Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Jatene procedure wikipedia , lookup
Electrocardiography wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
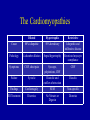
Cardiovascular Board Review II Sohan Parekh, MD Department of Emergency Medicine Mount Sinai School of Medicine Question 1 Regarding treatment of heart failure in patients with diastolic rather than systolic dysfunction: A. B. C. D. E. Aggressive therapy with diuretics is more effective b-Blocking agents might improve cardiac output Both are associated with impaired cardiac contractility Most patients with CHF have diastolic dysfunction Ventricular filling pressures are higher in systolic dysfunction than in diastolic dysfunction PEER VII 268 Q1 Answer Regarding treatment of heart failure in patients with diastolic rather than systolic dysfunction: A. B. C. D. E. Aggressive therapy with diuretics is more effective b-Blocking agents might improve cardiac output Both are associated with impaired cardiac contractility Most patients with CHF have diastolic dysfunction Ventricular filling pressures are higher in systolic dysfunction than in diastolic dysfunction Heart Failure Syndromes • Systolic dysfunction – EF < 40% – Decreased contractility due to ischemic heart disease – Intolerant to high afterload • Diastolic dysfunction – Preserved contractility, EF normal or increased – Impaired relaxation and diastolic filling – Due to long-standing hypertension – Intolerant to tachycardia which reduces filling time Heart Failure Syndromes • Left Heart Failure – DOE, orthopnea, PND – Cough with pink, frothy sputum – Rales on lung exam – CXR: pulmonary edema, cephalization, Kerley B lines • Right Heart Failure – Less common than left heart failure – Cause include left heart failure, pHTN, PE – Anasarca, Hepatomegaly, Ascites Question 2 A 30 yo M with a history of prior episode of tachycardia presents with palpitations. His pulse is 170, and blood pressure is 100/50. The EKG reveals the rhythm depicted in EKG below. PEER VII 142 Q2 (continued) Q2 (continued) Which of the following treatments would terminate the tachycardia most rapidly? A. B. C. D. E. Adenosine 6 mg IV rapid bolus Amiodarone 150 mg IV over 10 minutes Diltiazem 15 mg IV slow push Lidocaine 75 mg IV slow push Procainaminde 1000 mg over 20 minutes Q2 Answer Which of the following treatments would terminate the tachycardia most rapidly? A. B. C. D. E. Adenosine 6 mg IV rapid bolus Amiodarone 150 mg IV over 10 minutes Diltiazem 15 mg IV slow push Lidocaine 75 mg IV slow push Procainaminde 1000 mg over 20 minutes Post adenosine Supraventricular Tachycardia • Regular rhythm • Originates above bifurcation of His bundle • Palpitations, chest pain, syncope, APE • Treatment approach based on hemodynamic stability & QRS morphology – If wide-complex: treat as VT – If unstable: synchronized cardioversion Supraventricular Tachycardia • Stable SVT – Vagal Manuevers: carotid massage, diving reflex, Valsalva manuever – Adenosine 6 12 12 ( 18?) – Diltiazem, Esmolol, Digoxin – Amiodarone • If known SVT with normal lytes and return to baseline, can be discharged Question 3 Which of the following statements comparing dilated cardiomyopathy and hypertrophic cardiomyopathy is correct? PEER VII 335 Q3 (continued) A. Both are improved by digitalis and nitrate therapy B. Both involve four-chamber heart enlargement C. Dilated cardiomyopathy is a more common cause of sudden death in young patients D. Dilated cardiomyopathy is associated with diastolic dysfunction E. Most cases of hypertrophic cardiomyopathy are hereditary Q3 Answer A. Both are improved by digitalis and nitrate therapy B. Both involve four-chamber heart enlargement C. Dilated cardiomyopathy is a more common cause of sudden death in young patients D. Dilated cardiomyopathy is associated with diastolic dysfunction E. Most cases of hypertrophic cardiomyopathy are hereditary The Cardiomyopathies • Dilated cardiomyopathy – 80% idiopathic – Dilation and hypertrophy of myocardium resulting in decreased cardiac output – Pump failure results in CHF, syncope, DOE – Stagnant blood flow in LV can results in mural thrombi with resultant embolic complications – ECG shows LVH; CXR shows cardiomegaly and CHF – Treatment with diuretics and nitrates acutely – Long term ACE-I and b-blockers decrease mortality The Cardiomyopathies • Hypertropic (aka HCM, HOCM, IHSS) – 50% of cases are hereditary – Hypertrophy of the intraventricular septum without ventricular dilation – CO is normal, diastolic filling is impaired – Symptoms: DOE, palpitations, chest pain – SEM which increases with Valsalva – ECG shows LVH only 30%; CXR negative – Outflow obstruction worse with exertion, nitrates, dig The Cardiomyopathies • Restrictive – Decreased diastolic volume of both ventricles – Uncommon, often idiopathic – Infiltrative disease – Symptoms: CHF. Chest pain uncommon – CXR: CHF without cardiomegaly – ED treatment is symptomatic for CHF and/or underlying disease The Cardiomyopathies Dilated Hypertrophic Restrictive Cause 80% idiopathic 50% hereditary Idiopathic and infiltrative disease Pathology 4-chamber dilation Septal hypertrophy Restricted myocyte compliance Symptoms CHF, chest pain Syncope, palpitations, CHF CHF Failure Systolic Diastolic and outflow obstruction Diasolic Findings Cardiomegaly SEM Non-specific ED Treatment Diuretics No Nitrates or Digoxin Diuretics Question 4 A 51 yo M with a history of HTN and ERSD presents with chest heaviness and SOB. Vital signs are blood pressure 95/80, HR 135, RR 18, and temperature 36.7oC. Exam reveals JVD, bibasilar inspiratory crackles, distant heart sounds, and pitting peripheral edema. CXR demonstrates cardiomegaly with mild bilateral pulmonary vascular congestion. The rhythm strip is shown below. PEER VII 38 Q4 (continued) Which of the following is the most appropriate therapy? Q4 (continued) A. Blood cultures x 2, broad-spectrum antibiotics, and dopamine infusion at 10 units/kg/min B. Calcium gluconate IV, insulin 10 units IV, detrose 50 g IV, and arrange for emergent dialysis C. Diltiazem 20 mg IV bolus, followed by drip at 5 mg/hr D. Heparin 5000 units IV bolus, followed by synchronous cardioversion at 75J E. Normal saline 500 mL IV bolus, and emergent pericardiocentesis Q4 Answer A. Blood cultures x 2, broad-spectrum antibiotics, and dopamine infusion at 10 units/kg/min B. Calcium gluconate IV, insulin 10 units IV, detrose 50 g IV, and arrange for emergent dialysis C. Diltiazem 20 mg IV bolus, followed by drip at 5 mg/hr D. Heparin 5000 units IV bolus, followed by synchronous cardioversion at 75J E. Normal saline 500 mL IV bolus, and emergent pericardiocentesis Cardiac Tamponade • Pericardial effusion compressing RV causing impaired filling and decreased cardiac output • Effusion can be medical or traumatic – Medical: usually chronic and large volume – Traumatic: small volume (< 100 cc) • Causes: uremia, cancer, infectious, SLE Cardiac Tamponade • Findings – Beck’s triad • Hypotension • Distended neck veins • Muffled heart tones – Narrow pulse pressure – Pulsus Parodoxus • EKG: low voltage, electrical alternans (20 %) Cardiac Tamponade • CXR: +/- enlarged cardiac silhouette (“water-bottle”) • Treatment – IVF trial – Pericardiocentesis Question 5 Which of the following statements regarding cocaine-associated chest pain is correct? A. B. C. D. E. Cardiac markers are often unreliable in patient with cocaineassociated MI Aspirin and b-blockers are indicated A minority of patients with cocaine-associated MI have evidence of underlying coronary artery disease Palpitations and tachycardia are the most commonly associated symptoms The average time from cocaine use to the presentation of the patient in the ED is 2 hours PEER VII 381 Q5 Answer Which of the following statements regarding cocaine-associated chest pain is correct? A. B. C. D. E. Cardiac markers are often unreliable in patient with cocaineassociated MI Aspirin and b-blockers are indicated A minority of patients with cocaine-associated MI have evidence of underlying coronary artery disease Palpitations and tachycardia are the most commonly associated symptoms The average time from cocaine use to the presentation of the patient in the ED is 2 hours Cocaine Chest Pain • Causes arterial vasoconstriction, sympathetic surge, and increased platelet aggregation • Greatest risk from cocaine use is in the first hour • Patients present with chest pain, tachycardia, HTN • Workup: EKG, serial cardiac enzymes Cocaine Chest Pain • Treatment – – – – Benzodiazepines are the mainstay of treatment ASA can be given Chest pain should be controlled with NTG Blood pressure control can be achieved with direct a-blockade or Ca-channel blocker – b-blockers absolutely contraindicated Cocaine Chest Pain • Dispo – If they make enzymes, admit – If older with other risk factors, consider stress – If young, discharge with Rx for cocaine and metoprolol Question 6 In the treatment of hyperkalemia-induced cardiac arrest, which of the following treatment modalitites provides the most rapid reduction in serum potassium levels? A. B. C. D. E. Calcium gluconate Insulin Magnesium sulfate Sodium bicarbonate Sodium polystyrene sulfonate PEER VII 143 Q6 Answer In the treatment of hyperkalemia-induced cardiac arrest, which of the following treatment modalitites provides the most rapid reduction in serum potassium levels? A. B. C. D. E. Calcium gluconate Insulin Magnesium sulfate Sodium bicarbonate Sodium polystyrene sulfonate Hyperkalemia • EKG changes – – – – Peaked T waves PR prolongation QRS prolongation, P wave flattening Loss of P wave, QRS prolongation to sine wave Webster, et al. Recognising signs of danger. Emerg. Med. J., Jan 2002; 19: 74 – 77. Hyperkalemia http://sprojects.mmi.mcgill.ca/heart/ecgk1.html http://urbanhealth.udmercy.edu/ekg/pdf/hyperkalemia.pdf Hyperkalemia • Treatment – – – – – – Calcium chloride or gluconate Dextrose + Insulin (onset: 20 min, duration: 1 hr) Bicarbonate (onset: 10 min, duration: 2 hr) Lasix Albuterol Kayexalate (onset: 2 hr) Question 7 Which of the following is true concerning the rhythm in the EKG below? PEER V Q7 (continued) A. Is a benign rhythm with low mortality B. Overdrive pacing is an effective treatment C. Occurs in patients with shortened QT interval D. Responds to IV calcium E. Procainamide is first-line therapy Q7 Answer A. Is a benign rhythm with low mortality B. Overdrive pacing is an effective treatment C. Occurs in patients with shortened QT interval D. Responds to IV calcium E. Procainamide is first-line therapy Torsades de Pointes • Polymorphic V-tach • Can degenerate into Vfib • Underlying long-QT (QTc > 460 ms) – Drug-induced (Haldol, TCAs, procainamide) – Congenital prolonged QT syndrome • Treatment – Magnesium IV – Overdrive pacing – Cardioversion if unstable Question 8 Which of the following statements regarding posterior wall infarction is correct? A. B. C. D. E. Associated with ST-segment depression in V1 ECG shows an inverted T wave in V1 ECG shows large S waves in V1 Occurs in 5% of all acute MIs Results from occlusion of the LAD PEER VII 249 Q8 Answer Which of the following statements regarding posterior wall infarction is correct? A. B. C. D. E. Associated with ST-segment depression in V1 ECG shows an inverted T wave in V1 ECG shows large S waves in V1 Occurs in 5% of all acute MIs Results from occlusion of the LAD STEMI • Complete occlusion of coronary artery • ECG with characteristic ST elevations • ASA +/- b-blocker • PCI vs Thrombolytics STEMI • Posterior Wall MI – ST depression, R:S ratio > 1 in V1 to V2 http://emj.bmj.com/cgi/content/abstract/19/2/129?ck=nck STEMI • Anterior Wall MI – ST elevations in V2-V4 – Reciprocal ST depressions in II, III, aVF http://urbanhealth.udmercy.edu/ekg/pdf/acuteAnterWallMI.pdf STEMI • Inferior Wall MI – ST elevations in II, III, aVF – Must obtain Right-sided EKG http://www.lf2.cuni.cz/Projekty/interna/heart_sounds/ekg4/ekg12.jpg STEMI • Lateral Wall MI – ST elevations in I, aVL, V5, V6 http://sprojects.mmi.mcgill.ca/heart/ecg9805316.html Question 9 Which of the following is most commonly seen in infants with congestive heart failure? A. B. C. D. E. Bilateral pedal edema Bounding femoral pulses Excessive weight gain Jugular venous distention Sweating with eating PEER VII 376 Q9 Answer Which of the following is most commonly seen in infants with congestive heart failure? A. B. C. D. E. Bilateral pedal edema Bounding femoral pulses Excessive weight gain Jugular venous distention Sweating with eating Infant CHF • CHF results from left-to-right shunting – VSD – PDA – Coarctation of the Aorta • Symptoms – Poor feeding with sweating during feeds – Poor growth and weight gain – Weak cry; Coughing and wheezing Infant CHF • Findings – Weak peripheral pulses – Rales • EKG: possible SVT, otherwise non-specific • CXR – Cloudy lung files – Cardiomegaly Question 10 A 45 yo F s/p heart transplant five years ago, presents to the ED with a 2d of SOB, and nonproductive cough. She is on immunosuppressant therapy. VS include BP 98/60, HR 130, RR 22, T 37.9 0C, and SaO2 95%. The physical exam is unremarkable except for scattered basilar rales. CXR shows cephalization, interstitial infiltrates, a slightly enlarged heart, and no effusions. EKG shows sinus tachycardia. Q10 (continued) Which study is indicated next, as part of an appropriate ED evaluation of this patient? A. B. C. D. E. Blood cultures, then start empiric antibiotics V/Q Scan Serum cardiac markers Cardiac MRI TEE Q10 Answer Which study is indicated next, as part of an appropriate ED evaluation of this patient? A. B. C. D. E. Blood cultures, then start empiric antibiotics V/Q Scan Serum cardiac markers Cardiac MRI TEE Heart Transplant • Post-transplant physiology – Heart is denervated – Both recipient and donor sinus nodes are functional thus 2 sets of P waves Circulation. 2007 Jan 23;115(3):e41-2 Heart Transplant • Ischemia of graft difficult to detect – Patients with CHF, SOB must have serial CE • Rejection – Mostly asymptomatic but can have dysrhythmia – Dose with steroids • Dysrhythmias – Bradycardia: isoproterenol (atropine doesn’t work) – Trachycardia: Standard resuscitation measures Question 11 What is the most effective medication to lower blood pressure in a patient with an acute aortic dissection? A. Fentanyl B. Labetalol C. Metoprolol D. Nitroglycerin E. Sodium Nitroprusside PEER VII Q331 Q11 Answer What is the most effective medication to lower blood pressure in a patient with an acute aortic dissection? A. Fentanyl B. Labetalol C. Metoprolol D. Nitroglycerin E. Sodium Nitroprusside Aortic Dissection • Violation of intima of aorta resulting in false lumen • Bimodal distribution – Young patients with connective tissue disease – Older patients with hypertension • Clinical presentation – Abrupt onset of tearing chest pain or back pain – Neurologic symptoms are common Aortic Dissection • Diagnosis – CXR: Abnomal in 90% of cases • Wide mediastinum • Abnormal aortic contour • Pleural effusion – CT-A with IV contrast or aortogram if stable for transport – Bedside TEE Aortic Dissection • Disposition depends on type – Type A (ascending): surgery – Type B (descending): medical mangement • Treatment – Must control the shear force on the intimal flap – b-blocker to decrease pulse – Anti-hypertensive to decrease BP • Sodium nitroprusside, fenoldopam, nicardipine Question 12 A 74 yo F presents by ambulance after she passed our at church. She is awake and alert but says she feels dizzy. VS include BP 80/50, HR 41, and temperature 36.8oC, O2 sat 99% on 3L. Cardiac monitoring reveals the rhythm depicted below. PEER VII Q331 Q12 (continued) Administration of atropine 1 mg IV has no effect on her blood pressure or heart rate. The next step should be: A. B. C. D. E. Dopamine infusion at 20 mcg/kg/min Epinephrine 1 mg IV slow push Stat cardiology consultation Transcutaneous cardiac pacing Transvenous cardiac pacing Q12 Answer Administration of atropine 1 mg IV has no effect on her blood pressure or heart rate. The next step should be: A. B. C. D. E. Dopamine infusion at 20 mcg/kg/min Epinephrine 1 mg IV slow push Stat cardiology consultation Transcutaneous cardiac pacing Transvenous cardiac pacing AV Nodal Blocks • Caused by conduction delay in AV node • First-Degree – PR interval > 0.2s (200ms) – All P waves followed by QRS – No intervention required http://urbanhealth.udmercy.edu/ekg/pdf/AVBlocks.pdf AV Nodal Blocks • Second-Degree Mobitz I (Wenckebach) – Progressive lengthening of PR interval followed by dropped beat – Seen in MI, digoxin toxicity, myocarditis, CAD – Stable rhythm http://urbanhealth.udmercy.edu/ekg/pdf/AVBlocks.pdf AV Nodal Blocks • Second-Degree Mobitz Type II – Fixed-length PR interval with one or more nonconducted beats – Signifies major damage to conduction system – Unstable: Requires permanent pacemaker AV Nodal Blocks • Third-Degree (Complete) Heart Block – No P waves are conducted through AV node – Junctional or Ventricular escape paces the heart – Unstable: Requires permanent pacemaker http://urbanhealth.udmercy.edu/ekg/pdf/AVBlocks.pdf Question 13 A 28 yo M presents with a laceration to the left forearm. The patient is in good health and has no other complaints. At triage the patient's blood pressure was noted to be 155/94 mmHg; the remainder of his vital signs are normal. Following repair of the laceration, the patient's blood pressure is rechecked and is unchanged. Q13 (continued) What is the best approach to this patient's elevated blood pressure? A. Administer labetalol or nifedipine with observation until SBP is < 140 B. Evaluate for end-organ damage with CXR, ECG, electrolytes, BUN/Cr and UA C. Instruct the patient to follow-up with his private physician within two months for recheck D. No further management required E. Admit for blood pressure control and workup Q13 Answer What is the best approach to this patient's elevated blood pressure? A. Administer labetalol or nifedipine with observation until SBP is < 140 B. Evaluate for end-organ damage with CXR, ECG, electrolytes, BUN/Cr and UA C. Instruct the patient to follow-up with his private physician within two months for recheck D. No further management required E. Admit for blood pressure control and workup Hypertension • Classifications – Emergency: Elevated blood pressure with associated end-organ dysfunction – Urgency: Elevated blood pressure with risk of imminent target organ dysfunction – Essential hypertension: SPB > 140 or DBP >90 Hypertension • Only HTN emergencies require immediate treatment – Labetalol – Nitroprusside – Fenoldopam – Nicardipine • For HTN urgencies, goal is reduction of blood pressure in the next 24-48 hours • For non-urgent blood pressure elevation, refer for timely follow up Question 14 A 7 wk old full-term M is brought in 45 minutes after having a 60-second episode of unresponsiveness and cyanosis. He remained pale and limp for 20 minutes and refused to feed. Cardiac exam reveals a pulse of 160, a harsh pansystolic ejection murmur and the LSB, and a single second heart sound. O2 sat is 84%. PEER VI Q14 (continued) What is the most likely diagnosis? A. B. C. D. E. Coarctation of the Aorta Hypoplastic left heart syndrome Patent ductus arteriosus Tetrology of Fallot Transposition of the great vessels Q14 (continued) What is the most likely diagnosis? A. B. C. D. E. Coarctation of the Aorta Hypoplastic left heart syndrome Patent ductus arteriosus Tetrology of Fallot Transposition of the great vessels Cyanotic Congenital Disease • Due to anatomic shunt with mixing of oxygenated and deoxygenated blood • The 5 Ts – Tetrology of Fallot – Truncus Ateriosus – Transposition of the Great Arerties – Tricuspid Atresia – Total Anomalous Venous Return Cyanotic Congenital Disease • Tetrology of Fallot – VSD, overriding aorta, RV obstruction, RVH – Tet spells: episodic SOB triggered by crying, eating, or playing – Tachypnea cyanosis seizures shock – O2, Position in knee-chest position • For severe shock within the first 2 weeks of life, possible closure of PDA – Prostaglandin E1 Question 15 Concerning the treatment of acute decompensated heart failure with nesiritide, which of the new following statements is most accurate? PEER VII Q379 Q15 (continued) A. In controlled trials, nesiritide administration resulted in better hemodynamic improvements than placebo B. Nesiritide does not affect renal function in patients with acutely decompensated heart failure C. Nesiritide has demonstrated clear superiority to conventional vasodilator and diuretic based therapy D. The hemodynamic effects of nesiritide include vasoconstriction of the veins and arteries, including the coronary arteries E. The use of nesiritide is clearly associated with an increased death rate at 30 days Q15 (continued) A. In controlled trials, nesiritide administration resulted in better hemodynamic improvements than placebo B. Nesiritide does not affect renal function in patients with acutely decompensated heart failure C. Nesiritide has demonstrated clear superiority to conventional vasodilator and diuretic based therapy D. The hemodynamic effects of nesiritide include vasoconstriction of the veins and arteries, including the coronary arteries E. The use of nesiritide is clearly associated with an increased death rate at 30 days CHF and Cardiogenic Shock • Acute pulmonary edema – Oxygen – Nitro (SL and IV) – Non-invasive ventilation • CHF – Diuretics – Afterload reduction (blood pressure control) CHF and Cardiogenic Shock • Nesiritide – Endogenous BNP counteracting renin system – Dilation of arterial and venous systems with increase in SV and CO versus placebo – Increased mortality and worsening renal failure – Don’t use this in the ED CHF and Cardiogenic Shock • Cardiogenic shock – Pump failure resulting in inadequate tissue perfusion – Most often secondary of massive acute MI – Also consider acute valvular disease or severe decompensated heart failure – Evidence of volume overload with poor perfusion (hypotension, cool, mottled skin) – Treatment focused on correcting poor perfusion CHF and Cardiogenic Shock • Cardiogenic shock treatment – – – – – Fluid challenge if no pulmonary edema Vasopressors: Dopamine or norepinephrine Inotropy: Dobutamine Phosphdiesterase inhibitors: Milrinone Find / steal / create a CCU bed immediately