Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sarcocystis wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Lyme disease wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Leptospirosis wikipedia , lookup
Chagas disease wikipedia , lookup
Hepatitis C wikipedia , lookup
Schistosomiasis wikipedia , lookup
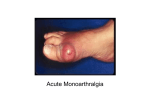
This lecture was conducted during the Nephrology Unit Grand Ground by Medical Student under Nephrology Division under the supervision and administration of Prof. Jamal Al Wakeel, Head of Nephrology Unit, Department of Medicine and Dr. Abdulkareem Al Suwaida, Chairman of Department of Medicine and Nephrology Consultant. Nephrology Division is not responsible for the content of the presentation for it is intended for learning and /or education purpose only. Arthritis Mono vs. Poly Presented By: Ali Al-blowi Medical Student Defenitions Causes History Examination Investigation Conclusion Definitions Arthritis = inflammation of a joint. Inflammation = Joint pain, stiffness, tenderness, redness, hotness, swelling & limited movement. Mono arthritis = one joint affected. Poly arthritis > 4 joints affected. Oligo/pausi-arthritis = 2-4 joints affected. Acute = < 6 weeks Chronic = > 6 weeks Symptoms: Articular symptoms Non articular symptoms Causes Monoarthritis mimickers: • Common inflammatory processes occur in the soft tissues around joints: Tendonitis of the shoulder. Olecranon bursitis of the elbow. Prepatellar bursitis of the knee. Diseases Causing Monoarticutar Symptoms: A) Septic • Bacterial • Mycobocterial • Lyme disease • Fungal B) Traumatic • Fracture • Internal derangement • Hemarthrosis C) Crystal deposition dis Gout Osteoarthritis CPPD Hydroxyapatite DD Calcium oxalate DD Palindromic rheumatism D) Others Juvenile RA (Pseudogout) Avascular N Foreign-body S Pigmented villonodular syno. Synovioma Coagulopathy Polyarticular diseases occasionally present with a monoarticular onset? • Rheumatoid arthritis • Reiter's syndrome/reactive arthritis • Juvenile rheumatoid arthritis • Psoriatic arthritis • Viral arthritis • Enteropathic arthritis • Sarcoid arthritis • Whipple's disease The most likely causes of chronic monoarthritis (inflammation within a single joint for > 6 weeks). INFLAMMATORY NON-INFLAMMATORY Inflammatory synovial fluid Mycobacterial infection Fungal infection Lyme arthritis Monoarticular presentation of RA Seronegauve spondyloarthropathies Sarcoid arthritis Foreign-body synovitis Structural abnormality Internal derangement Osteoarthritis Internal derangement of the knee Avascular necrosis of bone Pigmented villonodular synovitis Synovioma Causes of acute polyarthritis: Infection Other Inflammatory Gonococcal Meningococcal RA Polyarticular and syst JRA Polyarticular gout SLE Reiter's syndrome Psoriatic arthritis Sarcoid arthritis Lyme arthritis Acute rheumatic fever Bacterial endocarditis Viral (rubella, H BV & HCV, EBV& HIV) Causes of chronic polyarthritis: INFLAMMATORY • RA • Enteropathic arth • Polyarticular JRA • SLE * SSc • CPPD, Polyarticular gout • Polymyositis • Sarcoid arthritis • Reiter's syndrome • Vasculitis • Psoriatic arthritis • Polymyalgia Rh. NON-INFLAMMATORY OA Paget's disease CPPD Fibromyalgia Benign hypermobility syndrome Polyarticular gout Hemochromatosis Rheumatologic emergency • Acute monoarthritis = the joint is infected until proven otherwise. • The septic joint must be diagnosed quickly and managed aggressively to avoid permanent structural damage. History History taking from a patient with monoarthritis 1. Onset of pain: sudden, in seconds or minutes? (Consider fracture and internal derangement). 2. Over several hours or 1-2 days? (Consider infection, crystal deposition diseases, inflammatory arthritis and palindromic rheumatism). 3. Insidiously over days to weeks? (Consider indolent infections, such as mycobacteria and fungi, osteoarthritis, tumor, and infiltrative diseases). 4. Overused or damaged joint, either recently or in the past? (Consider traumatic causes). 5. History of IV drug abuse? Recent infection of any kind? (Consider septic arthritis). 6. Previous acute attacks of joint pain and swelling that resolved spontaneously? (Consider crystal deposition and other inflammatory arthritis). 7. Treatment with a prolonged course of corticosteroids? (Consider infection or osteonecrosis of bone). 8. Associated skin rash, low-back pain, diarrhea, urethral discharge, conjunctivitis, or mouth sores? (Consider Reiter's syndrome, psoriatic, or enteropathic arthritis). 9. History of a bleeding diathesis? treatment with anticoagulants? (Consider hemarthrosis). Is the age of the patient useful in the differential diagnosis? I- In children, consider: • Congenital dysplasia of the hip. • Slipped femoral epiphysism. • Monoarticular presentation of JRA. • Children are unlikely to have GOUT. II- In young adults, consider: • • • • • Seronegative spondyloarthropathy. RA. Internal derangement of the joint. They are less likely to have GOUT. A septic- joint is often due to gonococcal infection. III- Older adults : • • • • • Crystalline arthritis. OA. Osteonecrosis. Internal derangement of the joint. A septic joint in these individuals is less likely due to gonococcal organisms. • What are the most likely diagnoses in hospitalized patients with acute monoarthritis? • Acute monoarthritis: * Pyogenic infection * Acute crystal deposition diseases • Risk factors known to provoke gout or pseudogout: trauma, surgery, hemorrhage, infection or medical stress such as: CRF, MI & CVS. Polyarthritis • Pains differ: Polyarthritis = inflammation (swelling, tenderness, warmth) of > 4 joints by examination. Polyarthralgia = pain in > 4 joints without demonstrable inflammation; eg: SLE, systemic sclerosis, vasculitis, polymyalgia rheumatica, and chronic non-inflammatory. Diffuse aches and pains are poorly localized symptoms originating in joints, bones, muscles, or other soft tissues. Polymyalgia rheumatica, fibromyalgia, polymyositis, and hypothyroidism. Sequence of joint involvement: 1- Migratory (fleeting) polyarthritis: Symptoms disappear in the affected joints to reappear in others. Ex.: ARF, Gonococcal, Viral, early phase of Lyme. 2- Additive: Symptoms persist with addition of new joint inflammation Ex.: RA, SLE. 3- Intermittent: Attacks of remissions & exacerbations in the same joint. Ex.: Gout, sarcoid arthritis, Reiter's syndrome and psoriatic. What are the most likely diagnoses in women aged 25-50 who present with chronic polyarticular symptoms? OA. RA. SLE. Fibromyalgia. Benign hypemobility syndrome. What are the most likely diagnoses in men aged 25-50 who present with chronic oligoarticular or polyarticular symptoms? Gonococcal arthritis. Reiter Syndrome. Ankylosing Spondylitis. OA. Hemochromatosis. And in patients over age 50 presenting with chronic polyarticular symptoms? OA. RA. CPPD disease. Polymyalgia rheumatica. Paraneoplastic polyarthritis. Distribution of Joint Involvement Ex. Ex. Ex. Symmetrical Asymmetrical RA SLE Reiter PA AS Axial Peripheral AS PA (70% also affects IPJ--- sausage digits) Reiter RA SLE Large Small Seronegative Reiter ARF RA SLE JOINTS COMMONLY INVOLVED DISEASE JOINTS COMMONLY SPARED Gonococcal arthritis Knee, wrist, ankle, hand IP Axial Lyme arthritis Knee, shoulder, wrist, elbow Axial Rheumatoid arthritis Wrist, MCP, PIP, elbow, glenohumeral, cervical spine, hip, knee, ankle, tarsal, MTP DIP, thoracolumbar spine OA First CMC, DIP, PIP, cervical spine, thoraco-lumbar spine, hip, knee, first MTP, toe IP MCP, wrist, elbow, shoulder, ankle, tarsal Reiter's syndrome Knee, ankle, tarsal. MTP, toe IP, elbow, axial Psoriatic arthritis Knee, ankle, MTP. toe IP, wrist. MCP, hand IP. axial Enteropathic arthritis Knee, ankle, elbow, shoulder, MCP, PIP, wrist, axial Polyarticular gout First MTP, instep, heel, ankle, knee Axial CPPD disease Knee, wrist, shoulder, ankle, MCP, hand IP, hip, elbow Axial Sarcoid arthritis Ankle, knee Axial Heroochromatosis MCP, wrist, knee, Hip, feet, shoulder Extra-articular Organ Involvement: •ARF Ht, pleura •Viral A. Liver •SBE Ht valves & kidney •RA Lung, pl., ht. •SLE Lung, pl., ht., kidney, CNS •Scleroderma Lung, pl., ht., kid., GI., Liver •PM/DM Lung, pl., ht. •Reiter Valves, GI. •Enteropathic A: GI., Liver •Gout Kidney •Sarcoid A: Lung, Liver •Vasculitis Lung, Kidney • Hemochromatosis: Ht, liver, Pnc Morning stiffness Morning stiffness = time it takes for patients with polyarthritis to move after arising in the morning, or after rest. Site: Affecting hands in RA & back in AS. Inflammatory arthritis, morning stiffness lasts > I hour & tends to parallel the activity. Non-inflammatory, eg. OA, ---MS < 15 minutes. Examination Is Fever a useful sign? • • • • • • Misleading !! Infectious arthritis. Acute attacks of gout and CPPD disease. RA, juvenile RA. Sarcoidosis. Reiter's syndrome. • Skin – Nodules: RA, gout tophi – Rash: psoriasis, lupus, Still’s, viral etc • Inability to bear weight – Sepsis – Fracture – Crystal arthritis – Neurologic • Signs of inflammation – Synovitis (soft tissue swelling) – Local heat – Effusion • Range of motion – Active, N Passive: soft tissue eg bursitis, tendinitis, muscle – Active, Passive: contracture, synovitis, structural abnormality Investigations Monoarthritis • Synovial fluid analysis.: Most useful diagnostic study in the initial evaluation of monoarthritis Almost always indicated 1. Radiograph of the joint: may reveal: • Normal, OR unsuspected fracture, • Osteonecrosis, OA, or • Juxta-articular bone tumor. • Chondrocalcinosis, a radiologic feature of CPPD • Chronic fungal or mycobacterial infection. • Contralateral joint radiograph for comparison. 2. Complete blood count. • Leukocytosis + possibility of inf. Indicated in selected patients 1. Cultures of blood, urine: Mandatory in septic joint. 2. PT & PTT: when anticoagulation or coagulation disorder is suspected. 3. ESR, CRP: nonspecific; significant elevation = inflammation. Ask for further investigations in chronic cases: 4. Radiograph of sacroiliac joints: asymptomatic sacroiliitis in young males (spondyloarthropathy). 5) Chest radiograph: pulmonary TB or sarcoidosis. 6) Tuberculin test: negative test in excluding TB?. 7) Serologic tests: Lyme disease (Borrelia burgdorferi), RF, ANA, and HLA-B27. Polyarthritis • X-ray • • • • • • • • Laboratory testing CBC Serum uric acid THS Iron studies Liver enzymes Serum creatinine Urinalysis • ESR • ANA • RF • HLA-B27 antigen • Synovial fluid analysis Conclusion 1.Acute monoarthritis = joint aspiration to exclude septic & crystal- induced arthritis. 2.Chronic monoarthritis > 6 weeks of unknown cause needs synovial biopsy. 3.Gout does not occur in premenopausal females or in joints close to spine. Take your time for final diagnosis! • Because many chronic polyarticular diseases require months or years to diagnose, patience is often required. • Many diseases present insidiously with few objective findings for prolonged times. • Many diseases initially represent others before finally take their usual pattern. • RA, for example, can present as a monoarthritis before assuming its more typical polyarticular course. Take your time for final diagnosis! (cont.) • Characteristic laboratory abnormalities may require months or years to develop. • The joint symptoms precede the extraarticular features by months or years. • Joint radiographs may not show characteristic changes of the arthritis for months or years. Not all pts. with +ve RF=RA, nor +ve. ANA = SLE . Remember nothing is 100% 1 Musculoskeletal complaint History & Examination? Articular or non• Acute or chr.• Inflammatory or non.• Number & distribution• Articular? Non articular Fibromyalgia R Hypermobility S Acute or Chronic ? Acute<6 W. Acute arthritis: Infectious• Crystal-induced• Reiter’s• Presentation of Chr. Arth.• Chronic>6W. Inflammatory or non-infl. 2 Inflammatory or non-inflam. Chronic non-inflammatory arthritis Affects Wt. Br. J. (H & k), DIP, CMC Chronic inflammatory arthritis= MS>1hr, synovial swelling, warm, tender Joint, +syst. manifes., CRP, ESR 1=mono, 2-4=oligo arthritis: PA- RS- PJA >4 J = polyarthritis Symetrical _ + OA Osteonecrosis Charcot arthritis PA, RS PIP, MCP, MTP SLE, SSc, PM + RA THANK YOU