Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Radiation therapy wikipedia , lookup
Center for Radiological Research wikipedia , lookup
Backscatter X-ray wikipedia , lookup
Proton therapy wikipedia , lookup
Positron emission tomography wikipedia , lookup
Nuclear medicine wikipedia , lookup
Radiation burn wikipedia , lookup
Brachytherapy wikipedia , lookup
Radiosurgery wikipedia , lookup
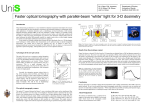
S Dr. S. J. Doran Department of Physics, University of Surrey, Guildford, GU2 7XH, UK High-resolution measurements of radiation dose in 3-D using gel dosimetry Simon J Doran Department of Physics University of Surrey Acknowledgements • Paul Jenneson, Mamdouh Bero, Nik Krstajic (Physics Dept., University of Surrey) • Phil Murphy, Mark McJury, Viv Cosgrove (RMH / ICR) • Mark Oldham (William Beaumont Hospital, Michigan) • Steve Hepworth (BNFL) • Dave Bonnet (Maidstone) Overview of Seminar • What is gel dosimetry? • Uses and application areas • Introduction to MRI and optical methods • Principal problems • Research areas • Report back from conference What is gel dosimetry and why do it? • • • • Conventional methods of dosimetry are either single point (e.g., TLD’s, ion chambers, etc.) or 2-D (film). Complex radiotherapy treatments (e.g., conformal therapy, brachytherapy, abutting fields) require 3-D measurements. Gel dosimetry is a way of achieving this in special test objects (phantoms) filled with a radiosensitive gel. Monte Carlo simulation is known to be capable of high accuracy … but … we still need experimental verification that delivery occurred as expected. Steps in a gel dosimetry experiment 1. Prepare heated gel and pour into container or anatomicallyshaped mould. Cool and solidify gel. 2. Irradiate with same protocol as for intended patient. 3. Image with desired modality (MRI, optical, ultrasound, CT, ...) MRI: original monomer has long T2, polymer has short T2. Optical: original monomer gel is transparent, polymer gel is cloudy. Ultrasound: acoustic properties of gel change with irradiation. Data from Maryanski et al. Med. Phys. 23(5) 699-705, 1996 Potential uses of gel dosimetry • Gel dosimetry is not a replacement for routine QA using ion chambers, etc. • Machine imperfections (e.g., leakage through MLC leaves) • Commissioning • Treatment verification • Accident prevention • Special procedures and “one offs” Application areas for gel dosimetry • Standard therapy with 3-D planning systems • Overlapping fields and match lines • Stereotactic radiotherapy • IMRT • Brachytherapy • Particle therapy (proton, electron, BNCT, etc.) Physical basis of measurement: (1) Fricke gels • Fricke solution Fricke and Hart, 1966: standard “absolute” dosimetry method Fe(NH4)2(SO4)2.6H2O(aq), HCl(aq), NaCl(aq) Effect of radiation: Fe2+ + h Fe3+ + e Originally detected via UV spectrophotometry • Detection by NMR Gore et al. 1984 T1 and T2 reduced by presence of Fe3+ • Fricke gel Numerous authors 1990-2001 Fricke solution mixed with gelatin to fix dose in space Physical basis: (2) Diffusion problem in Fricke gels • • The Fe3+(aq) that are used to record dose in a Fricke gel are not fixed securely enough by the gelatin. Diffusion occurs on a timescale of a few hours and causes a blurring of the dose profile. t=0 [Fe3+] t=0 t=1 hr t>0 x t=16 hr Physical basis of measurement: (3) Polymer gels • First proposed by Maryanski et al. in 1993 • Two monomers in a matrix of gelatin Monomers + h long T2 • Polymer short T2 Simple recipe with 4 constituents: Acrylamide N-N'-methylenebisacrylamide Gelatin Water 3% (by weight) 3% 5% 89% Physical basis: (4) Polymer gel mechanism 1. Creation of free radicals by the radiation H2O + h HO* + H* 2. Transfer of an OH* radical to one of the co-monomers Physical basis: (5) Polymer gel mechanism (cont.) 3. Extension of the chain by the encounter of a radical and a further monomer unit (either of the comonomers). A new longer chain radical is formed. * Physical basis: (6) Polymer gel mechanism (cont.) 4. Termination of the chain by the encounter of two radicals. At the end, a branched and cross-linked structure is formed. • • The polymerisation is limited spatially to a small region around the site of the incident radiation. The polymer fragment created is supported in a matrix of gelatin. Manufacture of polymer gels N2 N2 • The whole manufacturing process must take place in a sealed reaction vessel, or nitrogen-filled glove-box to avoid the slightest contact with air. • Preparation requires considerable experience as there are a number of problems that can lead to inconsistent results. Example of gel dosimetry in routine treatment • Visualisation of beam penumbra for a 4 4 cm2 field Target 2 treatment plan MRI result Results from the Royal Marsden team (M. McJury, M. Oldham, M.Leach, S. Webb), Phys. Med. Biol., 43, 1113-1132 (1998) Example of gel dosimetry in conformal therapy • Simulated nine-field prostate treatment using NOMOS MIMIC device Treatment Plan Target organ MR dose map Organs to spare Results from the Royal Marsden team (M. McJury, M. Oldham, M.Leach, S. Webb), Phys. Med. Biol., 43, 1113-1132 (1998) Gel dosimetry in brachytherapy • No other methods are available for measuring the dose distributions close to a brachytherapy source. Data: M Maryanski, Ir-192 seed Y de Deene et al. PMB 46, 2801 (2001) Gel dosimetry in vascular brachytherapy • No other methods are available for measuring the dose distributions close to a brachytherapy source. Data: Bonnett et al. DOSGEL 2001 Why look for another method? • Although MR imaging of the gel can work very well, there are a number of problems precluding a wide uptake: MRI is expensive and cannot currently be used routinely for radiotherapy QA and planning. MRI is relatively slow if you really need true 3-D data. The polymer gel is difficult to make reproducibly. Contamination by oxygen causes the polymer gel to fail. Absolute dosimetry is difficult. Measurements are temperature and time dependent. What is optical computed tomography (OCT)? • As its name suggests, OCT relies on the detection of radiation in the visible region, rather than X-rays. • • The principles are exactly the same as X-ray CT. However, the properties of visible light lead to a number of advantages and disadvantages: No ionising radiation Equipment is cheap and off-the-shelf (total cost < £10,000) We can use optics to manipulate the beam Extremely limited range of samples due to strong absorption and scatter Problems of reflection and refraction to contend with A reminder about X-ray CT • • • We are all used to the idea of X-ray CT. X-rays emitted by the source are attenuated to varying degrees by the sample (patient). At each detector a signal is detected that is proportional to • • e ( x ) dx . Together the signals from all the detectors form a projection. Acquisition of a number of projections as the detector rotates gives a complete dataset, from which the image is computed by back-projection. Physical basis for OCT: (1) Colour-change gel • • Take a standard Fricke gelatin gel and add a metal-ion indicator sensitive to Fe3+. Gel changes colour from orange to purple on irradiation. Attenuation primarily by absorption 1 Change in optical absorbance / cm--1 / cm absorbance) D(optical • 0.4 FXG spectral dose-response 0.2 0.0 -0.2 350 400 450 500 550 600 650 700 Wavelength / nm Wavelength / nm Appearance of gel post-irradiation Dose response of gel, with mercury spectrum inset Physical basis for OCT: (2) Polymer gel • • Polymer gels attenuate light primarily by scattering. Above 500 nm, response to dose is approximately linear. Data: M Maryanski, Ir-192 seed Data: M Maryanski et al. Phys. Med. Biol. 41, 2705 (1996) Physical basis for OCT: (3) PRESAGE • • PRESAGE is not a gel but a solid polyurethane. Active ingredient is a “leuco dye”. Data: J Adamovics, Heuris Pharma • Attenuation occurs primarily by absorption and is currently optimised for use with a He-Ne laser (max absorption at 632 nm) OCT: Historical perspective • Colour-change gels introduced in 1991 (Appleby and Leghrouz, Med. Phys. 18, 309-312, 1991) • “Pencil-beam”, laser-based systems Typically one plane in ~15 mins. (Tarte et al. Unpublished Gore et al. Phys. Med. Biol. 41, 2695-2704, 1996; Kelly et al. Med. Phys. 25(9), 1741-1750, 1998) • 2-D imaging of radiation dose with CCD (Tarte et al. Med. Phys. 24(9), 1521-1525, 1997) • Imaging of stacked gels (Gambarini et al. DOSGEL ’99) • First CCD tomography scanners (Wolodzko et al., Bero et al., DOSGEL ’99) Typically 512 planes in ~30 mins., possibly faster still Two flavours of optical tomography • Single-beam tomography (Gore, Maryanski et al., 1996) Other workers in the field: Oldham et al. (Michigan) Jordan et al. (London, Ontario) • Parallel-beam tomography (Bero, Doran et al., 1999) Other workers in the field: Wolodzko, Appleby et al. (New Jersey) Jordan et al. (London, Ontario) Single beam laser scanning of phantom (1) • • • • Single laser beam moves across sample in n steps to give a 1-D projection. Sample rotates by angle 180/nproj. Nproj projections are acquired and reconstructed by filtered back-projection. Scan time typically 15 mins per 2-D slice Data: Oldham et al. Med. Phys. 30 (4), 623 (2003) Single beam laser scanning of phantom (2) Phantom using clear gelatin and food colouring Reconstructed plane Demonstration of accuracy of image attenuation values Data: Oldham et al. Med. Phys. 30 (4), 623 (2003) CCD optical CT scanning (1) • • • • Parallel light beam shines through the sample. 2-D projection is captured in a single shot Sample is rotated by 180/nproj and procedure repeated. nproj projections are acquired and reconstructed by filtered back-projection. Scan time typically 15 mins per 3-D volume CCD optical CT scanning (2): Potential speed • • Frame-grabber captures 1 frame (768 x 576 pixels) in 50 ms. Suppose we took ~800 projections (Nyquist requirement) whilst continually rotating phantom through 1 revolution. • We could then potentially acquire a 5123 dataset with data acquired in 40 s! • Compare MRI T2 map — up to, say, 5 x 256 x 256 in about 4 minutes. However … we are not there yet!! CCD optical CT scanning (3): Phantom Data sinogram Single 2-D slice from tomography dataset 3-D reconstruction CCD optical CT scanning (4): Irradiated gel X-ray tube 10 Gy 57 mm 0 Gy Schematic 3-D visualisation of the beam pattern Single slice from tomography dataset Pros and cons of different gels for optical imaging • Fricke gels Easy to make; not oxygen sensitive Attenuation by absorption so fast CCD t=0 t=16 hr tomography possible 10 Polymer gels No diffusion Attenuation by scattering, so must use slow laser tomography • 0 hr after irradiation 1 hr after irradiation Diffusion simulation 8 Dose / Gy • Diffusion is a major issue 6 4 2 0 Tricky to make PRESAGE polyurethane Cheap and easy to make; robust solid Attenuation by absorption Very stable and no diffusion -10 0 Distance / mm 10 Raman Spectroscopy Data: Baldock et al. DOSGEL 2001 Ultrasound Measurements Data: Mather et al. DOSGEL 2001 MAGIC gels insensitive to oxygen Data: Fong and Gore DOSGEL 2001 Xenon spectroscopy of polymer gels Data: Gore et al. DOSGEL 2001 Conclusions (1) • • • Gel dosimetry has an important role to play in radiotherapy. A number of clear functions of gel dosimetry have been established and 3-D application areas identified. That role is currently limited for a number of reasons: Technical difficulties with the method Lack of absolute dosimetry Difficulty in preparing polymer gels reproducibly Expense of MRI readout Lack of support from a major RT company • At the last major conference (DOSGEL 2001) no clear consensus at conference about when the technique will become routine in clinics. Conclusions (2) • • The best method of radiation dose mapping in 3D that we currently have is polymer gel MRI. However, this technique has a number of long-term problems that will slow its uptake: High cost of equipment Difficulties with gel manufacture High degree of expertise needed • • Optical computed tomography is currently where MRI dose mapping was 5-10 years ago, but demonstrates a number of promising features. Other imaging modalities, such as ultrasound, show some promise, but require much further development. Conclusions (3) • The currently active research areas in this field are: Understanding in detail how the gels work physical chemistry Development of polymer gel that is not spoiled by oxygen Assessment of the quality of the results obtained via MRI (Current consensus is ~ 3%) Development of new types of gel Development of new imaging modalities Opening up new application areas • Finally … the gel dosimetry community is currently very small. Less than 50 people made the trip to Brisbane for DOSGEL 2001. • So … there are lots of opportunities to do exciting research in this new field.