Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
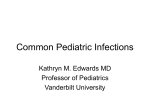
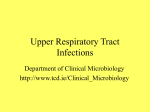
Respiratory Infection Ali Somily MD, FRCPC OUTLINE Resp Tract URT LRT Upper Respiratory Tract Infections Etiologies Acute pharyngitis Bacterial – Streptococcal (GAS) • Main • Most common bacterial – Diphtheria • Rare – N. gonorrhoeae, – B. pertussis Viral • Most common EBV Adenopathy Adenovirus & EBV GAS How to collect throat swab ? How to send it to the lab ? Bacterial –Swab GAS Viral –VTM What is the diagnosis Neck X-rays Anatomy Paranasal Sinuses Sinusitis What is sinusitis? An acute inflammatory process involving one or more of the paranasal sinuses. 5%-10% of URIs in children. Maxillary and ethmoid sinuses are most frequently involved. Acute & Chronic Sinusitis Acute Sinusitis >10 days but < 30 days. Subacute sinusitis >30 days without improvement. Chronic sinusitis >120 days. Etiology of Sinusitis 70% of bacterial sinusitis is caused by: Streptococcus pneumoniae Haemophilus influenzae Moraxella catarrhalis Clinical Presentations of Sinusitis Periorbital edema Cellulitis Nasal mucosa is reddened or swollen Percussion or palpation tenderness over a sinus Nasal discharge, thick, sometimes yellow or green Postnasal discharge in posterior pharynx Difficult transillumination Swelling of turbinates Boggy pale turbinates Pale, Boggy Turbinates Diagnostic Tests Radiographs Ultrasonograms CT scanning Laboratory studies, such as culture of sinus puncture aspirates. Pharmacological Plan of Care Clarithromycin:15mg/kg/d in 2 divided doses(>30kg, 250mg q12) OTITIS MEDIA Definition: Presence of a middle ear infection Acute Otitis Media: occurrence of bacterial infection within the middle ear cavity. Otitis Media with Effusion: presence of nonpurulent fluid within the middle ear cavity Normal & abnormal tympanic membrane MICROBES Streptococcus pneumoniae Haemophilus influenzae(non-typeable) Moraxella catarrhalis Group A Streptococcus Staph aureus Pseudomonas aeruginosa RSV assoc. with Acute Otitis Media PATHOGENESIS Otitis Media usually follows an URI in which there is edema of the eustacian tube, leading to blockage. Other factors: allergic rhinitis, nasal polyps, adenoidal hypertrophy Diagnosis Diagnostic tympanocentesis & myringotomy TREATMENT Amoxicillin: 20-40 mg/kg/day tid for 10-14 days or, Augmentin: 45 mg/kg/day po bid for 10-14 days NASOPHARYNGEAL CULTURES Carrier of – Streptococcus pyogenes, – Corynebacterium diphtheriae – Neisseria meningitidis Limited Practical Value – Otitis Media – Sinusitis For isolation of – Bordetella pertussis – Viral Lower respiratory tract infection Lung Anatomy Classification Typical Pneumonia 2. Atypical Pneumonia 1. According to the following 1. 2. 3. 4. 5. Organisms Treatment Presentation X-rays Prognosis Etiology No agent isolated in 40 to 60% of cases Culture sensitivity (50%) of sputum culture for S. pneumoniae, Agents of pneumonia are difficult to grow – Legionella, – Chlamydia pneumoniae, – Mycoplasma pneumoniae). C. pneumoniae – Second most common cause of pneumonia M. pneumoniae – Most cases of ambulatory CAP (serologic methods) Haemophilus influenzae and Legionella – The third and fourth most common bacterial causes of CAP requiring hospitalization. Specimens are easily contaminated with upper respiratory secretions, S.pneumo Pneumonia Staph.aureus Lung abscess. Pneumatocele and abscess Transplant and CMV Hematological malignancy and Asp lobar pneumonia Primarily caused by – – – – Streptococcus pneumoniae, Legionella pneumophila. Klebsiella pneumoniae, "currant jelly" sputum tissue damage and hemorrhage into the alveoli Escherichia coli – Often complicated by empyema and septicemia. Pseudomonas aeruginosa Serratia marcescens – Associated with a severe necrotizing pneumonia in immunosuppressed patients S.pneumoniae Lung abscesses Anaerobes Staphylococcus aureus Mycobacterium tuberculosis Mycoplasma pneumoniae Fungus Specimens A. Acceptable specimens 1. Sputum 2. Trachael and transtracheal aspirates 3. Bronchial washings, bronchial alveolar lavage, bronchial brushes, and bronchial biopsy 4. Lung aspirate and lung biopsy B. Unacceptable specimens 1. Saliva submitted as sputum 2. Twenty-four-hour sputum collection . 3. Swabs A. Media •1. BAP •2. MAC •3. CHOC •4. Broth-BHI or THIO Anaerobs Invasive procedure Processed as rapidly as possible. Collected and transported anaerobically Cultured for anaerobes. Transtracheal aspiration Transbronchial biopsy Protected bronchial brushes Bronchalveolar Protected bronchoscopy brush send for quantitative culture – Quantitative culture: Plate 10 µL. – Vortex the brush in 1 ml of BHI or steril saline Sputum Specimens Teeth brush – Contamination one log less Mouthwash – Avoid antiseptic Early morning – Pooled overnight secretions – Discouraged 24 hr collection – Contamination – Dilution Induced sputum Sterile wide-mouth jar – tightly fitted screwcap lid – press the rim of the container under the lower lip Translaryngeal (Transtracheal) Aspiration 1. The patient is debilitated 2.Routine sputum samples have failed to recover a causative organism in the face of clinical bacterial pneumonia. 3. An anaerobic pulmonary infection is suspected. Bronchoalveolar Lavage Injection of 30 to 50 mL The saline is then aspirated and submitted for smear preparation and culture The semiquantitative cultures >103 /mL that demonstrate intracellular bacteria in more than 25% of the inflammatory cells are indicators of pneumonia that requires specific treatment. Other Tests Blood cultures – Streptococcus pneumoniae 25% to 30% Direct fluorescent antibody tests Various Staining – – – – Pneumocystis carinii The tissue forms of various fungi Mycobacteria Viral inclusions Serological tests V. MICROSCOPIC A. Smear preparation B. Microscopic screening (sputum specimens only) Legionella Legionnaires' disease Story In the summer of 1976, public attention was focused on an outbreak of severe pneumonia that caused many deaths in members of the American Legion convention in Philadelphia. 231 people within a short time, and 34 of them died After months of intensive investigations, a previously unknown gram-negative bacillus was isolated. Subsequent studies found this organism, named Legionella pneumophila, to be the cause of multple epidemic and sporadic infections. The organism was previously not known to exist, because it stains poorly with conventional dyes and does not grow on common laboratory media. Despite the initial problems with the isolation of Legionella organisms, it is now recognized to be a ubiquitous aquatic saprophyte. Pneumophila means "love of the lungs" and Philadelphia means "city of brotherly love", 200 - 216 South Broad Street - Bellevue - Stratford Hotel (Fairmont Hotel) (1400 Walnut Street)] Taxonomy Taxonomic studies have shown that the family Legionellaceae – One genus, Legionella, • 39 species – > 60 serogroups. (Approximately half of these species and serogroups have been implicated in human disease, with the others found in environmental sources. ) L. pneumophila is the cause of almost 85% of all infections; – serotypes 1 is the most commonly isolated Physiology and Structure Slender, pleomorphic, gram-negative bacilli. Stains poorly with common reagents. Nutritionally fastidious with requirement for L-cysteine and enhanced growth with iron salts. Nonfermentative. Virulence Capable of replication in alveolar macrophages (and amoeba 'in nature). Prevents phagolysosome fusion. They enter the cell by – C3b and mem.protein – CR3 and bacterial surface – Endocytosis to Macro and Mono comp receptor Epidemiology Capable of sporadic and epidemic disease. Commonly found in natural bodies of water, cooling towers, condensers, and water systems (including hospital systems). Summer and autumn Estimated to be between 10,000 and 20,000 cases in United States annually. Patients at high risk for symptomatic disease include patients with compromised pulmonary function and patients with decreased cellular immunity (particularly transplant patients). Presentations Diseases – Legionnaires' disease. – Pontiac fever. Diagnosis – Culture on BCYE agar is the diagnostic test of choice but positive titers develop late in the course of disease. Gram stain of Legionella pneumophila grown on buffered charcoal-yeast extract agar Legionella species may appear as characteristic ground-glass colonies with iridescent edges, which is typical of L. pneumophila. Non-pneumophila species may appear as mucoid protuberant colonies (C) or raised greyish white colonies (D). The colonies of certain species of Legionella autofluoresce either blue-white (E) or red (F) under long-wavelength UV light. Immunofluorescent staining of either respiratory specimens or culture isolates should reveal short coccobacilli that stain a bright (3 to 4+) apple green Direct fluorescent antibody stain of Legionella micdadei. Treatment, Control, and Prevention Severe disease treated with azithromycin or levofloxacin; less severe disease can be treated with erythromycin or tetracycline. Rifampin can be added in sever cases Decrease environmental exposure to reduce risk of disease. For environmental sources associated with disease, treat with hyperchlorination, superheating, or copper-silver ionization