for inclusion in studies of pharmaceutical treatment of youth depression up until this point has been highly exclusionary. • The vast majority of researchers have disqualified any patients found to have drug or alcohol dependency or co-morbid psychological diagnoses such as bipolar disorder or schizophrenia. • Most importantly, patients who are actively suicidal have been completely excluded from most of the studies. Gibbons et al noted: “by design, the randomized controlled trials analyzed by the FDA systematically excluded patients who were actively suicidal, and thus the FDA lacks data on those who are at highest risk for suicide.” How Did This Happen? Time Magazine published an article in February of 2004 titled: Prescription for Suicide? At the beginning of the article the following narrative was included: Kara Jaye-Anne Otter, 12, had been on the antidepressant Paxil for seven months when she committed suicide. “I was told the worst side effects would be flulike symptoms,” recalls her mother, Shannon Baker. “But after three weeks she had begun to cop an attitude. Her grades started falling. Then she didn’t care what she looked like, and she was fighting with everybody.” Baker says her daughter developed rashes and dark circles under her eyes and had trouble sleeping. Then, on June 3, 2001, Kara pinned a note to her chest reading, “By the time you find me I’ll be dead. I love you with all my heart. Don’t worry, Jesus is with me.” She hooked a bungee cord onto a plate hanger on the wall, wrapped the cord around her neck and pulled against it until she passed out. Within minutes she was dead. (Lemonick, 2004) How Did This Happen? The article does go on to present a simplified but accurate summation of the controversy over prescription of SSRI’s in youth including arguments by physicians who support the continued use of these medications in the treatment of depression, however, the damage has been done. Most people reading this article are not going to come away with the message that many practitioners still believe that SSRI’s are an important pharmaceutical option for depressed youth. The majority of the people who read this article are going to remember the vivid description of Kara Jaye-Anne Otter’s suicide, and furthermore that this tragic sequence of events was triggered by an antidepressant. MOVIE TIME!!!!! MOVIE TIME!!!!! MOVIE TIME!!!!! MOVIE TIME!!!!! Pitfalls to Practice • The Pediatric Advisory Committee along with the FDA have crafted the following recommended monitoring program in the event that antidepressants are prescribed in youth: “weekly visits for the 1st month of treatment, bimonthly during the 2nd month and once every 12 weeks for the remainder of the dosing period.” • Many parents may be unable or unwilling to bring their children in for follow up on such a frequent basis. Pitfalls to Practice • A great majority of primary care providers in underserved areas may not have access to specialized psychiatric treatment for their pediatric patients and will be forced to care for these complex cases with extremely limited resources. • Many of these practitioners will be forced to prescribe SSRI’s “off label” for fear that not prescribing may increase the risk of suicide in their patient. • Through initiating a “black box warning” and not an outright ban on all antidepressants in youth the FDA has placed many practitioners between a rock and a hard place, effectively washing their hands of the matter. What’s the Solution? • While we as practitioners may or may not agree that recent headlines concerning SSRI’s and their connection to self harm in youth are overblown, we must still err on the side of caution. • Because most of the studies on youth depression have excluded individuals with many predisposing factors that could increase risk of suicide, we must be hypervigilant with usage of antidepressants in those particular patients who suffer from comorbid psychiatric of medical conditions. What’s the Solution? • Parents and guardians must be warned of the possibility for increased suicidal behavior in youth during the first few weeks of treatment with antidepressant medications. • Practitioners should consider the competency of their patient’s parent or guardian particularly regarding the probable level of vigilance they may have regarding a child’s changing psychological symptoms. • We must weigh the severity of a patient’s depression and it’s likelihood to cause them physical harm against the possibility that his or her caretaker may not remain observant enough to assess an increase in the youth’s suicidal behavior due to institution of antidepressant treatment. What’s the Outcome? • If we as health care workers can become more vigilant in our treatment of depressed youth while not being gun shy in prescribing antidepressants in appropriate situations, I think mental health care in the United States will improve drastically. • If, however, all these black box warnings and alarmist decrees scare us away from appropriate pharmaceutical interventions for fear of increased liability, the most vulnerable of our mentally ill youth will undoubtedly suffer the most. SOURCES • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • BIBLIOGRAPHY Bostwick, John Michael, (2006). Do SSRIs Cause Suicide in Children? The Evidence is Boylan, Khrista, Romero, Soledad, & Birmaher, Boris, (2007). Psychopharmacologic 191, 2738. Bridge, Jeffrey A., Iyengar, Satish, Salary, Cheryl B., Barbe, Remy P., Birmaher, Boris, and Risk for Reported Suicidal Ideation and Suicide Attempts in Pediatric Trials. JAMA, 297 (15), 1683 – 1696. The Diagnostic and Statistical Manual of Mental Disorders IV. 1994. American Psychiatric Association. Gibbons, Robert D., Brown, C. Hendricks, Hur, Kwan, Marcus, Sue M., Bhaumik, Dulal Evidence On the Effects of Regulators’ Suicidality Warnings on SSRI Psychiatry, 164, 1356 - 1363. Lemonick, Michael D. (2004) Prescription for Suicide? Time, February 1, 2004. Mann, John J., Emslie, Graham, Baldessarini, Ross J., Beardslee, William, Fawcett, Jan D., Shaffer, David, & Wagner, Karen D. (2006). ACNP Task Force Report on 492. Olfson M, Gameroff MJ, Marcus SC, Waslick BD. (2003). Outpatient treatment of child and adolescent depression in the United States. Archive of General Psychiatry, 60: 1236-1242. Richardson, Laura P., Lewis, Charlotte W., Casey-Goldstein, Mary, McCauley, Elizabeth Katon, Wayne. (2007). Pediatric Primary Care Providers and Adolescent Depression: A Qualitative Study of Barriers to Treatment and the Effect of the Black Box Warning. Journal of Adolescent Health, 40, 433 – 439. Sharp, Susan C., & Hellings, Jessica A. (2006). Efficacy and Safety of Selective SSRI’s in the Treatment of Depression in Children and Adolescents. Clinical Drug Investigations, 26 (5), 247 – 255. US Food and Drug Administration. (2004). Suicidality in children and adolescents being treated with antidepressant medications. FDA Public Health Advisory, October, 18, 2004. Valuck, Robert J., Libby, Anne M., Sills, Marion R., Giese, Alexis A., Allen, Richard R. (2004). Antidepressant Treatment and Risk of Suicide Attempt by Adolescents with Major Depressive Disorder: A Propensity-Adjusted Retrospective Cohort Study. CNS Drugs, 18 (15), 1119-1132. Varley, Christopher K. (2006). Treating Depression in Children and Adolescents: What Options Now? CNS Drugs, 20 (1), 1-13. Vitiello, B., Swedo, S. (2004). Antidepressant Medications in Children. The New England Journal of Medicine, 350 (15), 1489-1491. Underwhelming. Journal of Clinical Psychology, 62 (2), 235 – 241. treatment of pediatric major depressive disorder. Psychopharmacology, Pincus, Harold Alan, Ren, Lulu, & Brent, David A, (2007). Clinical Response Antidepressant Treatment: A Meta-Analysis of Randomized Controlled K., Erkens, Joelle A., Herings, Ron M.C., & Mann, J. John. (2007). Early Prescriptions and Suicide in Children and Adolescents. American Journal of A., Goodwin, Frederick K., Leon, Andrew C., Meltzer, Herbert Y., Ryan, Neal SSRIs and Suicidal Behavior in Youth. Neuropsychopharmacology, 31, 473