Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
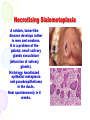
Diseases of the Salivary Glands Salivary glands and Saliva There are a lot of salivary gland diseases, to bo treated only surgically (ex.. cysts and salivary gland stones). The dentist must know the anatomy and physiology of the salivary glands. The saliva It is a secretum of exocrine glands, needs for the integrity of the oro-facila tissues. Saliva is a complex solution having protecting function. Phisical features of the saliva Parotid gland produce serous, the sublingual gland mucinous and the submandibular produce mixed saliva. Decrease in the quantity cause clinical and social problems for the patients. The main part of amylase are produced by the parotid gland, the blood group antigens by the small salivary glands. Salivary glands The biggest Parotid is arrow-headed, behind of the ramus mandibulae, innervate by the facial nerve. The saliva through the Stenon duct running in front of the masseter muscle get into the mouth. Its lead into the mouth is covered by a small papilla. The mass of the two submandibular glands are the half of parotid can be find between the corpus mandible and m. mylohyoideus, produce mucinous saliva its get into the mouth beside of frenum linguae. Smallest the sublingual salivary gland produce mixed saliva, and get into the mouth by the Caruncula, more than one. Examination of salivary glands The parotis is cowered by the ramus mandibulae, by this way it can be palpate behind the bone. If there are any swelling or pain must be differentiate from masseter or TMJ diseases. If we press the skin over the ducts the secretion can help in the diagnosis. Volumetric saliva quantitation (sialometry) Measurable the resting and stimulated saliva quantity, and also the parotid saliva (CarlsonCrittenden cap). All big salivary glands are canulable. It was shown out that 50% decline of saliva can cause xerostomia. The quantity of resting saliva 0.3 ml/min. the stimulated saliva 1.2 ml/min. Salivary gland examinations X-ray: Salivary gland stone can shown by this method. Sialography: Salivary duct system become visible by this method (Söjgren,s syndrome, salivary gland stones). Scintigraphy: The salivary glands concentrate isotopes (ex.. 99Tcm). Ultrasound, MRI. Sialochemistry, Biopsy There are many diseases in which worthy to study the chemical constituents of the saliva. Measurable: drug, hormone, antibody level, sodium, potassium, calcium, although the diagnostic value rather small. Small salivary gland biopsy can be use for the diagnosis of Sjögren’s syndrome. Diseases of the Salivary Glands Sialoadenitis More frequent as a result of bacterial or viral infections, than as a result of allergy or irradiation. The salivary flow decrease. Mainly the big salivary glands are affected, but in small glands also occur. (nicotinic palatal stomatitis). Epidemic Parotitis MUMPS Caused by an RNA (paramyxovirus), most frequently parotid glands are affected. Beside of salivary gland pain stomach pain also develops accompanied by fever, epididimitis, orchitis and the submandibular gland could be affected. After healing lifelong immunity develop. Epidemic infections evolve. Therapy: symptomatic. Sialoadentitis Other virus also can cause inflammation in the salivary glands (cytomegalovirus, Coxakie). The bacterial infections are frequently caused by the stricture of the duct (ex.. stone). In this form an only gland is affected (the swelling is painful) and radiate to the temporal region. The aperture reddish and swollen. Predisposing factor of sialadenitis decrease the quantity of saliva. It helps the ascending infections from the oral cavity to the salivary glands. There are swollen lymph nodes in the neck. Therapy: Antibiotics (if it is possible after culture). Sialosis Sialoadenosis is a nonpainful, non-tumor-like salivary gland swollen. Could be cause by a lot of drug (antirheumatic, iodine containing and adrenergic activators). In generally reversible. Frequently develop as a complication of hormonal diseases: diabetes, acromegaly, but chronic alcohol consumption too. Diagnosis: labor test and biopsy. Necrotising Sialometaplasia A seldom, tumor-like disease develops rather in men and smokers. It is a problem of the palatal, small salivary glands vasculature (infarction of salivary glands). Histology: keratinized epithelial metaplasia and pseudoepithelioma in the ducts. Heal spontaneously in 8 weeks. Necrotizáló sialometaplasia NECROTIZÁLÓ SIALOMETAPLASIA Salivary gland swelling and tumors The swelling associate mainly to sarcoidosis and HIV infection. The tumors include the total sphere of benign and malignant tumors. Diseases as a result of changing saliva quantity Xerostomia: Xerostomia is a subjective sense, caused by the salivary gland hypofunction. Salivary deficiency can be caused by the decrease of salivary gland mass, the lesion of secretory neuron innervation, some drugs and general medicine diseases. Xerostomia patients must be follow for a long period of time, because it could be a sign of serious systemic diseases (ex.. irradiation of head and neck malignant tumors). Most frequently: drug Sid effect, which is in most cases reversible. Saliva quantitation Symptoms of xerostomia: Thirst, complication in the mastication of dry meals, problem in the denture stabilization, to force the patients to drink. The main complaints are: burning mouth, taste disorder. The lip is scaled. Questions for salivary gland hypofunction Management of xerostomy and salivary gland hypofunction The treatment depends on the severity of xerostomy or the affection of salivary glands. Where: there is saliva production: xlilitol, where it is very low: pilocarpin or other parasympatomymetic material, but where there is no functioning salivary gland not worth the drug treatment. Renewal of saliva with any plastic material ameliorate the patients subjective complaints. These materials contain: carboxicellulose and mucin, some contains fluoride for prevention of caries. If the xerosotmia patients have had teeth follow him/her monthly. Alcohol containing rinsing material forbidden. Sögren,s syndrome SJÖGREN SYNDROMA SJÖGREN SYNDROMA FÉLOLDALI PAROTIDECTOMIA UTÁN Autoimmune disease of the exocrine glands mainly in the salivary and lachrymal glands. Autoantibodies are produced against the acetylcholine receptors of the glandular cells, but autoantibodies against striated duct also has been found. Until the glandular tissue seems to be health, it means a good prognosis, when impair the prognosis become worsen. In the primary form (SSA) the salivary and lachrymal glands are affected, if it is combined with an other connective tissue diseases (SLE, RA) it is the secondary form (SSB). It is a disease mainly in females about 40 years. Their frequency in England 1-3%. Swelling of the salivary glands are painful in inflammation, and non painful in Sjögren,s syndrome. Keratoconjunctivitis sicca in the eye. Possible the Non-Hodgkin disease. Diagnosis Sialomatry, scintigraphy with 99Tcm, autoradiography can help, sometimes small salivary gland biopsy or MRI need for diagnosis. There are a lot of techniques with high specificity, but low sensitivity. Labortests Increased immunoglobulin levels, positive RF, ANA, SSA and SSB autoantibodies. Exclusion of other diseases (ex.. diabetes), blood picture, endocrine examinations. Schirmer test: over 5 mm/5 min. Therapy There is no adequate treatment schedule, but the symptoms are well controllable. There are Sjögren,s syndrome patients helping groups, which can give good advices to the patients. Overproduction of saliva Its name: sialorrchea or ptyalinism really seldom. Two main cause: hypersecretion and neuromuscular dysfunction. Frequent complaints of new denture bearing patients. In erosive oral diseases and in tumors the saliva production also increase. Cholinesterase also increase the saliva production. Therapy: stop the cause, and Atropine.