Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
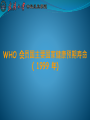
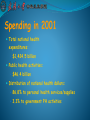
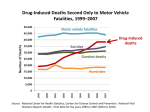
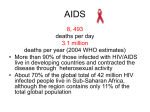
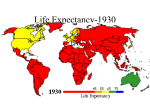
English for special purpose in Public health Introduction to public health and preventive medicine Story of life expectancy Mortality Rate CIA World Factbook 2007 Estimates for Life Expectancy at birth (years). 按联合国会员排名 按国家或地区排 名 国家或地区 总预期寿 命 男性预期寿 命 女性预期寿 命 1 澳門特別行政區 84.33 81.36 87.45 1 2 安道爾 82.67 80.35 85.14 2 3 日本 82.07 78.73 85.59 3 4 新加坡 81.89 79.29 84.68 3 5 聖馬利諾 81.88 78.43 85.64 6 香港 81.77 79.07 84.69 7 吉布拉塔(英國) 80.9 78.5 83.3 5 8 瑞典 80.63 78.39 83 6 9 澳洲 80.62 77.8 83.59 7 10 瑞士 80.62 77.75 83.63 8 11 法國 80.59 77.35 84 12 根西島(英國) 80.53 77.53 83.64 9 13 冰島 80.43 78.33 82.62 10 14 加拿大 80.34 76.98 83.86 76 103 土耳其 72.88 70.43 75.46 76 103 中國 (mainland) 72.88 71.13 74.82 79 106 馬來西亞 72.76 70.05 75.65 80 114 巴西 72.70 69.0 76.50 81 107 聖克里斯多福及尼維斯 72.66 69.81 75.69 82 108 保加利亞 72.57 68.95 76.4 83 109 泰國 72.55 70.24 74.98 84 110 安地卡及巴布達 72.42 70.03 74.94 85 111 塞席爾 72.34 66.98 77.86 86 112 愛沙尼亞 72.3 66.87 78.07 87 113 哥倫比亞 72.27 68.44 76.24 173 203 索馬里 48.84 47.06 50.69 174 204 奈及利亞 47.44 46.83 48.07 175 205 查德 47.2 46.17 48.27 176 206 幾內亞比索 47.18 45.37 49.04 177 207 尼日 44.03 44.05 44 178 208 阿富汗 43.77 43.6 43.96 179 209 中非 43.74 43.69 43.79 180 210 吉布地 43.25 41.88 44.65 181 211 納米比亞 43.11 44.39 41.79 182 212 馬拉威 42.98 43.35 42.61 183 213 南非 42.45 43.21 41.66 184 214 莫三比克 40.9 41.4 40.4 185 215 獅子山 40.58 38.36 42.87 186 216 賴比瑞亞 40.39 38.93 41.89 187 217 賴索托 39.97 40.73 39.18 188 218 辛巴威 39.5 40.62 38.35 189 219 尚比亞 38.44 38.34 38.54 190 220 安哥拉 37.63 36.73 38.57 191 221 史瓦濟蘭 32.23 31.84 32.62 Major Reasons for Increased Longevity Improved sanitation Provision of clean water Universal immunization programs Health education and prevention practices Improved treatment of chronic diseases (for recent advances) Healthy life expectancy Disability Adjusted Life Expectancy How it is caculated? Morbidity and Mortality of commen diseases Living habits Social Violence Dietary pattern Substance abuse(drug,alcohol) Medical facilities Environment Climate And How many year been disability in average (subtract this number from life expectancy) WHO 会员国主要国家健康预期寿命 ( 1999 年) 排名 国 家 ( 歲 ) 健康预期寿命 ( 岁 ) 1 日本 74.5 2 澳洲 73.2 3 法国 73.1 4 瑞典 73.0 5 西班牙 72.8 6 意大利 72.7 7 希腊 72.5 7 瑞士 72.5 9 摩纳哥 72.4 10 安道尔侯国 72.3 10 圣玛利诺 72.3 12 加拿大 72.0 12 荷兰 72.0 14 英国 71.7 14 挪威 71.7 16 比利时 71.6 16 澳地利 71.6 18 卢森堡 71.1 19 冰岛 70.8 20 芬兰 70.5 20 马尔他 70.5 22 德国 70.4 22 以色列 70.4 24 美国 70.0 25 塞浦路斯 69.8 26 多明尼加 69.8 27 爱尔兰 69.6 28 丹麦 69.4 29 葡萄牙 69.3 29 新加坡 69.3 31 纽西兰 69.2 32 智利 68.6 33 古巴 68.4 33 斯洛法尼亚 68.4 35 捷克 68.0 36 牙买加 67.3 37 乌拉圭 67.0 37 克罗埃西亚 67.0 39 阿根廷 66.7 40 哥斯大黎加 66.7 . . . . . . 81 中国大陆 62.3 . . . . . . . . . 186 乌干达 32.7 187 波札纳 32.3 188 尚比亚 30.3 189 马拉威 29.4 190 尼日 29.1 191 狮子山 25.9 Sources: UN Healthy Life Expectancy Ratings J.P.Bunker’ s report (1994 published) Life expentancy from 45-75 years Medical care contributes to only five years Improvement of public health contributes to the rest Spending in 1992 Average medical care cost for each person: $3007 Public health spending for each person: $34 Distribution of national health dollars on public health: About 1% Spending in 2001 Total national health expenditures: $1,424.5 billion Public health activities: $46.4 billion Distribution of national health dollars: 86.8% to personal health services/supplies 3.3% to government PH activities Requirements for survival 1.air 2.water 3.food 4.shelter 5.care Health The United Nations' World Health Organization defines health as "a state of complete physical, mental and social well- being and not merely the absence of disease or infirmity." What is Public health? In 1920, C.E.A. Winslow defined public health as "the science and art of preventing disease, prolonging life and promoting health through the organized efforts and informed choices of society, organizations, public and private, communities and individuals." The history of public health Public health is an old concept, dating back to when people first began living in communities. Through the ages, governments have shown varying degrees of concern for the public health. The ancients Greeks, and the Romans after them, tried to ensure the health of their citizens by providing a supply of clean water (via aqueducts and pipelines), managing the disposal of waste working to control disease by hiring public physicians to treat the sick. During the late 1800s European governments began turning their attention to matters of public health in an effort to control the spread of disease. (Because Epidemics of leprosy, the plague, cholera, and yellow fever). In the United States, the public health became an official concern when in 1866 a cholera epidemic struck the nation-for the eighteenth consecutive year What is Public health? "the science and art of preventing disease, prolonging life and promoting health through the organized efforts and informed choices of society, organizations, public and private, communities and individuals." The 'science' is concerned with making a diagnosis of a population's health problems, establishing their cause, and determining effective interventions. The 'art' is to address these problems creatively. This definition underscores the broad scope of public health and the fact that public health is the result of society’s efforts as a whole, rather than that of single individuals. In 2003, Detels defined the goal of public health as: The biologic, physical, and mental well-being of all members of society regardless of gender, wealth, ethnicity, sexual orientation, country, or political views. (This definition or goal emphasizes equity and the range of public health interests as encompassing not just the physical and biologic, but also the mental well-being of society.) Both WHO and Detels’ goals depict public health as being concerned with more than merely the elimination of disease. To achieve the WHO goal of ‘health for all’, it is essential to bring many diverse disciplines to obtain the optimal health (physical, biologic, and social sciences) . The field of public health has adapted and applied these disciplines for the elimination and control of disease, and the promotion of health. 1988 <the future of public health> Mission: Substance: Organizational framework: Core functions: mission The fulfillment fo society’s interest in assuring the conditions in which people can be healthy Substance Organized community efforts aimed at the prevention of disease and the promotion of health Organizational framework Bothe activities undertaken within the formal structure of government and the associated efforts of private and voluntary organizations and individuals Core functions Assessment Policy development Assurance Monitor Health Status to Identify and Solve Community Health Problems Diagnose and Investigate Health Problems and Health Hazards in the Community Inform, Educate and Empower People About Health Issues Mobilize Community Partnerships to Identify and Solve Health Problems Develop Policies and Plans That Support Individual and Community Health Efforts Enforce Laws and Regulations That Protect Health and Ensure Safety Link People to Needed Personal Health Services and Assure Health Care When Otherwise Unavailable Assure a Competent Public Health and Personal Health Care Workforce Evaluate Effectiveness, Accessibility, and Quality of Personal and Population- Based Health Services Research for New Insights and Innovative Solutions to Health Problems 5 steps process 1. Define the health problem 2. Identify the risk factors associated with the problem 3. Develop and test community-level interventions to control or prevent the cause of the problem 4. Implement interventions to improve the health of the population 5. Monitor those interventions to assess their effectiveness The science of Public health Epidemiology and statistics Biomedical sciences Social and behavior sciences Environmental sciences Health policy and management Health management Ten Great Achievements in Public Health 1900-1999 Vaccination. Weekly Report, December 24, 1999 / 48(50); 1141. 2. Motor-vehicle safety. 3. Safer workplaces. 4. Control of infectious diseases. 5. Decline in deaths from coronary heart disease and stroke. 6. Safer and healthier foods. 7. Healthier mothers and babies. 8. Family planning. 9. Fluoridation of drinking water. 10. Recognition of tobacco use as a health hazard. 1. CDC, Morbidity and Mortality Challenges Ahead New and Persistent Problems in Public Health Leading causes of death,worldwide 2001 Perinatal conditions 4.4% Respiratory infections 7.0% Others 8.6% Infectious & parasitic 19.3% Injuries 9.0% Respiratory & digestive 9.8% Source: WHO 2002 Malignant neoplasms 12.6% Cardiovascular diseases 29.3% (suicide) Leading infectious killers, worldwide 2001 Respiratory infections 3.9 4 3.9 HIV/AIDS 2.9 Diarrhoeal diseases 2 TB 1.6 3.5 Malaria 1.1 Measles 0.7 2.9 3 2.5 2.0 2 1.6 1.5 1.1 1 0.7 0.5 Source: WHO 2002 0 Respiratory infections HIV/AIDS Diarrhoeal diseases TB Malaria Measles Under-five mortality rate, 1990-2003 Child deaths per 1,000 live births 1990 2003 World 95 80 Developed regions 11 7 46 46 Developing regions 105 88 Northern Africa 87 38 Sub-Saharan Africa 185 172 54 32 Eastern Asia 48 37 Southern Asia 126 90 South-Eastern Asia 78 46 Western Asia 68 60 Oceania 86 77 Commonwealth of Independent States Latin America and the Caribbean Source: United Nations Statistics Division, “World and regional trends”, Millennium Indicators Database, available from http://millenniumindicators.un.org (accessed June 2005); based on data provided by United Nations Children’s Fund and the World Health Organization. Statistics Division, Department of Economic and Social Affairs Distribution of deaths by broad causes group and region 2001 Deaths (thousands) Total Group I Group II Group III Group II/Group I ratio World 56554 18374 33077 5103 1.8 Developed 15614 1441 12833 1320 8.9 Developing 40940 16933 20244 3783 1.2 Group I: Communicable diseases, maternal and perinatal conditions and nutritional deficiencies Group II: Noncommunicable conditions Group III: Injuries Source: WHO (2002) Health Disparities Access and Outcomes Infant Mortality Cancer Screening and Management Cardiovascular Disease Diabetes HIV Infection/ AIDS Immunizations Contemporary health issues The 20th century witnessed the transition of major disease burdens ( defined by death) from infectious and/or communicable diseases to chronic diseases (Table 1.1.2). In 1900, the leading cause of death in the United States and other developed countries was reported to be pneumonia and influenza. By the end of the century, diseases of the heart were the leading cause of death, and pneumonia and influenza dropped to the seventh place, primarily affecting the elderly. Communicable diseases Chronic diseases Mental illness Population changes: Ageing Pollution Disparity between the rich and the poor widen Public health interventions One important task of public health professionals is to raise the level of anxiety of the public about public health problems to the level at which they will be willing to take an appropriate action. Public health interventions can be divided into four categories: biologic/environmental social/behavioral political structural The public health professional must use strategies in all categories to achieve the maximum health of the public. biologic / environmental interventions The strategies: improved standard of living, including provision of clean water and safe disposal of wastes. The most cost-effective biologic intervention strategy is immunization Eliminate of vectors of disease: DDT Social/Behavior interventions Most public health interventions depend ultimately on behaviour ( personal or community behavior). At the personal or individual level, promotion of good health habits and avoidance of smoking, excess alcohol use, and other dependency disorders are important interventions that have a major impact on health. Political interventions Public health is politics. Any process that involves obtaining the support of the public will involve politics and differing points of view. For example, the campaign to stop smoking Structural interventions The end result of the political process is the passage of laws and regulations. This action, if implemented, can have a very significant impact on the improvement of the health of the public. For example, the law reducing the maximum speed in California from 65 to 55 miles per hour had a significant impact on lowering the automobile fatality rate Impact of public health The dramatic achievements of public health in the 20th century have improved our quality of life: an increase in life expectancy. world wide reduction in infant and child mortality elimination or reduction of many communicable disease. As life expectancy increases in many developing countries, more people are developing those chronic diseases which have been a major burden in developed countries for many decades. Unlike developed countries, however, these countries still carry the burden of infectious diseases which have been greatly reduced in developed countries. Because of the rapid advances in travel and communications, the developed world is threatened in new ways and thus cannot afford to ignore the problems of the developing world. Today, public health leaders must strengthen their roles as advocates for improved population-based health in an international, global community. The future of public health We have made tremendous strides to improve the health of the public, but the challenge to do better remains Leading cause of preventable death Leading causes of preventable deaths in the United States as of the year 2000. Cause Number of deaths resulting Smoking 435,000 deaths or 18.1% of the total deaths Overweight and Obesity 365,000 deaths or 15.2% of the total deaths. Alcohol consumption 85,000 deaths or 3.5% of the total deaths. Infections 75,000 deaths or 3.1% of the total deaths. Toxic agents 55,000 deaths or 2.3% of the total deaths. Motor vehicle collisions 43,000 deaths or 1.8% of the total deaths. Incidents involving firearms 29,000 deaths or 1.2% of the total. Sexually transmitted infections 20,000 deaths or 0.8% of the total. Illicit use of drugs 17,000 deaths or 0.7% of the total deaths. Why is public health controversial? Economic impact Individual liberty Moral and religious opposition Political interference with science Multiple Determinants of Health Policies and Interventions Behavior Physical Environment Individual Biology Access to Quality Health Care Source: U.S. Department of Health and Human Services, Health People 2010 Social Environment What is preventive medicine? The branch of medicine that is concerned with the prevention of disease and methods for increasing the power of the patient and community to resist disease and prolong life. Preventive medicine is a medical discipline which focuses on preventing diseases and promoting a general state of health and well being. In both Europe and the United States, it is considered to be a board specialty, meaning that physicians can focus on preventive medicine while they get their medical degree, and use the skills they learn in school to reduce the outbreak of disease epidemics, improve public health, and increase the general quality of life for individuals all over the world. Preventive medicine Healthcare: health departments, academic institutions, state and national government, international or global institutions including the WHO, UN agencies or government agencies like the CDC or NASA, organized medical care programs in industry, voluntary health agencies, and the military. The history of preventive medicine Dating back for centuries to the time (Romes) when people first realized that unclean water made them sick, and that living conditions needed to be more hygienic to prevent illness. Twentieth century, when numerous governments founded disease prevention centers such as the Centers for Disease Control and Prevention (CDC) in the United States. These scientific establishments began to set firm guidelines designed to minimize the transmission of disease, improve hygiene, and enable rapid responses to major outbreaks In addition to medicine and science, preventive medicine also looks at economic and social issues, as some populations are clearly more at risk of contracting dangerous diseases than others. Many sociologists, psychologists, and economists work in the field of preventive medicine to assist people of low income, education, and social status all over the world. Organizations which promote preventive medicine work closely with these individuals in the hopes that all people on earth can enjoy healthy, disease free lives. Training: Generally requires 2 years in residency after a clinical internship or transitional year. Training includes earning a Master of Public Health (MPH) degree which is usually done in one of the two years. There are three specialty areas within preventive medicine: General Preventive Medicine & Public Health Occupational and Environmental Medicine Aerospace Medicine Core courses: biostatistics epidemiology management administration clinical preventive medicine occupational or environmental health. Specific career paths: managed care public health practice occupational medicine environmental medicine aerospace medicine clinical medicine informatics policy development academic medicine consulting international medicine and research. What differences between public health and medicine? Medicine Individual Health Best outcome for individual Public Health Population Health Healthy community Balance of individual autonomy vs. limitations on individual Balance in allocation of resources Focus on prevention Medicine Individual Health Public Health Population Health Thermometer Demographics Stethoscope Vital statistics Individual data, Epidemiology medical history