Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
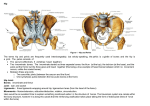
Anatomy & Injuries to the Thigh, Hip and Pelvis SP Sports Medicine John Hardin Instructor General Information about the pelvis This area of body is strong and stable Great demand placed on this part of body— ”core” Functions: support the spine & trunk Transfer weight to lower extremities Place for muscle attachment of thigh and trunk Protect organs of pelvic region Anatomy Bones Muscles Ligaments Bones Femur Head, neck, greater trochanter, lesser trochanter, shaft, medial & lateral condyle and epicondyles Pelvis Ilium: iliac crest, ASIS, AIIS, PSIS Ishcium: ischial tuberosity Pubis: Pubic symphysis Acetabulum Bones-the anterior femur The posterior femur The pelvis Muscles Hip Flexors: Iliacus & psoas major= Iliopsoas Rectus femoris Sartorius Hip Extensors: Hamstrings-biceps femoris, semitendinosus, semimembranosus Gluteus maximus Muscles Knee flexors: Hamstrings, gastrocnemius Knee extensors: Quadriceps—rectus femoris, vastus lateralis, vastus medialis, vastus intermedius Muscles Muscles Muscles Muscles Hip Adductors: Adductor magnus, adductor longus, adductor brevis, gracilis, pectineus Hip Abductors: Gluteus medius, tensor fascia latae Muscles Muscles Muscles Hip Internal rotators: Tensor fascia latae, gluteus minimus Hip External rotators: Gluteus maximus, gluteus medius, piriformis Ligaments Thickening of joint capsule allows for very stable joint Iliofemoral Ischiofemoral pubofemoral Ligamentum Teres Also called the round ligament Attaches head of femur into acetabulum allowing blood supply to that area Ligaments Preventing injuries to thigh/hip Flexibility training and stretching Strength training Proper protective equipment Common Injuries Strains Sprains Contusions Fractures Dislocations Strains Quads Hamstrings Groin (adductors) Hip flexors Gluteals Strains Mxn: sudden strong contraction of muscle(s) overstretching of muscle(s) Muscle strength imbalance Strains-hamstring Strains- groin Strains S/S: pain/discomfort POT Bleeding causing discoloration (after 1-2 days) Loss of function Muscle spasm deformity Strains TX: RICE modify/restrict activity crutches if necessary Medical referral if necessary Restore normal ROM flexibility and strength using various modalities as needed Strains Complications: recurrent strains due to “inelasticity of scar tissue” especially at that same site Excess buildup of scar tissue Strains-quad after the fact Strains-quad Strains-hamstring Strains-hamstring Hamstring strain treatment Hamstring avulsion Contusions Quadriceps Hip pointer Quadriceps Contusion Mxn: direct blow to relaxed thigh compressing the musculature again the femur Quadriceps Contusion S/S: Pain POT Bleeding into the muscle Swelling Temporary loss of function Quad contusion Tx: RICE w/ knee flexed Crutches if necessary Restore normal ROM, flexibility & strength Ultrasound Heat Medical referral if needed Quad contusion Complication: Myositis ossificans—formation of bony tissue within the muscle Very painful Greatly restricts ROM mainly flexion Caused by: severe blow that is not properly cares for Repeated blows to same area Myositis Ossificans Hip Pointer Mxn: direct blow to the iliac crest and/or ASIS S/S: Pain Spasm Bleeding in the area—discloration Temporary loss of motion Unable to rotate trunk or flex hip without pain Hip Pointer Hip Pointer Tx: RICE Bed rest if necessary Medical referral if necessary Return to activity when pain if gone and motion is restored Fractures-Avulsion Most common at ASIS or Ischial Tuberosity Mxn: forceful contraction of muscle Avulsion Fractures S/S: Extreme pain with movement & weight bearing POT (either over the ASIS or Ischial tub.) Bleeding/discoloration Avulsion TX: Ice crutches Medical referral for x-ray Fractures- femur Occurs most often in the shaft of the femur Mxn: great force-direct or indirect- placed on the femur Femur Fractures S/S: Pain POT Deformity w/ thigh externally rotated, shortened Loss of motion/function Swelling due to internal bleeding Muscle spasms Muscle lacerations Femur fractures Can be life threatening—fatty tissue and bone marrow can get into the blood stream and cause a blood clot Femur Fracture Tx: Call 911 Don’t move the athlete Hare traction splint Check for distal pulse Control any external bleeding Treat for shock Femur fractures Femur fractures Femoral Stress Fracture Mxn: repetitive stress of the pounding of the lower extremity which causes the femur to bend (one side is compressed the other is stretched) Femoral stress fracture S/S: POT at one specific site Pain with activity Pain with a compressive force at the site (sitting on edge of table) Pain with activity Femoral Stress fracture Tx: Rest Alternate activity—non-weight bearing Crutches if limping Medical referral---x-rays and bone scan or-- Femoral stress fx Slipped Capital Femoral Epiphysis Growth plate injury (epiphyseal fracture) Occurs at the capital femoral epiphysis (where neck joins the head of femur) More common in boys 10-17 yrs. Tall and thin obese Slipped Capital femoral epiphysis Mxn: Not know but may be related to effects of a growth hormone In ¼ of cases both hips are affected Slipped---epiphysis S/S: Pain in groin area that arises suddenly as a result of trauma arises slowly over weeks or months as a result of prolonged stress Early signs minimal but later get pain in hip and knee Major limitations with movement Limp when walking Slipped --- epiphysis TX: Minor cases Rest Non-weight bearing to prevent further slippage Medical referral Major cases Surgery to repair “fracture” usually put pins into bone to keep in place and allow for proper healing Slipped---epiphysis Complications: If displacement goes undetected or if surgery fails to restore normal hip mechanics can have problems later in life Bone doesn’t grow properly Head of femur doesn’t grow properly Bone spurs Arthritis SCFE SCFE SCFE Pins to fix Legg-Calve-Perthes Disease Disruption of blood flow to the head of femur causing the bone tissue to die and become flattened Occurs in children 3-12 yrs Occurs in boys 4 times more often than girls Usually occurs in first born Affect usually only one hip LCPD Mxn: Unknown S/S: complaints of pain in groin, and sometimes referred pain to abdomen or knee Limited hip movement LCPD Tx: Medical referral Bed rest or non-weight bearing If treated in time, the head of femur will revascularize and regain its normal shape (the old cells that die will be resorbed and new bone cells laid down to take their place) LCPD LCPD Complications: If not treated early enough, the head of femur will be ill (abnormally) shaped producing osteoarthritis in later life Hip Dislocation Rarely occurs in sports Most are posterior Mxn: traumatic force along the long axis of the femur such as falling on one side with the knee bent (and landing on that bent knee) forcing head of femur posteriorly Hip Dislocation S/S: Hip in flexion, adduction, and internal rotation Deformity posterior—head of femur can be palpated through gluteal muscle Extreme pain Inability to move at hip joint Hip Dislocation Hip Dislocation Hip Dislocation TX: Call 911 Don’t move athlete Splint in position you find them Treat for shock Hip Dislocation Complications: Tears in the vascular and nerve structures Blood vessels to ligamentum teres may be torn (as will the ligament itself) Sciatic nerve may be damaged Paralysis of muscles in the area Atrophic necrosis (degeneration of femoral head)