Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
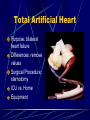
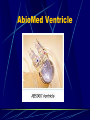
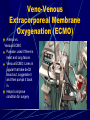
Rejection Normal response Inflammation 25% of pt. will have acute rejection during the first year post transplant Causes: Previous Rejection Noncompliance High cholesterol 3 Kinds of Rejection Hyper-acute: happens immediately Acute: within 1 month of transplant Chronic: all pts have this Likely sources of rejection: 0-1 Month IV line infection Urinary tract infection Wound infection Pneumonia Human herpes simplex virus Outcomes – Heart Transplant Hospital LOS Typical 15 Long Term Survival 3mo: 93% 1yr: 88% 5yr: 76% 10yr: 54%, can go 20+ years Outcomes – Lung Transplant Hospital LOS 1-3 weeks Long Term Survival 3mo: 91% 1yr: 80% 5yr: 51% 10yr: 21% Morbidity and Mortality Most common causes of death in patient’s with transplant are infection and rejection Most common complications for these patient’s are CVA, kidney failure, development of DM, muscle atrophy Physical Therapy Goals Airway Clearance Patient Function Patient Education Strengthening HEP Aerobic Training HEP Pacing, self-monitoring, targeting exercise, progression of HEP Discharge Plans Mechanical Assist Devices Cardiac Ventricular Assist Device Total Artificial Heart Respiratory Venous-Venous Extracorporeal membrane oxygenation (ECMO) Cardiac and Respiratory Venous-Arterial Extracorporeal membrane oxygenation (ECMO) Ventricular Assist Devices • What is it? • Purpose • Placement: L side • Attachments • Equipment: pump implanted in body, runs a long cord to keep infection away. Ventricular Assist Devices LVAD: RVAD: temporarily BiVAD: not good success Total Artificial Heart: bilateral heart failure Purpose Temporary: usually because of complications or younger patients. Long Term Bridge to Transplant Bridge to Explant: wean off VAD Destination Ventricular Assist Devices – History Technological Advances Ventricular Assist Devices – Types Types Pneumatic Axial Flow: screw that spins fastly Heartmate 2 • Continuous Flow • Significantly decreased pulse pressure • Anticoagulation • Hemolysis • “Vitals” • Flow: set rate • Speed • Power • Pulsatility Index Ventricular Assist Devices – Types Types Pneumatic Axial Flow Centrifugal Flow HeartWare Jarvik 2000 Total Artificial Heart Purpose: bilateral heart failure Differences: remove values Surgical Procedure: sternotomy ICU vs. Home Equipment Total Artificial Heart Ventricular Assist Devices Operative Procedure Median Sternotomy Benefits: able to be on wait list longer Risks: infection, clotting, bleeding, cognitive changes. Lifestyle changes: 24 hour supervision: trained with VAD emergency. Stay away from water Restriction on recreation and exercise Restriction for static electricity Necessary equipment: back-up power in <5min. Temporary / External VADS Purpose Types AbioMed Blood Pump 5000 Ventricles CentriMag Stay in ICU Functional Limitations AbioMed Ventricle CentriMag Patient Video: CentriMag and Heartmate II Veno-Venous Extracorporeal Membrane Oxygenation (ECMO) Arterial vs. Venous ECMO Purpose: used if there is heart and lung failure. Venous ECMO: Lines in jugular that take deO2 blood out, oxygenate it and then pumps it back in. Helps to improve condition for surgery Patient Video: VVECMO Implications For PT Physiology of LVAD Preload and afterload dependent BP (with axial or centrifugal flow) appropriate target for exercise intensity Arrhythmias AICD Lab Values-HgB/Antibodies Equipment Emergency Procedures Post-Operative Course Post Transplant Or VAD ICU Course Multiple chest tubes, IV lines, A-line, swanganz, catheter, pulse ox, SCDs, telemetry Delayed sternal closure Intubated/Sedated PT POD #1 Focus on Early Mobility: winkleman “bed rest in hell and critical illness, a body systems approach” Early Post-Op Course Day 1 common problem list Impaired airway clearance Decreased chest wall mobility Decreased functional mobility Decreased ROM and strength Limited knowledge of post-surgical precautions Other considerations Pressure relief / skin care Edema management Early Post-Op Course Day 1 common treatment activities Airway clearance Breathing exercises Chest wall mobility Positioning for postural drainage and edema management Shoulder exercises Bed mobility Transfer to chair Initiate patient/family education Discharge planning Early Post-Op Course Day 2-3 Continues in ICU usually PA catheter and A-line are taken out Continue with day 1 treatment activities adjust and progress as necessary Progress ambulation Early Post-Op Course Day 4-14: Moves out of ICU Teach independent airway clearance Progress mobility/activity Begin stair climbing Nu-Step or treadmill training Aerobic home exercise program Strengthening home exercise program Functional Outcome Measures Complete patient/family education For patients s/p transplant or LVAD: Issues Regarding Discharge Home Significant medication regime and side effects Frequent lab, procedure and MD appointments Changes in physical appearance/return to intimacy Depression and mood disorders Stress on finances and social support system Outpatient Treatment Options Outpatient Cardiac Rehabilitation VADs not covered Outpatient Pulmonary Rehabilitation Outpatient PT (for VADs - comfort level of therapists?) Subacute rehab, acute rehab, etc.