Survey
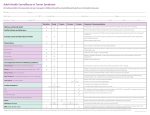
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
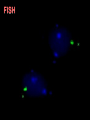
45 X Karyotype syndrome. Bonnevie-Ullrich syndrome. Gonadal dysgenesis. Monosomy X. Henry Turner, 1938 Ford et al., 1959 1 in 2,000 live-born female infants. 15% of spontaneous abortions have a 45,X0 Karyotype. In Sudan ? Race No racial or ethnic predilections. Genetic mechanisms 1. Absence of one copy of X chromosome. Paternal loss in 62% Maternal in 48% 2. Patient with Mosaic karyotype. Ex. 46,XX/45,X 3. Structural rearrangement result in loss of Xp material. Ex. 46,iX(Xq) 4. Loss of the SHOX gene. Variety of Turner syndrome. 45, X0 – Turner syndromes 99% of cases – aborted Total fetal hydrops 1 in 2,500 or 1 in 2,000 liveborn females. normal intelligence; may have 3D spatial problems or math problems. http://www.gfmer.ch/Genetic_diseases/Turner_syndrome/Turner.htm Web of skin Aorta Breast development Under- developed ovaries Phenotype 95% of adult with Turner syndrome exhibit short stature and infertility. 94% of patients are infertile Pregnancy has been achieved by: 1. Fresh embryo. 2. Frozen embryo transfer. Delivery by caesarean section is related to small pelvic outlet size. Ovarian failure primary amenorrohoae. Undeveloped breast. 45,X[6]/46XX [80] Patients may present with Ambiguous genitalia Age 7 month Sex Male Diagnosis Intersex Examination Big phallus, Labia major. Small L. minora. Blind vagina. Male urethra. Ultrasound NO uterus. Testes could be identified. 46,X,del(X)(p11)[11]. Low hairline. Shield-shaped chest. Narrow hip development. . Lymphedema May be present at any age. It is the cause of the webbed neck and low posterior hairline. In infants, the combination of dysplastic or hypoplastic nails and lymphedema gives a characteristic sausage-like appearance to the fingers and toes. Lymphedema The toes have the characteristic sausage-like appearance Generalized lymphedema. Loose skin folds around the neck will form a webbed neck later in life Hyperconvex nails in Turner syndrome note U-shaped cross section Mortality and morbidity Mortality Is high due to: 1. Coarctation of the aorta. 2. Cardiovascular disease. 3. Obesity, associated diabetes and hypertension. 4. Osteoporosis. Life expectancy is reduced by 10 years. Morbidity Individuals with mitral or aortic valve disease require prophylaxis for sub acute bacterial endocarditis (SBE). 35% of patients have renal anomalies. Ultrasound evaluation at the diagnosis. Yearly urine culture. BUN, and creatinine. Girls with horseshoe kidneys: Have an increased risk of Wilms tumor. Should have renal ultrasound examinations: Every 5 months until the age of 8 years. Every 6-12 months thereafter. Hearing assessment At birth At 1 year-age. Before entering school. At adulthood. A cardiologist should evaluate patients at diagnosis. 1. Risks of aortic root dilatation. 2. Risks of Aortic dissection. Complete cardiovascular evaluation For all patients prior to attempting assisted reproduction or conception. Supplement with: 1. Growth hormone. 2. Estrogens. 3. progestins. Attention should be paid to: 1. Growth and development, 2. Thyroid status 3. Osteoporosis. Patients on growth hormone should be seen every 3-4 months. Other Gastrointestinal bleeding: Hip dislocation: Scoliosis in 10% of adolescent girls with Turner syndrome. Thyroid: 10-30% develop hypothyroidism. Should be considered in Individuals with : Primary or secondary amenorrhea. Adult women with unexplained infertility Unexplained short stature. Turner syndrome may be diagnosed prenatally by: 1. Amniocentesis. 2. Chorionic villous sampling. The clinical suspicion Cytogenetic analysis 45,X. 45, X/46, XX. 46,XX,del(X)(P10). FISH analysis. Cytogenetic analysis of fibroblas in case of normal karyotype 46,XX. FISH 45, X0 – Turner syndromes Short Stature (approximately 4 feet 8 inches) –; loss of action SHOX gene on the X-chromosome. treated by growth hormone No ovarian function or early loss of function (in late teens) estrogen-progesterone treatment to maintain secondary sexual development Coarctation of the aorta (narrow aorta) 10-15% Corrected surgically Kidney problem (Horseshoe kidney) high blood pressure Medical Care In childhood Growth hormone therapy is standard to prevent short stature as an adult. Cecilia takes her daily growth hormone injection "My name is Regina and I’m 9 years old. I felt that taking my growth hormone injection was a bit difficult in the beginning, but I practiced with an orange and after a while I found out how to do it, and now it’s just a habit like brushing your teeth." Estrogen replacement Therapy is required, but starting too early can compromise adult height. Estrogen usually is started from age 12-15 years. Keloid formation Turner syndrome individuals exhibits high risk of keloid formation. Subacute bacterial endocarditis Prophylaxis is required prior to and dental or surgical procedure in women with cardiac valve disease, to prevent subacute bacterial endocarditis. Before After surgery Ovarian failure are risk factors for osteoporosis thus adequate daily intake of calcium (1.0-1.5 g) and vitamin D (at least 400 IU) should consider. Patients with short stature require fewer calories than those of normal height. Genetics counseling Turner syndrome is not an inherited disorder, and the recurrence risk is low. Due to infertility, it is rarely passed to offspring. Consultation with a geneticist 1. Suspected mosaicism for all, or part 2. Virilization with part of Y chromosome. Overall prognosis is good. Even with growth hormone therapy, most individuals will be shorter than average. Turner syndrome is not a cause of mental retardation. Life expectancy is slightly shorter. Almost all individuals will be infertile, but pregnancy with donor embryos is possible. Yearly follow-up TSH tests will help avoid unrecognized hypothyroidism, which can interfere with growth. Osteoporosis and aortic arch dissection are known complications in adulthood. Dosage Compensation Shouldn’t XX females produce twice the amount of X-linked gene products (proteins) as XY males? No, because XX females “compensate” by inactivating one of their X chromosomes to make a single “dosage” of X-linked genes. Barr Bodies are inactivated X chromosomes in Females Normal male, Turner female 0 1 2 3 Normal female, Klinefelter male # Barr bodies= N-1 rule Inconsistencies between syndromes and X inactivation If normal XX female has one X inactivated, why is a X Turner female not normal? Similarly, if XXY male has one X inactivated, why does he have Klinefelter syndrome? Perhaps not complete inactivation or inactivation does not happen immediately, Then some overexpression of X-linked genes The Lyon Hypothesis of X Inactivation Proposed by Mary Lyon and Liane Russell (1961) Which X is inactivated? Inactivation of X chromosome occurs randomly in somatic cells during embryogenesis Progeny of cells all have same inactivated X chromosome as original, creating mosaic individual Lyon-Hypothesis: X-inactivation A precursor cell to all coat color cells Random inactivation early in dev. **Also in calico cats X chromosome inactivation • X chromosome has many more genes than the Y chromosome • Females have 2 Xs One X must be inactivated to preserve gene dosage Inactive Xs condense to form Barr bodies during development Inactivation is random during development Barr bodies in female cells Color pattern seen in female calico cats due to random X chromosome inactivation Mosaicism Reveals the Random Inactivation of one X chromosome Anhidrotic ectodermal dysplasia in a heterozygous woman Regions where sweat glands are absent.